Metatarsophalangeal Joint Arthrodesis: Key Techniques for Success
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Metatarsophalangeal Joint Arthrodesis: Key Techniques for Success. Metatarsophalangeal joint arthrodesis is a surgical procedure fusing the first MTP joint to treat severe arthrosis, including advanced hallux rigidus, rheumatoid disease, and gout. It is indicated when conservative pain management fails. This procedure aims to alleviate pain and improve function by stabilizing the joint, often being the treatment of choice for advanced cases.
Introduction and Epidemiology
Arthrosis of the first metatarsophalangeal joint is a highly prevalent condition encountered in orthopedic foot and ankle surgery, commonly presenting as primary osteoarthritis (hallux rigidus), secondary osteoarthritis, or in the setting of systemic inflammatory arthritides such as rheumatoid disease, gout, and psoriatic arthritis. The primary indication for surgical intervention of the first metatarsophalangeal joint is recalcitrant pain that has failed comprehensive conservative management. Arthrodesis of the first metatarsophalangeal joint remains the gold standard surgical treatment of choice in rheumatoid disease and is the definitive indicated procedure in hallux rigidus when the degenerative disease is advanced (Coughlin and Shurnas Grade 3 or 4).
Primary osteoarthritis and inflammatory arthritides account for the vast majority of causative factors. Secondary osteoarthritis typically arises from mechanical abnormalities, including severe hallux valgus, hallux varus, and prior trauma resulting in joint incongruity, intra-articular fractures, and excessive cartilage wear. The natural history of first metatarsophalangeal joint arthrosis is intrinsically related to its etiology. Hallux rigidus is a progressive disease process; the joint will inevitably deteriorate radiographically over time, although the patient's subjective clinical symptoms may not always demonstrate a perfectly linear correlation with radiographic deterioration. Progression of arthrosis secondary to inflammatory arthritides will be closely related to the systemic activity and medical management of the underlying disease.
In true hallux rigidus, patients characteristically experience an insidious onset of pain, swelling, and stiffness in the first metatarsophalangeal joint that is exacerbated by weight-bearing activities such as walking and running. Lateral forefoot pain due to mechanical overload frequently develops as the foot supinates to avoid painful dorsiflexion of the first ray just before and immediately after heel rise during the gait cycle.
A comprehensive physical examination is required to enable accurate diagnosis and selection of the correct surgical procedure. The physician should palpate the metatarsophalangeal joint for localized tenderness; dorsal or dorsolateral osteophytes (cheilus) are typically palpable and tender. The physician must examine the range of motion of both the metatarsophalangeal and interphalangeal joints. Restriction in dorsiflexion but full plantarflexion may indicate that a dorsal closing wedge osteotomy of the proximal phalanx (Moberg procedure) or a cheilectomy may improve the functional dorsiflexion arc in early-stage disease. However, the grind test is not normally painful unless an osteochondral defect is present or degeneration is advanced. If the grind test is acutely painful, arthrodesis is the indicated procedure.
The physician should observe the patient's walking gait. Avoidance of weight bearing on the hallux implies significant joint pain, and transfer lesions or adventitial callus may be present under the lesser metatarsal heads. The physician must palpate for posterior tibial and dorsalis pedis pulses. Peripheral vascular disease is a strict contraindication to elective foot surgery; if suspected, formal non-invasive vascular assessment and optimization are required prior to any surgical consideration. Furthermore, the physician should palpate and move the tarsometatarsal joint. A thorough assessment of first ray mobility is required to rule out concomitant tarsometatarsal hypermobility or arthrosis, which may necessitate a Lapidus procedure rather than, or in addition to, an isolated metatarsophalangeal arthrodesis.
Surgical Anatomy and Biomechanics
Osseous and Articular Anatomy
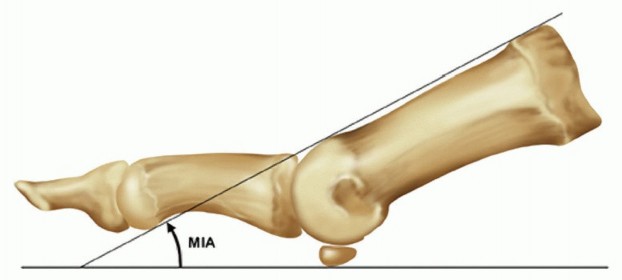
The first metatarsophalangeal joint is anatomically classified as a ball-and-socket joint, though its kinematics are highly complex, involving sliding, rolling, and compression forces. The normal hallux valgus angle is less than 15 degrees. The metatarsal inclination angle relative to the weight-bearing surface is usually 25 to 30 degrees but varies significantly with intrinsic foot morphology, being greater in a cavus foot type and less in a planus foot type.

