

Introduction and Epidemiology
Radial head fractures constitute a significant proportion of elbow injuries, representing 1.7% to 5.4% of all fractures and approximately one-third of all elbow fractures encountered in orthopedic practice. This prevalence underscores the importance of a comprehensive understanding of their diagnosis and management. The seemingly innocuous nature of some radial head fractures belies their potential for severe complications, particularly when associated with ligamentous or osseous injuries of the elbow, forearm, or wrist, collectively leading to chronic pain, instability, and functional impairment. Indeed, approximately one-third of patients present with concomitant injuries, which may include fractures or ligamentous damage of the shoulder, humerus, forearm, wrist, or hand. This complex injury pattern, frequently involving the ipsilateral upper extremity, necessitates a meticulous diagnostic approach and often multidisciplinary management strategies. The spectrum of radial head fractures ranges from simple, non-displaced fissures to highly comminuted fractures with significant articular disruption and associated elbow instability, demanding a tailored treatment approach based on the fracture characteristics, patient demographics, and functional requirements.
Surgical Anatomy and Biomechanics
The radial head is a crucial component of the elbow and forearm complex, contributing significantly to both articular motion and stability. Understanding its intricate anatomy and biomechanical role is paramount for effective treatment of its fractures.
Articular Configuration and Force Transmission
The proximal radius articulates with the capitellum of the humerus, forming the radiocapitellar joint, which is a key contributor to elbow flexion-extension and forearm rotation. The capitellum and the radial head are reciprocally curved, facilitating smooth articulation throughout the arc of motion. Force transmission across the radiocapitellar articulation occurs at all angles of elbow flexion and is most pronounced in full extension, where the radial head bears a substantial portion of the axial load. This inherent load-bearing capacity explains its vulnerability to axial compression injuries. The concave articular surface of the radial head accommodates the convex capitellum, and the integrity of this articulation is essential for normal elbow kinematics.
Forearm Rotation and Stability
Full rotation of the head of the radius, encompassing both supination and pronation, requires accurate anatomic positioning within the lesser sigmoid notch of the ulna. This articulation, stabilized by the annular ligament, forms the proximal radioulnar joint (PRUJ). Any incongruity or displacement of the radial head can significantly impair forearm rotation, leading to functional limitations.
Valgus and Longitudinal Stability
The radial head plays a critical role in the valgus stability of the elbow, although the precise degree of its contribution remains a subject of ongoing debate in biomechanical studies. It is widely recognized as a secondary restraint to valgus forces, with the primary restraint being the medial collateral ligament (MCL) complex. The radial head appears to function by shifting the center of varus-valgus rotation laterally, thereby reducing the moment arm and the forces exerted on the medial ligaments. Clinically, the radial head's contribution to valgus stability becomes most significant when there is injury to both the ligamentous and muscle-tendon units about the elbow, particularly in cases of MCL disruption. In such scenarios, the intact radial head provides crucial buttressing against valgus stress. Conversely, excision of the radial head in the presence of MCL insufficiency can lead to gross valgus instability.
The radial head also acts in concert with the interosseous ligament of the forearm to provide longitudinal stability between the radius and ulna. This robust ligamentous structure prevents proximal migration of the radius relative to the ulna. Disruption of the interosseous ligament, especially in conjunction with radial head excision or fracture, can lead to proximal migration of the radius, resulting in distal radioulnar joint (DRUJ) instability, positive ulnar variance, and carpal impingement syndromes (e.g., Essex-Lopresti injury complex).

The complex interplay of these structures highlights the radial head not merely as a bone, but as an integral component of the elbow’s stability and kinematic chain.
Neurovascular Considerations
Proximity of the radial head to neurovascular structures, particularly the posterior interosseous nerve (PIN), is critical. The PIN, a branch of the radial nerve, typically courses within the supinator muscle, approximately 3-4 cm distal to the radiocapitellar joint. Surgical approaches to the radial head must meticulously protect this nerve. The radial head receives its blood supply predominantly from branches of the radial recurrent artery, forming a rich periosteal network. Disruption of this network, especially with severe comminution or stripping, can compromise healing.
