Masterclass: Comprehensive Management of Radial Head and Neck Fractures

Key Takeaway
This masterclass provides an immersive, step-by-step guide to managing radial head and neck fractures. Explore comprehensive anatomy, preoperative planning, and intraoperative execution of closed and percutaneous reduction techniques. Learn critical pearls, pitfalls, and post-operative care, ensuring optimal outcomes for these challenging elbow injuries.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to this masterclass on the definitive management of radial head and neck fractures. These injuries represent a fascinating intersection of complex joint biomechanics, intricate neurovascular anatomy, and the unique physiological demands of both the growing pediatric skeleton and the high-demand adult upper extremity. This is not merely an exercise in achieving radiographic alignment; it is a meticulous endeavor to preserve the delicate kinematics of the proximal radioulnar and radiocapitellar joints. A failure to appreciate the nuances of these fractures frequently leads to devastating long-term sequelae, including profound stiffness, early-onset osteoarthritis, and debilitating chronic instability. Therefore, we must approach these injuries with a profound respect for the anatomy and a rigorous, evidence-based surgical strategy.
To establish a solid foundation, we must first rigorously define and classify these injuries. A radial neck fracture is strictly defined as an extra-articular fracture of the radius located proximal to the bicipital tuberosity. Epidemiologically, these are particularly prevalent in the pediatric population, specifically children aged 9 to 12 years, where they account for approximately 14% of all pediatric elbow fractures. In this demographic, the proximal radial physis is frequently involved, typically presenting as a Salter-Harris I or II fracture pattern. However, we must maintain a high index of suspicion for Salter-Harris III and IV patterns, which imply intra-articular extension, disruption of the articular cartilage, and a significantly more guarded prognosis regarding future joint congruity. Furthermore, it is not uncommon to encounter fractures that are entirely extraphyseal, traversing the metaphysis exclusively. Conversely, intra-articular radial head fractures, while ubiquitous in skeletally mature patients (representing up to 52% of all adult elbow injuries), are exceedingly rare in children with open physes, comprising only about 7% of pediatric cases.
Classification systems are paramount, not merely for academic categorization, but to dictate our therapeutic algorithms. The Wilkins classification is the gold standard for understanding the mechanism and anatomic pattern in pediatric populations, particularly regarding physeal or articular involvement. It categorizes injuries into Type I (Valgus Injury), subdivided into A (Physeal injury—Salter-Harris I or II), B (Intra-articular—Salter-Harris III or IV), and C (Metaphyseal fracture). Type II encompasses fractures associated with an elbow dislocation, subdivided into D (Fracture occurred during dislocation) and E (Fracture occurred during reduction). Beyond anatomic patterns, classifications based on the degree of angulation are critical for surgical decision-making. The O’Brien classification stratifies fractures into Type I (less than 30 degrees angulation), Type II (30 to 60 degrees angulation), and Type III (more than 60 degrees angulation). Similarly, the Judet classification offers a granular assessment: Type I (Undisplaced), Type II (Less than 30 degrees angulation), Type III (30 to 60 degrees angulation), Type IVa (60 to 80 degrees angulation), and Type IVb (More than 80 degrees angulation).