The articular surfaces consist of the convex first metatarsal head and the concave base of the proximal phalanx. The plantar aspect of the metatarsal head features two longitudinal grooves separated by a central crest (crista), which articulate with the medial (tibial) and lateral (fibular) sesamoids. The sesamoid complex is embedded within the tendons of the flexor hallucis brevis and is critical for the mechanical advantage of the intrinsic flexors.

Biomechanics of the First Ray
The final position of the arthrodesed first metatarsophalangeal joint must precisely allow for heel rise during the late stance phase of gait. During normal locomotion, the first metatarsophalangeal joint must dorsiflex to engage the windlass mechanism, tightening the plantar fascia and stabilizing the longitudinal arch. When the joint is fused, this motion is eliminated, and the interphalangeal joint must compensate.

The position can be evaluated intraoperatively by applying a flat, rigid surface (such as a sterile tray or osteotome) to the plantar aspect of the foot, simulating weight bearing. The tip of the toe should clear the surface by approximately 2 to 5 millimeters with the interphalangeal joint in full extension, and the pulp of the toe should firmly touch the surface with the interphalangeal joint in 45 to 60 degrees of flexion. Failure to achieve this precise alignment results in significant gait dysfunction. Excessive dorsiflexion transfers stress to the lesser metatarsals and causes dorsal shoe impingement, while excessive plantarflexion causes vaulting, retrograde interphalangeal joint arthritis, and severe limitations in terminal stance.
Indications and Contraindications
Patient selection is paramount for achieving high satisfaction rates following first metatarsophalangeal joint arthrodesis. The procedure is highly reliable for eliminating pain and providing a stable medial column, but patients must be counseled regarding the permanent loss of joint motion and the necessity for shoe wear modifications (e.g., avoidance of high-heeled footwear).

| Indication Category | Specific Clinical Scenarios |
|---|---|
| Operative Indications | Advanced Hallux Rigidus (Coughlin/Shurnas Grade 3 or 4) |
| Severe Hallux Valgus (especially with concurrent degenerative changes) | |
| Rheumatoid Arthritis or other inflammatory arthritides | |
| Salvage of failed prior procedures (e.g., failed Keller arthroplasty, failed silastic or metallic implant arthroplasty, failed prior osteotomy) | |
| Neuromuscular instability (e.g., cerebral palsy, Charcot-Marie-Tooth) | |
| Post-traumatic arthrosis or intra-articular fracture malunion | |
| Non-Operative Indications | Mild to moderate Hallux Rigidus (Grades 1 and 2) responsive to rigid orthotics |
| Patient unwilling to accept loss of metatarsophalangeal joint motion | |
| Medically unstable patients unfit for elective anesthesia | |
| Active local or systemic infection | |
| Severe peripheral vascular disease with inadequate distal perfusion | |
| Poor soft tissue envelope precluding safe surgical exposure |
Pre Operative Planning and Patient Positioning
Clinical and Radiographic Assessment
Preoperative planning begins with standard weight-bearing radiographs of the foot, including anteroposterior, lateral, and sesamoid axial views. These images are evaluated for the extent of joint destruction, subchondral sclerosis, osteophyte formation, and any underlying deformity such as metatarsus primus varus or hallux valgus.