Mechanism of Injury and Classification
Radial head fractures predominantly result from a fall onto an outstretched hand (FOOSH), with the forearm in pronation and the elbow in slight flexion. Higher energy injuries, such as falls from significant heights or those occurring during sports activities, typically produce more complex fracture patterns.
Biomechanical Mechanisms
The radial head fractures when it impacts the capitellum under an axial load. This mechanism can occur in several scenarios:
* Pure Axial Load: Direct impaction of the radial head against the capitellum.
* Posterolateral Rotatory Force: Often associated with posterolateral rotatory instability, where the radial head dislocates posteriorly and impacts the capitellum.
* Associated Dislocations: As part of a posterior Monteggia fracture-dislocation (fracture of the ulna with dislocation of the radial head) or posterior olecranon fracture-dislocation.
Experimental biomechanical studies have further elucidated the relationship between elbow flexion angle and fracture patterns:
* Axial load at 0 to 35 degrees of elbow flexion tends to result in a coronoid fracture.
* Axial load at 0 to 80 degrees of elbow flexion more commonly leads to a radial head fracture.
These findings highlight the interdependence of elbow osseous structures in absorbing axial and valgus loads. It is frequently associated with injury to the ligaments, particularly the lateral ulnar collateral ligament (LUCL) complex, and other osseous structures, such as the coronoid process, creating complex injury patterns like the "terrible triad" of the elbow. The terrible triad involves a radial head fracture, coronoid fracture, and elbow dislocation (typically posterolateral).
Diagnostic Imaging
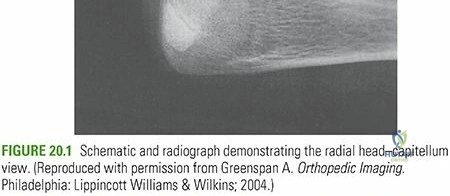
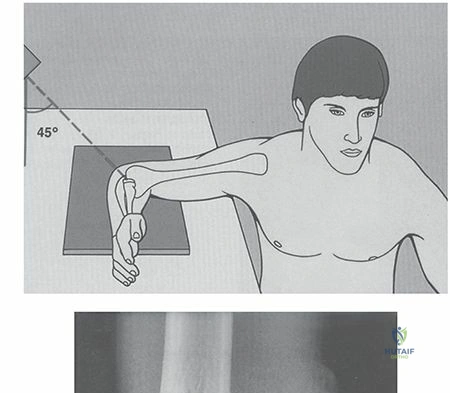
Diagnosis primarily relies on plain radiographs, including anteroposterior, lateral, and oblique views (Greenspan or radial head views). The presence of a posterior fat pad sign on a lateral radiograph is highly suggestive of an intra-articular injury, even if a fracture line is not clearly visible. The capitellar view (45 degrees lateral with 45 degrees pronation) can improve visualization of the radial head. Computed tomography (CT) scans are invaluable for assessing fracture comminution, articular step-off, depression, the presence of loose bodies, and associated coronoid or capitellar fractures. In cases of suspected ligamentous injury or occult fractures, magnetic resonance imaging (MRI) may be beneficial, although it is not typically part of the initial workup.
Classification Systems
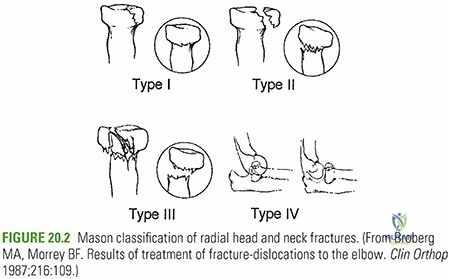
Accurate classification guides treatment decisions. The most widely adopted system is the Mason-Johnston classification, which categorizes radial head fractures based on displacement and comminution:
- Mason Type I: Non-displaced or minimally displaced (less than 2 mm displacement or angulation) partial articular fracture. No mechanical block to rotation.
- Mason Type II: Displaced (greater than 2 mm displacement or angulation) partial articular fracture. May involve a single large fragment. Mechanical block to rotation may be present.
- Mason Type III: Comminuted, displaced fracture involving the entire radial head. Often associated with significant articular depression and instability.