The pathogenesis of these fractures is inextricably linked to their clinical presentation. The most common etiology is a massive valgus and axial force applied to the elbow, classically resulting from a fall on an outstretched hand (FOOSH) with the elbow in extension and the forearm pronated. This specific mechanism generates a tremendous lateral compression force across the radiocapitellar joint, leading to failure of the radial head or neck, while simultaneously imparting a medial traction injury to the medial collateral ligament (MCL) complex. The precise plane of maximal radial head angulation is highly dependent on the forearm's rotational position at the exact moment of impact. This kinematic reality is vital to remember during closed reduction maneuvers; we must often recreate the exact position of injury to unlock the impacted fracture fragments. Furthermore, we must actively hunt for associated injuries. Occult MCL ruptures, capitellar osteochondral shear fractures, or subtle elbow subluxations occur in 30% to 50% of these cases. In adults, we must also rule out the "terrible triad" (radial head fracture, coronoid fracture, and elbow dislocation) and the Essex-Lopresti lesion (radial head fracture with distal radioulnar joint disruption and interosseous membrane tear), both of which drastically alter our surgical approach.
Detailed Surgical Anatomy and Biomechanics
Mastery of the surgical anatomy of the proximal radius and its surrounding structures is non-negotiable. The elbow is a highly constrained, compact joint where millimeters dictate the difference between a functional recovery and a catastrophic complication. The radial head is a complex, asymmetric cylindrical structure covered by hyaline cartilage. It articulates proximally with the capitellum of the humerus, absorbing up to 60% of the axial load transmitted across the elbow joint, and medially with the radial notch of the ulna, forming the proximal radioulnar joint (PRUJ). The radial neck, situated just distal to the head, is extra-articular. Crucially, the normal radial neck exhibits approximately 15 degrees of lateral angulation on anteroposterior (AP) radiographs and 5 degrees of anterior angulation on lateral views. Recognizing this inherent anatomical angulation is vital to prevent over-reduction or misinterpretation of post-operative imaging. In pediatric patients, the ossific nucleus of the radial head typically appears between 3 and 5 years of age; prior to this, diagnosing subtle fractures relies heavily on secondary radiographic signs and advanced imaging.
The stability of the proximal radioulnar joint and the radial head is orchestrated by a complex network of ligamentous restraints. The primary stabilizer is the robust annular ligament, which encircles the radial head and anchors it to the sigmoid notch of the ulna. This is reinforced by the lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL), which acts as the primary restraint to posterolateral rotatory instability (PLRI). The accessory collateral ligament and the quadrate ligament provide secondary stability. During high-energy trauma, these capsuloligamentous structures are frequently stretched, avulsed, or frankly ruptured. Even if a perfect osseous reduction of the radial neck is achieved, unrecognized incompetence of the LUCL or annular ligament will result in chronic micro-instability, leading to premature articular wear and progressive pain.
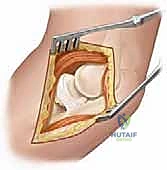
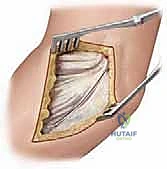
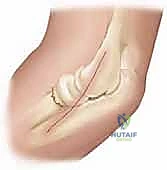
We must now turn our attention to the critical neurovascular structures, specifically the posterior interosseous nerve (PIN), which represents the greatest hazard during surgical intervention in this region. At the level of the lateral epicondyle, the radial nerve bifurcates into the superficial sensory branch and the deep motor branch, the PIN. The PIN travels distally, coursing directly anterior to the radiocapitellar joint and the radial neck. It then dives beneath the proximal edge of the superficial head of the supinator muscle—the Arcade of Frohse—located approximately 2.6 cm distal to the articular surface of the radial head.

