Open Reduction and Internal Fixation of Radial Head Fractures: A Comprehensive Surgical Guide

Key Takeaway
Open reduction and internal fixation (ORIF) of radial head fractures aims to restore radiocapitellar stability and forearm rotation. Indicated primarily for displaced Mason Type II and reconstructable Type III fractures, successful ORIF requires meticulous surgical exposure via the Kocher or Kaplan interval, precise articular reduction, and rigid fixation within the radial safe zone to protect the posterior interosseous nerve and ensure optimal functional recovery.
Comprehensive Introduction and Patho-Epidemiology
Radial head fractures represent the most frequently encountered articular fractures of the adult elbow, accounting for approximately one-third of all elbow fractures and up to 20% of all acute elbow trauma. The pathomechanics of this injury typically involve a high-energy axial load transmitted through a partially flexed and pronated forearm. As the patient attempts to arrest a fall on an outstretched hand, the resultant force vector drives the radial head directly into the convex, unyielding surface of the humeral capitellum. This impaction force not only results in shear and compression fractures of the radial head but frequently causes concomitant chondral or osteochondral injuries to the capitellum itself, which can significantly complicate the clinical picture and long-term functional outcomes.
The epidemiological profile of radial head fractures demonstrates a bimodal distribution, frequently affecting young, active individuals engaged in high-velocity sports or motor vehicle accidents, as well as an older cohort sustaining lower-energy, osteoporotic fragility falls. In high-energy scenarios, radial head fractures rarely occur in isolation. They are notoriously associated with complex ligamentous disruptions and multiligamentous elbow injuries, most notably the "terrible triad" of the elbow—a devastating injury pattern characterized by a radial head fracture, a coronoid process fracture, and a posterior elbow dislocation. The failure to recognize and adequately treat the associated soft tissue and bony stabilizing injuries inevitably leads to chronic elbow instability, early-onset post-traumatic osteoarthritis, and profound functional impairment.
Historically, the management of displaced or comminuted radial head fractures was heavily biased toward complete radial head excision. However, a deeper understanding of elbow biomechanics has illuminated the catastrophic consequences of this approach, particularly in the setting of unrecognized interosseous membrane tears (Essex-Lopresti lesions) or medial ulnar collateral ligament (MUCL) insufficiency. Excision in these scenarios precipitates proximal radial migration, ulnocarpal impaction syndrome, and chronic valgus instability. Consequently, modern orthopedic traumatology dictates that anatomic Open Reduction and Internal Fixation (ORIF) is the absolute gold standard for all reconstructable radial head fractures.
When managing these complex articular injuries, the orthopedic surgeon must meticulously weigh the indications for ORIF against radial head arthroplasty. While prosthetic replacement offers immediate restoration of the radiocapitellar column and is invaluable for un-reconstructable, highly comminuted fractures, it carries a substantial risk of overstuffing the radiocapitellar joint. Overstuffing alters the native kinematics of the elbow, leading to accelerated capitellar erosion, chronic lateral elbow pain, and a marked, permanent decrease in terminal flexion and extension. Therefore, preserving the native radial head through meticulous osteosynthesis remains the primary objective whenever anatomically feasible, ensuring the preservation of native biomechanics and averting the long-term pitfalls associated with metallic or pyrocarbon arthroplasty.