- Mason Type IV: (Hotchkiss modification) Any radial head fracture associated with an elbow dislocation. This type often represents a severe injury, frequently part of a terrible triad or an Essex-Lopresti injury.
Further modifications, such as the Hotchkiss modification for Type IV, and the AO/OTA classification, provide additional detail regarding fracture morphology and associated injuries, aiding in surgical planning.
Indications and Contraindications
The management of radial head fractures spans a spectrum from non-operative protocols to complex surgical reconstructions, dictated by fracture morphology, associated injuries, and patient factors. The primary goals are restoration of articular congruity, stability, and pain-free range of motion.
Indications for Operative vs. Non-Operative Management
| Parameter/Fracture Type | Non-Operative Indication | Operative Indication |
|---|---|---|
| Mason Type I | Minimally displaced (<2 mm), no mechanical block to rotation. | Rarely, if intractable pain or late mechanical symptoms develop. |
| Mason Type II | Displaced <2 mm, no mechanical block to rotation, stable elbow. | Displaced >2 mm, angulation >30 degrees, mechanical block to forearm rotation, or persistent pain with conservative management. |
| Mason Type III | Rarely, in very low-demand patients or with severe comorbidities precluding surgery. | Nearly always indicated for active patients. Open Reduction Internal Fixation (ORIF) if reconstructible; Radial Head Arthroplasty (RHA) or excision (rarely) if severely comminuted or irreparable. |
| Mason Type IV (with dislocation) | Never. Represents an unstable injury. | Always indicated. Requires reduction of dislocation, then management of radial head fracture (ORIF, RHA, or excision), and addressing associated ligamentous and coronoid injuries (e.g., terrible triad). |
| Associated Ligamentous Instability | Stable elbow after fracture reduction. | Any significant ligamentous disruption contributing to elbow instability (e.g., LCL tears, MCL tears), particularly in the context of Type III/IV fractures. |
| Mechanical Block to Rotation | None. | Any radial head fracture causing a block to forearm pronation/supination. |
| Essex-Lopresti Injury (proximal migration) | None. | Always indicated for reconstruction of the radial head (ORIF or RHA) and repair of the interosseous membrane/DRUJ stabilization. |
| Patient Factors | Low functional demand, significant comorbidities. | High functional demand, younger active patients. |
Contraindications
Absolute contraindications for operative management are rare and typically involve patient-specific factors such as:
* Active local or systemic infection: Increases risk of osteomyelitis and implant failure.
* Severe medical comorbidities: Patients unable to tolerate anesthesia or the surgical procedure.
* Extremely poor skin condition or soft tissue compromise: May preclude surgical incision and closure.
Relative contraindications may include:
* Pre-existing severe elbow arthritis: May temper expectations for functional recovery from fracture fixation alone.
* Severely osteoporotic bone: May compromise implant purchase, leading to fixation failure.
* Significantly delayed presentation: Chronic fractures may be more challenging to reduce and fix, sometimes necessitating different strategies.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is crucial for optimizing outcomes in radial head fracture management. This systematic approach ensures all potential complexities are anticipated and addressed.
Preoperative Assessment
- Clinical Examination: A detailed assessment of the entire upper extremity, including neurovascular status, range of motion (if pain permits), and assessment for associated injuries (e.g., tenderness over ligaments, DRUJ instability, ipsilateral wrist injuries). The presence of ecchymosis, swelling, and any deformity should be documented.
- Imaging Review: Beyond plain radiographs, a CT scan is almost universally indicated for Mason Type II, III, and IV fractures. This provides crucial information regarding comminution, articular step-off, depression, coronoid fracture patterns, and identification of loose bodies. 3D reconstructions can aid in visualizing fracture complexity. Review of the contralateral elbow radiographs can be helpful for assessing anatomical norms, especially for radial head replacement.
- Classification Confirmation: Re-evaluate and confirm the Mason-Johnston classification and any associated injuries (e.g., terrible triad, Essex-Lopresti) to guide the treatment strategy.