In cases of revision surgery or salvage of a failed implant arthroplasty, severe bone loss is often encountered. Radiographic templating is necessary to determine if structural autograft (e.g., from the iliac crest) or structural allograft will be required to restore the length of the first ray and maintain the normal metatarsal parabola. Shortening of the first ray by more than 5 to 8 millimeters can lead to devastating transfer metatarsalgia.
Positioning and Setup
The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the lower extremity to a neutral position, ensuring the patella and the foot are pointing directly towards the ceiling. This neutral alignment is critical for intraoperative assessment of rotation and valgus during the fixation phase. A pneumatic tourniquet is typically placed on the thigh or calf, depending on surgeon preference and patient vascular status, and inflated after exsanguination with an Esmarch bandage. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Detailed Surgical Approach and Technique
Surgical Exposure
A dorsal longitudinal incision is the most common and versatile approach for first metatarsophalangeal joint arthrodesis. The incision extends from the mid-shaft of the proximal phalanx to the distal third of the first metatarsal, positioned just medial to the extensor hallucis longus tendon.

Sharp dissection is carried through the skin, and careful blunt dissection is utilized to identify and protect the branches of the superficial peroneal nerve (specifically the dorsal medial cutaneous nerve) and the proper digital nerve. The extensor hallucis longus tendon is retracted laterally, and the extensor hallucis brevis tendon may be tenotomized if severe contracture is present. A longitudinal capsulotomy is performed, and full-thickness subperiosteal flaps are elevated medially and laterally to expose the metatarsal head and the base of the proximal phalanx. Collateral ligaments and the plantar plate attachments are released to allow complete plantarflexion of the proximal phalanx, providing unhindered access to the articular surfaces. Dorsal osteophytes are excised using a rongeur or sagittal saw to facilitate joint preparation.
Joint Preparation Strategies
Many techniques in the preparation of the joint exist to provide the requisite good cancellous apposition necessary for primary bone healing. The choice of preparation technique dictates the degree of shortening and the ease of intraoperative positional adjustment.
Flat cuts: Using a sagittal saw to create flat planar cuts on the metatarsal head and phalangeal base provides excellent cancellous bone contact and inherent rotational stability. However, these make accurate positioning of the toe exceedingly difficult, as any required alteration in sagittal or coronal alignment requires a secondary wedge resection, leading to progressive and often unacceptable shortening of the first ray.
Cone or peg socket: This technique involves shaping the metatarsal head into a conical peg and reaming a matching socket into the proximal phalanx. While it provides excellent intrinsic stability, this leads to excessive shortening and is generally reserved for specific revision scenarios.
Ball and socket: This is currently the most widely accepted and utilized technique. It results in minimal shortening and has the additional benefit of ease of adjustment in positioning the toe in all three planes prior to definitive fixation.

To execute the ball and socket preparation, specialized hemispherical reamers are employed. A guide pin is placed centrally within the metatarsal head, parallel to the metatarsal shaft. A concave (cup) reamer is used to denude the cartilage and subchondral bone from the metatarsal head. Subsequently, a guide pin is placed centrally in the base of the proximal phalanx, and a convex (cone) reamer is utilized to prepare the reciprocal socket.

Reaming must be performed judiciously, frequently irrigating to prevent thermal necrosis, and stopping as soon as bleeding, healthy cancellous bone is exposed across the entire articular footprint. The subchondral plate must be adequately breached to allow for cellular migration and osteogenesis. If dense sclerotic bone remains, it should be aggressively fenestrated with a 2.0-millimeter drill bit or a small osteotome ("fish-scaling") to stimulate an inflammatory healing response.
Arthrodesis Alignment
Accurate spatial alignment of the arthrodesis is the single most critical determinant of a successful clinical outcome. The joint must be positioned in three planes:
- Sagittal Plane (Dorsiflexion): The proximal phalanx should be positioned in approximately 10 to 15 degrees of dorsiflexion relative to the floor, which corresponds to approximately 20 to 25 degrees of dorsiflexion relative to the longitudinal axis of the first metatarsal (accounting for the normal metatarsal declination angle).
- Transverse Plane (Valgus): The hallux should be placed in 10 to 15 degrees of valgus, ensuring it rests parallel to the second toe without impinging upon it.
- Coronal Plane (Rotation): The toenail should be facing directly dorsal, in neutral rotation. Any pronation or supination will lead to painful callosities along the borders of the interphalangeal joint.