Detailed Surgical Anatomy and Biomechanics
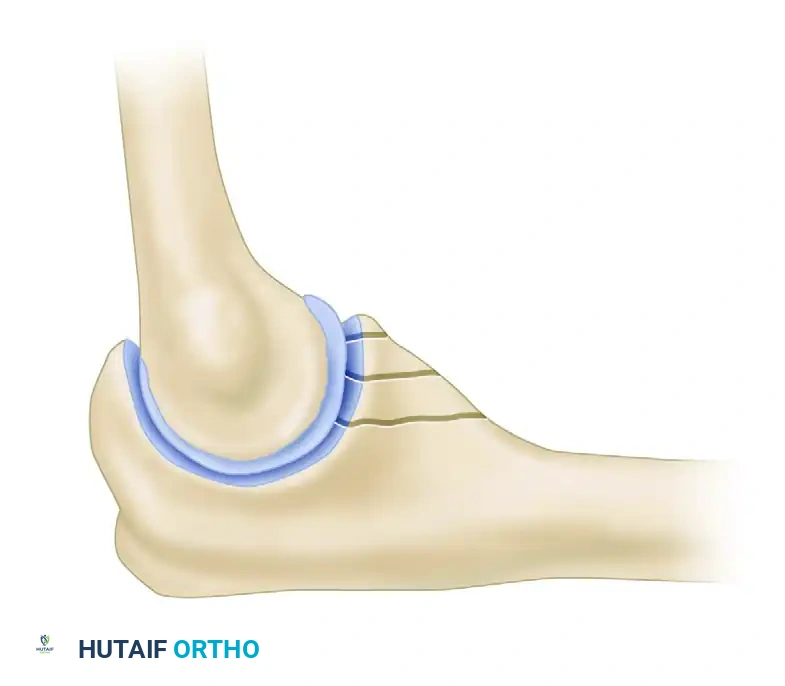
A profound understanding of the surgical anatomy and biomechanical properties of the proximal radius is non-negotiable for any surgeon attempting osteosynthesis in this region. The radial head is not perfectly cylindrical; rather, it is an elliptical or cam-shaped structure that articulates with both the humeral capitellum and the lesser sigmoid notch of the proximal ulna. The concave superior articular surface, termed the fovea, matches the convexity of the capitellum, while the peripheral articular margin, which is covered with hyaline cartilage for approximately 240 degrees of its circumference, articulates with the ulna. The remaining 110-degree to 120-degree arc of the radial head is devoid of articular cartilage. This non-articulating segment is critically designated as the "safe zone" for hardware placement, as implants positioned outside this arc will inevitably impinge upon the proximal radioulnar joint (PRUJ) during forearm rotation, leading to severe mechanical blocks and early degenerative changes.
The vascular anatomy of the radial head is notoriously precarious, predisposing it to avascular necrosis (AVN) and nonunion following high-energy trauma and extensive surgical dissection. The blood supply is predominantly retrograde, derived from a single intraosseous vessel ascending from the radial shaft, supplemented by a tenuous extraosseous plexus formed by small capsular vessels penetrating the non-articulating portion of the radial neck. Aggressive soft tissue stripping, particularly the elevation of the periosteum distal to the annular ligament, can completely devascularize the articular fragments. Therefore, surgical approaches must be fastidiously planned to minimize disruption of this delicate vascular network, often necessitating the use of fine, low-profile implants and the avoidance of circumferential subperiosteal dissection.
Biomechanically, the radial head is a critical secondary stabilizer of the elbow joint. While the anterior band of the medial ulnar collateral ligament (MUCL) serves as the primary restraint to valgus stress, the radial head provides approximately 30% of the valgus stability in a native elbow. However, in the setting of an MUCL rupture—a frequent concomitant injury in complex elbow trauma—the radial head becomes the primary and often sole restraint to valgus displacement. Excision of the radial head in an MUCL-deficient elbow will result in immediate and catastrophic valgus instability. Furthermore, the radial head acts as the primary restraint against proximal migration of the radius. The longitudinal stability of the forearm relies on the synergistic function of the radial head, the interosseous membrane (IOM), and the triangular fibrocartilage complex (TFCC) at the wrist.
The radiocapitellar joint transmits up to 60% of the axial load across the elbow during normal upper extremity weight-bearing and lifting activities. This massive force transmission underscores the necessity for rigid, anatomic fixation of radial head fractures. Even minor articular step-offs or malreductions can dramatically alter the contact mechanics of the radiocapitellar joint, leading to focal areas of high cartilage stress and subsequent rapid chondrolysis. The surgeon must therefore approach radial head ORIF with the precision of intra-articular fracture management, utilizing techniques that provide absolute stability, allow for early active mobilization, and flawlessly restore the complex elliptical geometry of the native proximal radius.