- Implant Selection: Based on fracture pattern, determine the feasibility of ORIF. If comminution is extensive or irreconstructible, plan for radial head arthroplasty (RHA). If RHA is anticipated, ensure appropriate sizers and various implant types (e.g., monopolar, bipolar, different stem sizes) are available. For ORIF, plan for low-profile plates and headless compression screws, with different lengths and diameters.
Patient Counseling
Patients must be thoroughly informed about the nature of their injury, the proposed treatment plan, potential risks (e.g., infection, stiffness, nerve injury, nonunion, hardware issues), expected recovery timeline, and the need for dedicated postoperative rehabilitation. Discussion of potential complications, revision surgery, and functional limitations is paramount for informed consent.
Anesthesia and Tourniquet
General anesthesia is typically preferred for optimal muscle relaxation and patient comfort. Regional anesthesia (e.g., interscalene block) can be used as an adjunct for postoperative pain control. A pneumatic tourniquet on the proximal arm is routinely used to provide a bloodless field, crucial for meticulous dissection and fracture reduction.
Patient Positioning and Draping
The most common positioning for radial head fracture surgery is supine on the operating table.
* The affected arm is placed on a radiolucent arm board, allowing for free manipulation of the elbow and forearm.
* The arm board should be positioned such that the elbow can be flexed to 90 degrees or more and extended fully.
* For specific lateral approaches, the patient may be slightly tilted, or the arm board adjusted to allow easier access to the posterolateral aspect of the elbow.
* Alternatively, a lateral decubitus position may be used, with the affected arm draped over a bolster, allowing full visualization and manipulation, especially if concomitant medial-sided surgery is anticipated.
* The entire upper extremity, from the shoulder to the hand, is sterilely prepped and draped to allow for elbow manipulation, assessment of forearm rotation, and in some cases, visualization of the DRUJ if longitudinal instability is a concern.
Detailed Surgical Approach and Technique
The primary surgical goals for radial head fractures include stable anatomical reduction of articular fragments, restoration of forearm rotation, and reconstruction of associated ligamentous injuries to ensure elbow stability.
General Principles of Management
- Anatomic Reduction: For reconstructible fractures, prioritize anatomical restoration of the articular surface to minimize post-traumatic arthritis.
- Stable Fixation: Employ implants that provide sufficient stability to allow early range of motion.
- Preservation of Articular Cartilage: Minimize iatrogenic damage during exposure and fixation.
- Management of Associated Injuries: Address concomitant coronoid fractures, ligamentous instability (LCL, MCL), and DRUJ instability.
- Early Mobilization: Essential to prevent stiffness, a common complication of elbow trauma.
Surgical Approaches
The most common approach for radial head fractures is the lateral approach.
Kocher Lateral Approach
This approach utilizes the internervous plane between the anconeus (radial nerve innervation) and the extensor carpi ulnaris (ECU) (posterior interosseous nerve innervation).
1. Skin Incision: A straight or slightly curved longitudinal incision centered over the lateral epicondyle, extending 4-6 cm proximally and distally along the palpable lateral supracondylar ridge and proximal forearm.
2. Deep Dissection:
* Subcutaneous dissection reveals the deep fascia.
* Incise the deep fascia along the line of the skin incision.
* Identify the interval between the anconeus muscle posteriorly and the extensor carpi ulnaris anteriorly.
* Retract the anconeus posteriorly and the ECU anteriorly. This exposes the lateral capsule and the annular ligament.
* Neurovascular Protection: Meticulous care must be taken to protect the posterior interosseous nerve (PIN), which typically enters the supinator muscle approximately 3-4 cm distal to the radiocapitellar joint. Avoid excessive retraction of the supinator muscle and do not extend the dissection too far distally or anteriorly.
* Incise the lateral capsule longitudinally to expose the radial head and capitellum. The annular ligament can be partially incised or carefully peeled off if necessary, though efforts should be made to preserve its integrity.
3. Visualization: The radial head and capitellum are now directly visualized. Flexing and extending the elbow and pronating/supinating the forearm aids in visualizing the entire articular surface of the radial head.
Anterolateral (Kaplan) Approach
This approach utilizes the interval between the brachioradialis and extensor carpi radialis longus/brevis. It provides a more anterior view of the radial head and is occasionally used when extensive anterior comminution or associated anterior capsule pathology is present. It carries a slightly higher risk of radial nerve injury if not performed meticulously.