As illustrated above, the PIN's intimate relationship with the anterior radial neck makes it exceptionally vulnerable during both percutaneous pinning and open approaches. Iatrogenic injury to the PIN results in a devastating motor deficit, characterized by the inability to extend the metacarpophalangeal joints and the thumb. When utilizing the Kocher or Kaplan intervals, extreme vigilance, meticulous dissection, and pronation of the forearm (which moves the PIN medially and away from the surgical field) are mandatory protective maneuvers.
The vascular anatomy of the proximal radius is equally unforgiving. The radial neck is largely devoid of direct muscular attachments, rendering its blood supply heavily reliant on the surrounding periosteal network and intraosseous vessels. The primary arterial supply is derived from the radial recurrent artery, which originates from the radial artery and courses proximally toward the lateral epicondyle, running along the anteromedial surface of the supinator. The intraosseous blood supply to the radial head enters distally at the radial neck and travels proximally. Consequently, displaced fractures of the radial neck severely disrupt this retrograde blood flow. Extensive surgical stripping of the periosteum during open reduction and internal fixation (ORIF) further devascularizes the fragment, drastically increasing the incidence of avascular necrosis (AVN) and subsequent nonunion. Therefore, our surgical techniques must prioritize biology alongside mechanics, utilizing minimally invasive or percutaneous methods whenever feasible.
Exhaustive Indications and Contraindications
The decision-making process for managing radial head and neck fractures requires a nuanced synthesis of patient age, functional demands, fracture morphology, and the presence of concomitant injuries. We have historically relied heavily on rigid radiographic parameters to dictate operative intervention. However, modern orthopedic philosophy dictates that we must evaluate the functional implications of the deformity rather than treating the radiograph alone. The overarching goal is the restoration of a congruent radiocapitellar and proximal radioulnar joint to permit unrestricted, pain-free pronation and supination.
| Parameter | Non-Operative Management | Operative Management (CRPP / ORIF) |
|---|---|---|
| Angulation (Judet/O'Brien) | < 30 degrees | > 30 degrees (Relative), > 45 degrees (Absolute) |
| Translation/Displacement | < 2-3 mm | > 3 mm |
| Forearm Rotation | Full, unrestricted active ROM | Mechanical block to pronation or supination |
| Joint Congruity | Maintained radiocapitellar alignment | Subluxation or dislocation of the radial head |
| Associated Injuries | Isolated injury | Concomitant MCL tear, coronoid fracture, Essex-Lopresti |
Indications for surgical intervention are primarily driven by mechanical blocks to motion and severe displacement. An absolute indication for reduction (either closed, percutaneous, or open) is any mechanical block to forearm rotation, regardless of the measured radiographic angulation. Even a seemingly benign 20-degree angulation can impinge on the radial notch of the ulna if the displacement vector is directed posteromedially. Radiographically, angulation exceeding 30 to 45 degrees or translation greater than 3 mm generally warrants intervention, as remodeling in the older child (approaching skeletal maturity) or adult is insufficient to restore normal kinematics. In pediatric patients, the remodeling potential of the proximal radius is robust, but it is strictly limited by the remaining growth potential of the proximal radial physis. Therefore, a 30-degree angulation might be acceptable in a 5-year-old but is an absolute indication for surgery in a 13-year-old.
Contraindications to operative intervention are relatively few but critical to recognize. Absolute contraindications include active, untreated local infection (e.g., overlying cellulitis or septic arthritis) and severe medical comorbidities that render anesthesia prohibitively dangerous. Relative contraindications include undisplaced or minimally displaced fractures (Judet Type I and II) with full, pain-free range of motion. In the elderly, low-demand patient with a highly comminuted radial head fracture, early mobilization or primary radial head excision may be preferred over complex, prolonged ORIF that is likely to fail or result in profound stiffness. Furthermore, attempting delayed open reduction in a pediatric patient presenting several weeks post-injury is heavily contraindicated due to the massive risk of iatrogenic AVN and radioulnar synostosis; in such neglected cases, allowing the fracture to malunite and addressing the deformity with a delayed corrective osteotomy is often the safer, albeit complex, salvage pathway.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the hallmark of the master surgeon. The success of the procedure is largely dictated before the scalpel ever touches the skin. This phase begins with a meticulous clinical evaluation. A detailed history elucidating the exact mechanism of injury is crucial; high-energy trauma should immediately raise suspicion for a terrible triad injury or an Essex-Lopresti lesion. During the physical examination, systematic palpation is required. Tenderness over the medial epicondyle or the distal radioulnar joint (DRUJ) must be documented. A comprehensive neurovascular exam, with specific attention to the motor function of the PIN (assessing thumb retropulsion and independent index finger extension), is absolutely mandatory to establish a preoperative baseline.
The evaluation of mechanical blocks to motion is often limited by pain and muscle guarding in the emergency department. Therefore, an Examination Under Anesthesia (EUA) is frequently the first and most critical step in the operating room. Once the patient is relaxed, the surgeon must gently assess full flexion, extension, pronation, and supination. Any subtle block or crepitus during rotation confirms the necessity for reduction. Furthermore, varus and valgus stress testing at 30 degrees of elbow flexion must be performed to evaluate collateral ligament integrity.
Standard radiographic evaluation includes true AP, lateral, and oblique views of the elbow. The radiocapitellar line must be meticulously assessed on all views; a line drawn down the center of the radial neck must perfectly bisect the capitellum. Any deviation indicates subluxation or dislocation.

