Radial Head Fractures: Comprehensive Epidemiology, Classification, Anatomy & Biomechanics

Key Takeaway
Radial head fractures are elbow injuries classified by Mason-Hotchkiss (Types I-IV) based on displacement. Associated injuries like MCL/LCL tears are critical. Understanding surgical anatomy, the radial head's role in axial load and forearm rotation, plus overall elbow biomechanics, is paramount for guiding effective treatment and restoring long-term function.
A 35-year-old male presents to the Emergency Department following a fall onto an outstretched hand (FOOSH) during a football match. He complains of significant lateral elbow pain. Clinically, he has limited forearm rotation. Please interpret the provided radiograph.
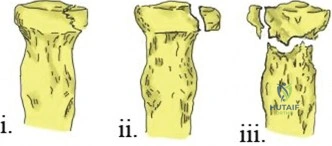
Candidate: The radiograph shows a displaced fracture of the radial head. Based on the Mason-Hotchkiss classification, this is a Type II or possibly Type III fracture, given the displacement and comminution. I would assess for a mechanical block to rotation and look for associated injuries like a coronoid fracture or ligamentous instability.
Focusing only on the radial head fracture. A failing candidate fails to mention the "Hidden" dangers of the elbow, such as the LCL complex, Essex-Lopresti injuries, or the status of the distal radioulnar joint (DRUJ). They also fail to ask for a CT scan to confirm comminution.
I see a displaced, comminuted radial head fracture. I would classify this as Mason-Hotchkiss Type II/III. My primary concern is the 'Terrible Triad' or an Essex-Lopresti variant. I would perform a physical exam to check for mechanical block, valgus/varus stability, and DRUJ tenderness. I would request a CT scan to delineate the articular surface and rule out associated coronoid fractures, and I would maintain a high index of suspicion for LCL complex injury.
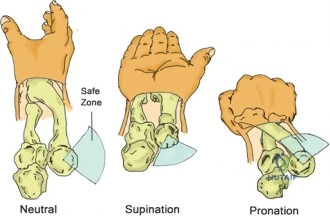
You have decided to proceed to surgery for this patient. During the lateral approach, you need to be mindful of specific anatomical structures to avoid iatrogenic injury. Which nerve is most at risk, and how do you protect it?
Candidate: The Posterior Interosseous Nerve (PIN) is the main structure at risk. It passes through the supinator muscle. I would keep the forearm in full supination during the approach to move the nerve anteriorly, away from the path of my dissection.
Saying "I would be careful" or "I would look for it." In the FRCS exam, you must provide the specific anatomical maneuver (supination) that moves the nerve away from the danger zone. Simply stating you will avoid it is insufficient.
The Posterior Interosseous Nerve is at risk as it exits the supinator. To protect it, I perform the dissection with the forearm in full supination, which rotates the PIN anteriorly, keeping it away from the lateral surgical field. Furthermore, I would limit the proximal extension of the dissection to avoid the radial nerve branches.
The fracture is comminuted and considered unreconstructible. What are your indications for radial head arthroplasty (RHA) versus simple excision of the radial head fragment?

Candidate: Excision is now rarely indicated because the radial head is a stabilizer. I would use an RHA if there is associated ligamentous injury, an Essex-Lopresti injury, or if the patient is high demand, to restore stability and prevent proximal migration of the radius.
Suggesting excision for a young, active patient. Excision leads to valgus instability and ulnar impaction syndrome. Failing to explicitly state why RHA is needed (restoration of axial load transmission) is a significant omission.
Excision is largely historical and reserved for low-demand, elderly patients with isolated fractures. I prefer RHA in virtually all active patients with comminuted fractures because the radial head transmits 60-80% of axial load and provides secondary valgus stability. Replacing it restores radial length, preventing longitudinal radioulnar dissociation (Essex-Lopresti syndrome) and protecting the medial collateral ligament.