Technique for Open Reduction Internal Fixation (ORIF)
ORIF is the preferred method for reconstructible Mason Type II and some Type III fractures, aiming to restore the articular surface and provide stable fixation.
1. Fragment Identification and Debridement: Carefully identify all fracture fragments, remove any hematoma, loose bone fragments, or interposed soft tissue that may impede reduction.
2. Temporary Fixation: Use small K-wires, dental picks, or reduction clamps to achieve anatomical reduction of the articular fragments. Start with the largest, most stable fragments and build the articular surface. Ensure the reduction is anatomical, with no significant step-off or gap.
3. Definitive Fixation:
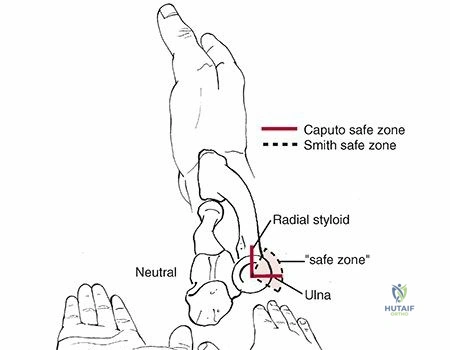
* Low-Profile Plates: Small, low-profile plating systems (e.g., 2.0 mm or 2.4 mm variable angle locking plates) are often used. These plates are designed to be placed on the "safe zone" of the radial head (the 90-degree arc between the radial styloid and Lister's tubercle when the forearm is in neutral rotation). This zone minimizes impingement during pronation/supination.
* Headless Compression Screws: Cannulated headless compression screws (e.g., 2.0 mm) can be used for fixation of larger, less comminuted fragments, especially if they are intra-articular and their heads need to be buried below the articular surface. Multiple screws may be used in conjunction with a plate or alone for simple two-part fractures.
* Screw Length and Placement: Ensure screws are bicortical for optimal purchase and do not penetrate the articular surface of the capitellum. Confirm appropriate screw length by imaging or direct visualization.
4. Articular Reduction Assessment: After fixation, meticulously check the articular surface for congruity. Perform fluoroscopic imaging in various planes and during forearm rotation to confirm the reduction and hardware placement.
5. Motion Testing: Gently move the elbow through a full range of flexion and extension, and pronation/supination, to assess for any mechanical impingement of the hardware against the capitellum or ulna. Adjust hardware if impingement occurs.
6. Associated Ligamentous Repair: If the lateral ulnar collateral ligament (LUCL) complex was disrupted or elevated, it should be repaired back to its isometric point on the lateral epicondyle using non-absorbable sutures through bone tunnels or suture anchors. This is crucial for elbow stability, particularly after fixation or replacement of the radial head.
Technique for Radial Head Arthroplasty (RHA)
RHA is indicated for severely comminuted, unreconstructible Mason Type III fractures, especially those with associated elbow instability (e.g., terrible triad) or longitudinal instability (Essex-Lopresti).
1. Fracture Excision: After exposure via the lateral approach, the comminuted radial head fragments are carefully excised. Ensure complete removal of all bone fragments and meticulous debridement of soft tissue.
2. Sizing and Trialing:
* Prepare the radial neck by removing any remaining cartilage or bone spurs.
* Using trial components, determine the appropriate stem diameter and head size of the radial head prosthesis. The head size should match the resected native radial head and articulate smoothly with the capitellum and lesser sigmoid notch of the ulna.
* Assess for impingement and ensure smooth forearm rotation with the trial implant.
* The goal is to restore the native radial length and maintain contact with the capitellum throughout the range of motion without overstuffing the radiocapitellar or proximal radioulnar joint. Overstuffing can lead to pain, stiffness, and increased contact pressures.
3. Prosthesis Insertion:
* Insert the definitive radial head prosthesis (monopolar or bipolar) into the radial neck. Some prostheses are cemented, while others are press-fit.
* Confirm secure fixation and proper articulation.