Exhaustive Indications and Contraindications
The decision-making algorithm for the surgical management of radial head fractures is heavily reliant on the Mason-Johnston classification system, combined with a thorough assessment of associated ligamentous injuries. Mason Type I fractures are non-displaced and are universally treated non-operatively with a brief period of immobilization followed by early active motion. Mason Type II fractures involve partial articular displacement (>2 mm) or an angulated fragment that creates a mechanical block to forearm pronation and supination. Mason Type III fractures are characterized by complete articular comminution involving the entire radial head. Mason Type IV fractures, added by Johnston, describe any radial head fracture associated with an elbow dislocation.
The primary indication for Open Reduction and Internal Fixation (ORIF) is a displaced Mason Type II fracture, particularly those demonstrating a mechanical block to rotation on clinical examination or under fluoroscopy. ORIF is also strongly indicated for reconstructable Mason Type III fractures. A fracture is generally deemed "reconstructable" if it consists of three or fewer major articular fragments that can be anatomically reduced and stably fixed without leaving massive osteochondral voids. In the context of multiligamentous elbow injuries or the "terrible triad," the threshold for surgical intervention is significantly lowered. In these unstable scenarios, even minimally displaced radial head fractures may require fixation to restore the lateral column and provide a stable foundation for lateral ulnar collateral ligament (LUCL) repair.
Contraindications to ORIF primarily revolve around fracture morphology that precludes stable, anatomic reconstruction. Severe comminution (greater than three major articular fragments), profound osteopenia, and extensive metaphyseal bone loss are absolute contraindications, as the rate of hardware failure, nonunion, and secondary displacement in these settings is unacceptably high. In such cases, attempting ORIF will likely result in a biologically dead, mechanically unstable construct, necessitating a morbid revision surgery. These un-reconstructable fractures are definitively managed with primary radial head arthroplasty using a modular metallic prosthesis. Additionally, severe, medically unoptimized comorbidities or an inability to comply with a strict postoperative rehabilitation protocol may serve as relative contraindications to extensive osteosynthesis.
To aid the operative surgeon in clinical decision-making, the following table delineates the comparative indications, advantages, and disadvantages of the three primary surgical modalities for radial head fractures:
| Surgical Modality | Primary Indications | Key Advantages | Major Disadvantages / Risks |
|---|---|---|---|
| Anatomic ORIF | Mason II; Reconstructable Mason III (≤ 3 fragments); Any fracture with mechanical block. | Preserves native radiocapitellar kinematics; avoids overstuffing; maintains bone stock. | Risk of AVN, nonunion, hardware impingement, and technical complexity. |
| Radial Head Arthroplasty | Un-reconstructable Mason III (> 3 fragments); severe osteopenia; delayed presentations. | Immediate stability; allows early aggressive ROM; definitive treatment for severe comminution. | Risk of capitellar erosion, overstuffing, implant loosening, and long-term wear. |
| Radial Head Excision | Isolated, highly comminuted fractures in low-demand, elderly patients with INTACT IOM and MCL. | Technically simple; rapid pain relief in appropriately selected, low-demand patients. | Absolute contraindication if IOM or MCL is injured (Essex-Lopresti); leads to proximal migration. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful radial head osteosynthesis. The standard radiographic series must include true anteroposterior (AP) and lateral views of the elbow. However, the complex overlapping anatomy of the proximal radioulnar joint often obscures the true extent of radial head comminution. Therefore, a Greenspan view (radiocapitellar view), obtained by angling the X-ray beam 45 degrees cephalad while the patient's elbow is flexed to 90 degrees and the forearm is in neutral rotation, is highly recommended to isolate the radiocapitellar articulation.
In modern orthopedic traumatology, a dedicated Computed Tomography (CT) scan with 3D reconstructions is considered the standard of care for any complex radial head fracture, particularly those suspected of being part of a "terrible triad" injury. The CT scan is invaluable for mapping the exact number, size, and spatial orientation of the articular fragments. Furthermore, it is essential for identifying occult capitellar shear fractures and quantifying the degree of coronoid process involvement. The O’Driscoll Classification of Coronoid Fractures is universally utilized during this planning phase, as the specific coronoid fracture pattern directly dictates the surgical approach and the sequence of fixation.