Intraoperative fluoroscopy and the simulated weight-bearing test (using a flat plate against the plantar foot) are mandatory to confirm alignment before definitive fixation.
Fixation Constructs
Various methods of fixation have been described in the literature, including crossed Kirschner wires, crossed compression screws, intramedullary devices, and plate-screw constructs. The most biomechanically advantageous method of fixation has been definitively shown to be a dorsal low-profile neutralization plate combined with an interfragmentary compression screw.

The interfragmentary lag screw is typically placed first. A 3.5-millimeter or 4.0-millimeter cannulated or non-cannulated screw is directed either from the medial-distal aspect of the proximal phalanx into the lateral-proximal metatarsal head, or from dorsal-proximal to plantar-distal. This screw provides rigid static compression across the prepared cancellous surfaces.

Following lag screw placement, a dorsal titanium or stainless steel plate is applied. The plate functions as a tension band. During the terminal stance phase of gait, ground reaction forces attempt to dorsiflex the hallux, placing the plantar aspect of the arthrodesis under tension and the dorsal aspect under compression. The dorsal plate neutralizes these tensile forces, protecting the lag screw and providing exceptional construct rigidity. Modern locking plates offer additional stability, particularly in osteopenic bone frequently encountered in rheumatoid arthritis patients.
Once fixation is secured, the wound is thoroughly irrigated. The capsule and extensor retinaculum are repaired with absorbable suture to prevent tendon bowstringing. The subcutaneous tissues and skin are closed in a layered fashion, and a sterile compressive dressing is applied.
Complications and Management
Despite being a highly reliable procedure, first metatarsophalangeal joint arthrodesis carries specific risks. Understanding these complications and their salvage strategies is essential for the orthopedic surgeon.