4. Stability Assessment: After prosthesis insertion, assess elbow stability in flexion, extension, valgus, and varus stress. Repair any associated ligamentous injuries (e.g., LCL, MCL) as previously described.

Radial Head Excision
Excision of the radial head is now rarely indicated, primarily reserved for low-demand, elderly patients with unreconstructible Mason Type III fractures without associated instability or longitudinal compromise. It is generally contraindicated in the presence of MCL or interosseous membrane injury due to the risk of proximal radial migration and chronic valgus instability.
Closure
After irrigation, carefully repair the joint capsule and lateral ligamentous complex (if incised or repaired). Close the deep fascia and skin in layers. A drain is usually not necessary. Apply a sterile dressing and often a splint, especially if extensive ligamentous repair was performed.
Complications and Management
Despite meticulous surgical technique, radial head fractures and their treatment carry a risk of various complications that can compromise functional outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence | Management Strategy/Salvage |
|---|---|---|
| Elbow Stiffness/Loss of Motion | Very common, up to 50% reported with severe injuries. | Early, controlled rehabilitation. Gentle, progressive active and passive range of motion. Dynamic or static progressive splinting. Surgical release (capsulectomy, heterotopic ossification excision) for recalcitrant cases after 6-12 months. |
| Heterotopic Ossification (HO) | Varies, 10-20% clinically significant HO. Higher in severe trauma. | Prophylaxis: Indomethacin or single-dose radiation therapy (controversial, typically for high-risk cases like head injury, burns, or prior HO). Excision of mature HO if it causes mechanical block or pain, typically after 6-12 months once mature. |
| Post-traumatic Arthritis | Variable, depending on initial injury severity, articular reduction, and fixation quality. | Non-operative management with activity modification, NSAIDs, injections. If severe, may require arthroscopy for debridement, partial or total elbow arthroplasty (TEA) in debilitating cases, or radial head replacement for isolated radiocapitellar arthritis. |
| Hardware Impingement/Prominence | Up to 20-30% with ORIF, especially with non-low-profile plates. | Surgical removal of symptomatic hardware, typically after fracture healing (6-12 months). Careful selection and placement of low-profile implants in the safe zone during initial surgery is preventative. |
| Nonunion/Malunion | Rare with modern techniques, but possible. | Nonunion: Revision ORIF with bone grafting, potentially with vascularized bone graft. Malunion: Corrective osteotomy if functionally limiting, or radial head arthroplasty if the malunion causes pain/impingement and is unreconstructible. |
| Instability (Valgus/Posterolateral Rotatory) | Higher incidence with associated ligamentous injuries (e.g., terrible triad, Essex-Lopresti). | Acute: Meticulous repair of associated ligamentous injuries (LCL, MCL) and proper radial head management (ORIF/RHA). Chronic: Reconstruction of deficient ligaments (e.g., LUCL reconstruction for posterolateral rotatory instability) and/or revision of radial head arthroplasty if stability is compromised by implant failure or sizing. |
| Proximal Radial Migration | Specific to radial head excision without addressing interosseous membrane/DRUJ injury (Essex-Lopresti). | Prevention: Avoid radial head excision in the presence of interosseous membrane or DRUJ injury. Acute: Radial head arthroplasty to restore radial length and stabilize DRUJ. Chronic: Radial head arthroplasty; potentially ulna-shortening osteotomy or DRUJ fusion for recalcitrant cases. |
| Nerve Injury | Rare (PIN, radial, ulnar, median nerve). | Prevention: Meticulous dissection and careful retraction. Intraoperative monitoring if high risk. Management: Observation for neuropraxia. Surgical exploration and neurolysis or repair if no recovery or transection confirmed. |
| Infection | <5% overall, higher with open injuries or multiple procedures. | Prevention: Standard aseptic technique, appropriate perioperative antibiotics. Management: Debridement, irrigation, cultures, targeted antibiotics. Implant retention if stable and wound clean, or removal and staged reconstruction. |
| Complex Regional Pain Syndrome (CRPS) | Variable, difficult to predict. | Early diagnosis and multidisciplinary management: aggressive physical therapy, pain medications, regional blocks, psychological support. |
Prevention Strategies
Many complications can be mitigated by careful preoperative planning, meticulous surgical technique, and early, guided rehabilitation. Optimal implant selection and placement within the radial head's safe zone are paramount for preventing hardware-related issues. Prophylaxis for heterotopic ossification should be considered in high-risk patients. Thorough addressing of all associated ligamentous injuries significantly reduces the risk of postoperative instability.
Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is critical for optimizing functional recovery and minimizing complications after radial head fracture management. The specific protocol will vary depending on the type of fracture, the surgical procedure performed (ORIF, RHA), the quality of fixation, and the presence and repair of associated ligamentous injuries. The overarching goals are to restore pain-free range of motion, regain strength, and prevent elbow stiffness and instability.
General Principles
- Early Motion: Initiating controlled motion early is crucial to prevent stiffness, which is a common and debilitating complication of elbow trauma.
- Protection of Fixation/Repair: The intensity and type of motion must respect the stability of the surgical repair and the healing process.
- Pain and Edema Management: Effective pain control and edema reduction are essential to facilitate patient participation in rehabilitation.
- Gradual Progression: Exercises should be progressively advanced as healing progresses and tolerance allows.
Phase 1 Early Motion and Protection (Weeks 0-2)
- Immobilization:
- For stable fractures with good fixation and no significant ligamentous repair, a sling for comfort is often sufficient, with immediate initiation of active range of motion (AROM).
- If significant ligamentous repair (e.g., LCL, MCL) was performed or if fixation is tenuous, a hinged elbow brace or posterior splint may be used. The brace is typically set to block full extension (e.g., 30-100 degrees flexion) and pronation/supination may be restricted initially.
- Exercises:
- Active Range of Motion (AROM): Gentle, gravity-assisted flexion and extension, pronation and supination within pain limits and any prescribed brace restrictions. The patient is encouraged to perform these exercises frequently throughout the day.
- Passive Range of Motion (PROM): May be cautiously initiated by a therapist if indicated by the surgeon, avoiding forceful manipulation.
- Hand, Wrist, and Shoulder Exercises: To maintain strength and prevent stiffness in adjacent joints.
- Pain and Edema Control: Ice, elevation, analgesics.
- Wound Care: Monitor surgical incision.
Phase 2 Intermediate Strengthening and Range of Motion (Weeks 2-6)
- Progressive ROM: Gradually increase the arc of motion as tolerated. If a brace was used, its limits are incrementally expanded. The goal is often full extension and flexion by 6 weeks, and full pronation/supination.
- Gentle Strengthening:
- Initiate isometric exercises for elbow flexors, extensors, pronators, and supinators.
- Progress to very light isotonic exercises with low resistance (e.g., theraputty, light weights).
- Scar Management: Gentle massage to minimize scar tissue adhesion and improve pliability.
- Activities of Daily Living (ADLs): Encourage use of the arm for light ADLs, avoiding heavy lifting or sudden movements.
Phase 3 Advanced Strengthening and Functional Return (Weeks 6-12+)
- Progressive Strengthening:
- Increase resistance and repetitions for isotonic exercises.
- Incorporate eccentric exercises.
- Begin functional strengthening activities that mimic sport or work-specific movements.
- End-Range Stretching: Focus on regaining any residual loss of full extension or flexion through sustained stretching, as tolerated. Dynamic splinting may be considered for persistent deficits.
- Proprioception and Coordination: Exercises to improve neuromuscular control.
- Return to Activity: Gradually progress to sport-specific drills or work-related tasks. Full return to unrestricted activities, especially contact sports or heavy labor, typically occurs between 3-6 months, depending on healing and functional recovery.
- Continue Pain and Swelling Management: As needed.
Specific Considerations
- Associated Ligamentous Repair: If an LCL repair was performed, avoid resisted supination for the first 6 weeks and protect against varus stress. If an MCL repair was performed, protect against valgus stress.
- Bone Healing: For ORIF, ensure radiographic evidence of fracture healing before allowing unrestricted activities or heavy loading.
- Patient Adherence: Emphasize the importance of consistent participation in the rehabilitation program for optimal outcomes. Non-compliance is a significant predictor of poor results.