The O’Driscoll Classification categorizes coronoid fractures based on their anatomic location and fragmentation pattern:
O’Driscoll Classification of Coronoid Fractures
Type I: Tip Fractures
These fractures involve the very apex of the coronoid. Subtype 1 involves ≤ 2 mm of coronoid bony height and often represents a capsular avulsion or flake fracture. Subtype 2 involves > 2 mm of coronoid height. While seemingly minor, these fractures often indicate a profound hyperextension/valgus injury and are frequently associated with severe instability.

Type II: Anteromedial Facet Fractures
These fractures involve the anteromedial rim of the coronoid and are pathognomonic for varus posteromedial rotatory instability. Subtype 1 involves the anteromedial rim alone. Subtype 2 includes the rim and the tip. Subtype 3 extends to involve the sublime tubercle, which is the critical anatomic insertion site of the anterior band of the MUCL.
Type III: Basal Fractures
These are massive structural injuries involving the base of the coronoid. Subtype 1 involves the coronoid body and base, severely compromising the anterior buttress of the ulnohumeral joint. Subtype 2 is a transolecranon basal coronoid fracture, typically requiring extensive posterior plating for stabilization.
Patient positioning must be optimized to allow seamless access to both the medial and lateral aspects of the elbow, as well as unimpeded fluoroscopic imaging. The patient is placed in the supine position with the operative extremity extended onto a radiolucent hand table. A non-sterile pneumatic tourniquet is applied high on the brachium to maximize the operative field. The C-arm fluoroscopy unit is typically brought in parallel to the operating table or from the head of the bed, allowing the surgeon to obtain orthogonal views by simply rotating the patient's shoulder rather than manipulating the fractured elbow. Pre-operative templating using digital software is crucial to anticipate the required sizes of headless compression screws or pre-contoured radial head plates, ensuring all necessary inventory is available prior to incision.
Step-by-Step Surgical Approach and Fixation Technique
Exposure of the radial head and neck is typically achieved via one of two primary lateral approaches: the Kocher approach or the Kaplan approach. The choice of approach is dictated by the surgeon's familiarity, the specific fracture pattern, and the location of associated injuries (e.g., coronoid fractures).
The Kocher approach utilizes the internervous plane between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (innervated by the posterior interosseous nerve). This approach provides unparalleled, direct exposure of the posterior aspect of the radial head and the capitellum. However, its primary disadvantage is a significantly higher risk of iatrogenic injury to the lateral ulnar collateral ligament (LUCL). If the dissection strays too far anteriorly or distally, the LUCL, which originates on the lateral epicondyle and inserts on the supinator crest of the ulna, can be easily transected, leading to profound posterolateral rotatory instability (PLRI).
Conversely, the Kaplan approach exploits the interval between the extensor digitorum communis (EDC) and the extensor carpi radialis brevis (ECRB). This approach provides a more anterior trajectory, offering excellent visualization of the anterior radial head and facilitating access to the coronoid process if simultaneous fixation is required. The critical disadvantage of the Kaplan approach is its proximity to the posterior interosseous nerve (PIN). The PIN crosses the operative field within the substance of the supinator muscle, making it highly vulnerable to traction or direct laceration if retractors are placed carelessly. Regardless of the approach, the forearm must be maintained in full pronation during deep dissection and retractor placement; pronation physically translocates the PIN anteriorly and medially, pulling it safely away from the lateral surgical window.
Fixation of Mason Type II Fractures
For Mason Type II partial articular fractures, the surgical objective is perfect anatomic reduction and stable compression to facilitate immediate postoperative motion. Upon exposing the fracture, the joint is meticulously irrigated to evacuate the fracture hematoma, and any non-viable, millimeter-sized osteochondral debris is excised. The capitellum must be visually inspected and palpated with a probe to rule out associated chondral shear injuries.
Reduction is achieved using fine dental picks, K-wires acting as joysticks, or small Freer elevators. The articular surface must be restored flawlessly. Once reduced, the fragment is provisionally stabilized with 0.045-inch Kirschner wires. Definitive fixation is typically achieved using one or two 1.5 mm to 2.4 mm headless compression screws or cortical lag screws. It is an absolute imperative that the screw heads are countersunk at least 1 mm beneath the articular cartilage; prominent hardware will act like a milling cutter, rapidly destroying the capitellar cartilage during forearm rotation.