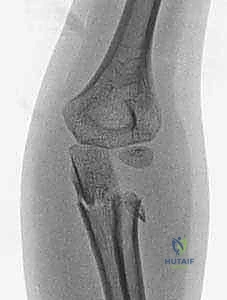
As seen in the radiographs above, evaluating the true degree of angulation can be exceptionally challenging, particularly in young children with non-ossified radial heads or when concomitant injuries, such as an ulnar shaft fracture, complicate the clinical picture. Plain orthogonal views frequently underestimate the maximal plane of deformity.
For complex cases, or in young pediatric patients where the cartilaginous radial head is invisible on plain films, advanced imaging is indispensable. Magnetic Resonance Imaging (MRI) or high-resolution ultrasound provides unparalleled visualization of the unossified cartilaginous anlage, the integrity of the articular surface, and the status of the surrounding ligamentous structures.


These MRI slices vividly demonstrate a severe, 60-degree radial neck angulation and articular incongruity that were entirely masked on standard plain radiographs. Arthrography, performed intraoperatively, is another powerful adjunct to delineate the joint surface and confirm concentric reduction in the pediatric population.
Patient positioning must be optimized for both surgical access and unhindered fluoroscopic visualization. The patient is typically positioned supine on a radiolucent operating table. The operative arm is placed on a radiolucent hand table. A non-sterile tourniquet is applied high on the brachium. The C-arm fluoroscope must be positioned to allow effortless transition between AP and lateral views without manipulating the fractured extremity. The surgeon should sit axillary to the patient, ensuring direct line-of-sight to the fluoroscopy monitor. Proper templating, particularly if intramedullary fixation or plate osteosynthesis is anticipated, must be performed preoperatively to ensure the availability of appropriate implant sizes, including titanium elastic nails (TENs), headless compression screws, and low-profile mini-fragment plates.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of radial neck fractures follows a strict escalation of invasiveness: closed reduction, followed by percutaneous manipulation/fixation, and finally, open reduction and internal fixation. The overarching principle is to achieve anatomical reduction while minimizing soft tissue stripping to preserve the tenuous blood supply.
Closed Reduction Techniques
Closed reduction should always be the initial attempt for displaced fractures. The two most common techniques are the Patterson maneuver and the Israeli maneuver. In the Patterson technique, the elbow is held in extension. An assistant provides counter-traction on the humerus. The surgeon applies varus stress to the elbow to open the lateral joint space, simultaneously applying direct digital pressure over the displaced radial head, pushing it medially and proximally while dynamically rotating the forearm. The Israeli technique involves flexing the elbow to 90 degrees, maximally supinating the forearm, and applying direct pressure to the radial head while simultaneously pronating the forearm.



These images demonstrate the precise hand positioning required for closed manipulation. The surgeon's thumb acts as a fulcrum against the displaced radial head. If closed reduction yields an acceptable alignment (less than 30 degrees angulation) and full, unblocked rotation is achieved, the elbow is immobilized in a long-arm cast or splint in 90 degrees of flexion and neutral rotation for 2 to 3 weeks.
Percutaneous and Intramedullary Fixation
If closed reduction fails or the fracture is highly unstable, percutaneous techniques are employed. The gold standard for pediatric radial neck fractures is the Metaizeau technique, which utilizes a retrograde intramedullary titanium elastic nail (TEN). A small incision is made over the lateral aspect of the distal radius, strictly avoiding the superficial radial nerve. The cortex is breached with an awl, and a pre-bent TEN (typically 1.5 to 2.0 mm) is introduced into the medullary canal.



The nail is advanced proximally under fluoroscopic guidance until the pre-bent tip engages the displaced radial head fragment.


Once engaged, the nail is rotated 180 degrees. The curved tip acts as an internal lever, sweeping the radial head back into anatomic alignment. The nail is then driven slightly into the subchondral bone for definitive fixation and cut flush at the distal entry site.
Alternatively, percutaneous K-wire leverage (the "joystick" technique) can be utilized. A robust K-wire (e.g., 2.0 mm) is inserted percutaneously into the displaced radial head fragment.



Using the K-wire as a joystick, the fragment is physically levered into reduction. Once reduced, the fragment can be pinned to the proximal ulna (radioulnar transfixation) or down the radial neck, though trans-articular pinning is generally discouraged due to the risk of pin breakage and joint damage.
Open Reduction and Internal Fixation (ORIF)
When all closed and percutaneous methods fail, or in the presence of complex adult intra-articular fractures, ORIF is required. The surgical approach is typically via the Kocher interval (between the anconeus and extensor carpi ulnaris) or the Kaplan interval (between the extensor carpi radialis brevis and extensor digitorum communis). The forearm must be strictly pronated to protect the PIN. The annular ligament is carefully incised, taking care to preserve the LUCL.




The fracture is meticulously debrided of hematoma and interposed periosteum. Reduction is achieved under direct vision. Fixation in adults is typically achieved using headless compression screws or
Clinical & Radiographic Imaging Archive