| Complication | Incidence | Etiology / Risk Factors | Salvage and Management Strategies |
|---|---|---|---|
| Nonunion (Pseudoarthrosis) | 5% - 10% | Smoking, non-compliance with weight-bearing restrictions, inadequate joint preparation, poor fixation, infection, avascular necrosis. | Asymptomatic nonunions require no intervention. Symptomatic nonunions require revision arthrodesis with removal of hardware, aggressive debridement to bleeding bone, structural or cancellous bone grafting (autograft preferred), and rigid revision fixation (often with locking plates or intramedullary constructs). |
| Malunion (Sagittal Plane) | 5% - 15% | Intraoperative technical error, failure to simulate weight-bearing, shifting of hardware. | Excessive Dorsiflexion: Causes dorsal shoe impingement and transfer metatarsalgia. Requires dorsal closing wedge osteotomy through the fusion mass. Excessive Plantarflexion: Causes vaulting gait and IP joint arthritis. Requires plantar closing wedge osteotomy. |
| Malunion (Transverse Plane) | 5% - 10% | Failure to align parallel to the second toe. | Excessive Valgus: Causes impingement on the second toe (cross-over deformity). Requires medial closing wedge osteotomy. Excessive Varus: Causes medial shoe rub and IP joint degeneration. Requires lateral closing wedge osteotomy. |
| Hardware Prominence | 10% - 20% | Thin dorsal soft tissue envelope, prominent screw heads, bulky dorsal plates. | Conservative management with shoe modification. Operative management involves hardware removal once complete radiographic union is confirmed (typically after 6-12 months). |
| Interphalangeal Joint Degeneration | 15% - 30% (Long-term) | Compensatory hypermobility of the IP joint due to loss of MTP motion, exacerbated by malunion. | Conservative management with stiff-soled shoes or rocker-bottom modifications. Surgical intervention may require IP joint arthrodesis in severe, recalcitrant cases. |
| Infection | 1% - 3% | Patient comorbidities (diabetes, rheumatoid arthritis on immunosuppressants), prolonged operative time. | Superficial infections managed with oral antibiotics. Deep infections require prompt surgical irrigation and debridement, hardware removal if loose, culture-specific intravenous antibiotics, and eventual revision arthrodesis once the infection is eradicated. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must balance the mechanical protection of the arthrodesis construct with the prevention of disuse osteopenia and deep vein thrombosis. Protocols vary slightly based on patient bone quality and surgeon preference, but generally adhere to the following phased approach:
Phase 1: Immediate Postoperative Period (Weeks 0 to 2)
The patient is placed in a bulky compressive dressing and a rigid postoperative shoe or controlled ankle motion (CAM) boot. Weight-bearing is typically restricted to heel-touch only or strict non-weight-bearing with crutches or a knee scooter, depending on the rigidity of the fixation and bone quality. Elevation of the operative extremity above the level of the heart is strictly enforced to minimize edema and promote wound healing. Sutures are removed at approximately 14 days postoperatively once the incision is fully coapted.
Phase 2: Protected Weight Bearing (Weeks 2 to 6)
Following suture removal, the patient is transitioned to progressive weight-bearing as tolerated in a rigid-soled postoperative shoe or CAM boot. The rigid sole is critical as it prevents bending moments across the forefoot that could compromise the arthrodesis site. Patients are encouraged to perform active and passive range of motion exercises of the ankle and the interphalangeal joint of the hallux to prevent secondary stiffness.
Phase 3: Radiographic Consolidation and Transition (Weeks 6 to 12)
At the 6-week postoperative mark, weight-bearing radiographs (anteroposterior and lateral) are obtained to assess for bridging trabecular bone and maintenance of hardware integrity. If clinical and radiographic signs of union are present, the patient is gradually transitioned into supportive, stiff-soled athletic footwear. A rocker-bottom shoe modification may be highly beneficial during this phase to facilitate a normal heel-to-toe gait pattern without placing undue stress on the midfoot or the healing fusion mass.
Phase 4: Return to Normal Activity (Months 3 to 6)
As the fusion mass fully consolidates and remodels, patients may progressively return to higher-impact activities. High-heeled shoes and extremely flexible footwear are permanently discouraged. Maximum medical improvement and complete resolution of postoperative edema may take up to 9 to 12 months.
Summary of Key Literature and Guidelines
The academic consensus strongly supports first metatarsophalangeal joint arthrodesis as a highly durable and predictable procedure. Foundational studies by Coughlin and Shurnas established the clinical grading system for hallux rigidus and demonstrated that arthrodesis yields superior long-term patient satisfaction rates (exceeding 90%) compared to implant arthroplasty or extensive cheilectomy in advanced disease stages.
Biomechanical investigations have rigorously evaluated fixation constructs. Politi et al. and subsequent authors demonstrated that the combination of a dorsal neutralization plate with an interfragmentary compression screw provides significantly greater stiffness and load-to-failure characteristics compared to crossed screws or Kirschner wires. This construct minimizes micromotion at the arthrodesis site, thereby optimizing the biologic environment for primary bone healing and reducing the incidence of nonunion.
Furthermore, long-term outcome studies emphasize that while the theoretical loss of metatarsophalangeal joint motion alters the windlass mechanism, the clinical functional impairment is remarkably minimal if the arthrodesis is aligned correctly. Patients routinely return to recreational running, hiking, and strenuous occupational activities, underscoring the procedure's efficacy as the definitive treatment for end-stage first metatarsophalangeal joint pathology.
Clinical & Radiographic Imaging
You Might Also Like