In instances where the fracture apex is highly comminuted, a large metaphyseal void may remain beneath the articular segment after reduction. In these complex Type II variants, simple screw fixation is biomechanically inadequate and will lead to secondary subsidence of the articular fragment under axial load. The surgeon must augment the construct by applying a small, low-profile buttress plate (often a 2.0 mm T-plate or dedicated radial neck plate) to physically support the articular surface and bridge the metaphyseal defect.
Fixation of Mason Type III Fractures
Mason Type III fractures demand a highly sophisticated approach. If the fracture is deemed reconstructable, the surgeon may need to extend the exposure by deliberately releasing the origin of the LUCL from the lateral epicondyle, tagging it with high-tensile, non-absorbable sutures for anatomic repair at the conclusion of the case.
In cases of severe comminution, attempting reduction in situ is often an exercise in futility. The preferred technique is "ex vivo reconstruction." The major articular fragments are carefully extracted from the joint, preserving any soft tissue attachments if possible, but prioritizing the retrieval of the bone. On the back table, the surgeon meticulously cleans the fracture edges and reassembles the radial head like a three-dimensional puzzle, securing the fragments with fine K-wires or miniature headless screws. This reconstructed "neoreadial head" is then re-implanted into the joint and secured to the radial neck.
Fixation to the radial shaft requires the application of a pre-contoured radial head plate. The absolute critical step here is positioning the plate strictly within the "safe zone"—the 110-degree non-articulating arc of the lateral radial head. The safe zone is identified intraoperatively by marking the midpoint of the lateral radial head with the forearm in neutral rotation; the boundaries are roughly defined by a line extending proximally from the radial styloid and another from Lister's tubercle.
The plate is secured with locking screws proximally to capture the small, often osteopenic articular fragments, and standard cortical screws distally in the radial diaphysis. If a structural void exists within the radial neck, it must be meticulously packed with cancellous autograft (harvested from the olecranon or lateral epicondyle) or high-quality allograft to promote osteoinduction and provide critical mechanical support against axial subsidence.


Prior to final closure, a dynamic fluoroscopic assessment is mandatory. The elbow is taken through a full arc of flexion, extension, pronation, and supination. The surgeon must visually and radiographically confirm that there is no hardware impingement at the PRUJ and that radiocapitellar tracking is smooth, congruent, and stable. Finally, the tagged LUCL is rigidly reattached to its isometric origin on the lateral epicondyle using robust suture anchors, restoring the lateral stabilizing column of the elbow.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of radial head fractures is fraught with potential complications. The complex anatomy, tenuous blood supply, and unforgiving biomechanical demands of the elbow joint create an environment where even minor technical errors can lead to profound functional deficits. The orthopedic surgeon must be acutely aware of these complications, their typical incidence rates, and the appropriate salvage pathways.
Posterior Interosseous Nerve (PIN) palsy is a devastating neurological complication, typically presenting as an inability to actively extend the digits and thumb. It is most commonly a neuropraxia secondary to aggressive, prolonged retraction rather than direct laceration. The risk is highest during the Kaplan approach and when dissecting distally along the radial neck. Prevention is entirely reliant on maintaining the forearm in full pronation during the exposure, which dynamically shifts the PIN anteriorly and medially, away from the retractor blades.
Hardware impingement and post-traumatic stiffness are the most frequent causes of a poor clinical outcome. If a plate or screw is inadvertently placed outside the 110-degree safe zone, it will mechanically block pronation and supination as it strikes the lesser sigmoid notch of the ulna. This requires prompt recognition and, once the fracture has achieved clinical and radiographic union, a secondary surgery for hardware removal. Post-traumatic stiffness (capsular contracture) is practically universal to some degree following elbow trauma. It is mitigated by rigid internal fixation that permits immediate, early active motion.