Summary of Key Literature and Guidelines
The management of radial head fractures has evolved significantly, driven by a deeper understanding of elbow biomechanics, advances in implant technology, and outcomes-based research. Current literature and guidelines emphasize a tailored approach, prioritizing stability, anatomical reconstruction, and early motion.
Evolution of Treatment Paradigms
Historically, radial head excision was a common treatment for displaced and comminuted fractures. However, its association with complications such as proximal radial migration, chronic instability (especially in the presence of ligamentous injury), and DRUJ dysfunction led to a paradigm shift. Modern literature now strongly advocates for either anatomical Open Reduction Internal Fixation (ORIF) for reconstructible fractures or Radial Head Arthroplasty (RHA) for severely comminuted or unreconstructible fractures, particularly when associated with instability.
Evidence for ORIF
Multiple studies support ORIF for Mason Type II and selected Type III fractures, demonstrating superior outcomes in terms of pain, range of motion, and functional scores compared to excision, provided anatomical reduction and stable fixation are achieved. The use of low-profile implants placed in the radial head's "safe zone" has significantly reduced rates of hardware impingement and subsequent removal. Factors influencing successful ORIF include fragment size, fracture pattern complexity, and bone quality. Nonunion rates are generally low with modern techniques, but malunion can lead to stiffness and arthrosis.
Evidence for Radial Head Arthroplasty
Radial head arthroplasty has emerged as a reliable option for unreconstructible Mason Type III and Type IV fractures, especially in the context of associated ligamentous injuries (e.g., terrible triad) or longitudinal instability (Essex-Lopresti injury). RHA aims to restore both radial length and the secondary valgus restraint, thus stabilizing the elbow and preventing proximal radial migration. Both monopolar and bipolar implants are available, with literature showing comparable functional outcomes. Careful sizing of the prosthesis is critical to avoid overstuffing the radiocapitellar joint, which can lead to stiffness, pain, and accelerated capitellar wear. Outcomes following RHA are generally favorable, with good to excellent results reported in the majority of patients, although stiffness and component loosening remain potential long-term concerns.
Management of Associated Injuries
The literature unequivocally highlights the importance of identifying and addressing associated injuries. The "terrible triad" of the elbow (radial head fracture, coronoid fracture, and elbow dislocation) is a complex injury pattern demanding comprehensive surgical reconstruction, including coronoid fixation, radial head management (ORIF or RHA), and repair of the lateral collateral ligament (LCL) complex. Failure to address all components of these complex injuries leads to high rates of persistent instability and poor functional outcomes. The Essex-Lopresti injury, characterized by a radial head fracture, interosseous membrane disruption, and DRUJ instability, mandates radial head reconstruction (ORIF or RHA) to restore radial length and prevent proximal migration.
Role of Arthroscopy
Elbow arthroscopy is gaining traction as a diagnostic and therapeutic adjunct in radial head fractures. It can assist in precise assessment of articular congruity, removal of small osteochondral fragments or loose bodies, and evaluation of associated ligamentous injuries. However, its role in definitive fixation is generally limited to simple, non-displaced or minimally displaced fractures, or as an adjunct to open procedures.
Future Directions
Ongoing research focuses on improving implant design, enhancing biological healing, and refining rehabilitation protocols. The long-term durability of radial head prostheses, particularly in younger, active individuals, remains an area of interest. Further elucidation of specific biomechanical contributions of the radial head and various ligamentous structures continues to refine our understanding of elbow stability.
In summary, the contemporary management of radial head fractures is guided by a principles-based approach:
1. Accurate diagnosis and classification, with liberal use of advanced imaging.
2. Comprehensive assessment for associated ligamentous and osseous injuries.
3. Anatomical reconstruction or replacement of the radial head when indicated.
4. Meticulous repair of all contributing stabilizing structures.
5. Aggressive, yet protected, early rehabilitation to prevent stiffness.
Adherence to these tenets maximizes the potential for restoring elbow function and minimizing long-term disability for patients with these challenging injuries.
Clinical & Radiographic Imaging

Detailed Chapters & Topics
Dive deeper into specialized chapters regarding radial-head-fractures