Avascular necrosis (AVN) and nonunion occur due to the precarious, retrograde intraosseous blood supply of the radial head. Extensive subperiosteal stripping during surgery exacerbates this ischemic insult. While some degree of radiographic AVN may be asymptomatic, progressive collapse of the articular segment leads to severe radiocapitellar arthritis, pain, and mechanical catching.
The following table summarizes the primary complications, their estimated incidence in the literature, and the standard salvage management strategies:
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| PIN Palsy | 2% - 5% | Retractor traction; anterior dissection; failure to pronate forearm. | Observation + EMG at 6 weeks. Tendon transfers if no recovery by 6-12 months. |
| Hardware Impingement | 5% - 15% | Plate/screws placed outside the 110° safe zone; prominent screw heads. | Hardware removal after radiographic union (typically > 6 months post-op). |
| Post-Traumatic Stiffness | 10% - 30% | Prolonged immobilization; severe initial trauma; heterotopic ossification. | Aggressive physical therapy; static progressive splinting; open or arthroscopic capsular release. |
| Nonunion / AVN | 5% - 10% | Extensive soft tissue stripping; severe comminution; inadequate fixation. | Late radial head excision (if IOM/MCL intact) or radial head arthroplasty. |
| Radiocapitellar Arthritis | 15% - 25% | Initial cartilage impaction injury; malreduction; hardware prominence. | Conservative management; late radial head excision or prosthetic replacement. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional success of a radial head ORIF is as dependent on a rigorously executed postoperative rehabilitation protocol as it is on the surgical osteosynthesis itself. The elbow is notoriously prone to rapid and severe capsular contracture following trauma; therefore, the primary objective of rehabilitation is to safely maximize range of motion while strictly protecting the healing bone and any associated ligamentous repairs. The protocol is heavily influenced by the security of the fixation and the presence of concomitant injuries (e.g., LUCL repair).
Phase I: Immediate Postoperative Phase (Days 0-7)
In the immediate postoperative period, the primary goals are edema control, pain management, and protection of the surgical construct. In the operating room, the arm is placed in a well-padded, custom-molded posterior plaster splint. The elbow is typically immobilized at 90 degrees of flexion with the forearm in neutral rotation. If a concurrent LUCL repair was performed, the forearm is strictly maintained in pronation to relax the lateral ligamentous complex and prevent tension on the suture anchors. Elevation and cryotherapy are aggressively utilized to minimize soft tissue swelling, which is a major contributor to early stiffness.
Phase II: Early Mobilization and Protection (Weeks 1-4)
At approximately 3 to 7 days postoperatively, assuming rigid internal fixation was achieved, the posterior splint is removed. The patient is transitioned to a supportive sling or a hinged elbow brace, depending on the degree of ligamentous instability. This phase marks the critical initiation of active and active-assisted range of motion (ROM) exercises.
* Motion Parameters: Patients are instructed to perform active flexion and extension within a pain-free arc. Pronation and supination are initiated with the elbow flexed at 90 degrees to minimize stress on the radiocapitellar joint.
* Strict Prohibitions: Passive stretching by physical therapists or forceful manipulation by the patient is absolutely contraindicated during this phase. Aggressive passive stretching incites an intense inflammatory response, exponentially increasing the risk of heterotopic ossification (HO) and potentially causing catastrophic failure of the osteosynthesis or ligament repairs.
Phase III: Progression and Weaning (Weeks 4-8)
By the fourth week, the patient should be entirely weaned from the sling or brace for activities of daily living. The focus shifts to achieving terminal extension and full supination/pronation, which are historically the most difficult arcs of motion to regain. Static progressive splinting (e.g., turnbuckle splints) may be introduced at 6 weeks if the patient has plateaued in their active ROM recovery and radiographic evidence of early fracture consolidation is present. Isometrics can be initiated, but heavy lifting remains restricted.
Phase IV: Strengthening and Return to Function (Weeks 8-12+)
Once definitive clinical and radiographic union is confirmed (typically between 8 and 12 weeks), progressive resistive exercises and formal strengthening programs are initiated. The focus is on restoring the strength of the biceps, triceps, and forearm musculature. Return to heavy manual labor, contact sports, or high-impact activities is generally delayed until 4 to 6 months postoperatively, contingent upon the restoration of near-normal strength and
