Proximal Hamstring and Adductor Lengthening for Spastic Hip Subluxation: An Intraoperative Masterclass

Key Takeaway
Join a master surgeon in the OR for a detailed guide on proximal hamstring and adductor lengthening. Learn crucial steps from incision to closure, focusing on neurovascular protection, precise myotomy, and managing spastic hip subluxation in children. Understand preoperative planning, intraoperative pearls, and postoperative care for optimal outcomes.
Comprehensive Introduction and Patho-Epidemiology
The Burden of Spastic Hip Disease
Welcome, colleagues and fellows, to the operating theater. Today, we are addressing one of the most critical, yet frequently insidious, aspects of pediatric orthopaedics: the management of spastic hip subluxation through proximal hamstring and adductor lengthening. This procedure is paramount in the armamentarium of the pediatric orthopaedic surgeon, serving as a prophylactic bulwark against progressive hip displacement, articular degeneration, and debilitating pain in our young patients with cerebral palsy (CP). Spastic hip displacement is the second most common orthopaedic deformity in CP, superseded only by equinus contracture of the ankle. The incidence of hip displacement is directly correlated with the severity of neurological impairment, reaching up to 90% in patients classified as Gross Motor Function Classification System (GMFCS) level V.
Without timely intervention, the natural history of this condition is a relentless progression from silent subluxation to frank dislocation, culminating in severe pelvic obliquity, sitting intolerance, and intractable pain that severely diminishes the patient's quality of life. The socioeconomic and psychological burdens on the caregivers are equally profound, as a dislocated, painful hip severely complicates perineal hygiene, transfers, and wheelchair seating. Therefore, our mandate is clear: we must identify hips at risk early and intervene decisively. Soft tissue lengthening remains the gold standard for intercepting this pathological cascade before irreversible bony architectural distortion necessitates highly invasive, morbid reconstructive osteotomies.
To truly master this intervention, the orthopaedic surgeon must look beyond the gross deformity and appreciate the microscopic and macroscopic forces at play. We are not merely cutting tendons; we are recalibrating a profoundly deranged biomechanical system. The success of this operation relies heavily on patient selection, precise timing, and an uncompromising adherence to meticulous surgical technique. As we proceed through this masterclass, we will deconstruct every facet of this procedure, from the foundational patho-epidemiology to the nuanced intraoperative decision-making required to achieve optimal, durable outcomes.
Pathophysiology of Muscle Imbalance
Before we make our first incision, we must establish a crystal-clear understanding of the underlying pathoanatomy. Spastic hip disease is fundamentally a pathology of dynamic force imbalance that eventually dictates static bony deformity. In the typically developing child, normal muscle balance and weight-bearing forces stimulate the proper development of the proximal femur and acetabulum. The physiological forces of walking and standing promote the gradual reduction of fetal femoral anteversion and coxa valga, while simultaneously deepening the acetabulum through concentric pressure from the femoral head. In the spastic patient, however, a profound and pervasive imbalance exists, disrupting this elegant developmental synergy.
The adductors, flexors, and hamstrings exhibit hypertonia and spasticity, overpowering the relatively weaker abductors and extensors. This persistent, asymmetrical pull creates an abnormal force vector across the hip joint. Initially, this manifests as a dynamic contracture—a limitation of hip abduction with the hips and knees extended, which is the hallmark clinical finding. Over time, this dynamic state induces structural changes within the muscle-tendon units themselves. Histological analyses of spastic muscle reveal a significant reduction in serial sarcomeres, increased deposition of rigid extracellular matrix proteins, and alterations in the titin filaments. This translates clinically to a fixed myostatic contracture, where the muscle physically shortens and loses its physiological excursion.
Furthermore, the chronic hypertonicity leads to a state of constant metabolic stress within the muscle belly, precipitating fibrosis and fatty infiltration. This fibrotic transformation renders the muscle highly resistant to conservative stretching protocols and pharmacological interventions like botulinum toxin type A. Once myostatic contracture is established, the abnormal biomechanical vectors become permanently entrenched, exerting a continuous, unyielding deforming force on the developing skeleton. It is at this critical juncture that surgical lengthening transitions from an elective consideration to an absolute necessity.
Natural History and Progression
The primary period during which spastic hip disease typically manifests and accelerates is between 2 and 8 years of age. During this critical window of skeletal growth, the unyielding spastic forces act upon the highly malleable cartilaginous anlagen of the proximal femur and acetabulum. The constant adduction and flexion forces prevent the normal resolution of fetal coxa valga and femoral anteversion. Consequently, the femoral head is driven posterosuperiorly against the lateral margin of the acetabulum.
This eccentric pressure inhibits normal acetabular development, leading to a shallow, dysplastic acetabulum that further facilitates subluxation. It is a vicious, self-perpetuating cycle: muscle imbalance causes subluxation, which causes bony dysplasia, which in turn exacerbates the subluxation. As the femoral head migrates laterally, the capsule becomes attenuated anteriorly and contracted posteriorly, creating a secondary soft-tissue barrier to reduction. If left unchecked, the femoral head will eventually breach the confines of the acetabulum, resulting in a paralytic dislocation.
Our intervention today is designed to decisively break this cycle by neutralizing the deforming muscular forces. By releasing the adductors and proximal hamstrings, we aim to restore a more concentric seating of the femoral head within the acetabulum. If performed early enough in the child's development, this concentric seating can stimulate remodeling of the dysplastic acetabulum—a phenomenon often referred to as "acetabular catch-up growth." However, if we miss this therapeutic window, the bony dysplasia becomes fixed, and soft tissue release alone will inevitably fail, condemning the child to complex pelvic and femoral reconstructions.
Detailed Surgical Anatomy and Biomechanics
The Adductor Compartment and Obturator Nerve
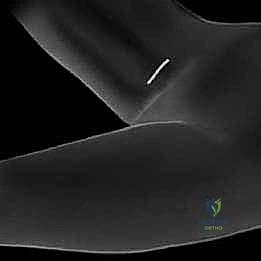
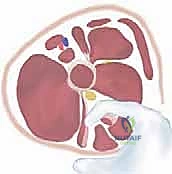
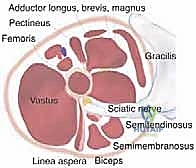
A profound mastery of the medial thigh anatomy is non-negotiable for this procedure. The adductor compartment is arranged in three distinct layers, all innervated primarily by the obturator nerve. The superficial layer comprises the adductor longus and the gracilis. The adductor longus arises from the anterior body of the pubis and fans out to insert on the linea aspera of the femur. It is a powerful adductor and a secondary flexor of the hip. The gracilis, the most medial muscle, originates from the inferior pubic ramus and is the only biarticular muscle of the medial group, crossing both the hip and the knee to insert on the pes anserinus.
Deep to these superficial structures lies the middle layer, consisting solely of the adductor brevis. The adductor brevis originates from the inferior pubic ramus, deep to the adductor longus, and inserts on the pectineal line and upper linea aspera. The deep layer is formed by the massive adductor magnus, a hybrid muscle with both adductor and hamstring components, innervated by both the obturator and sciatic nerves. For the purposes of prophylactic soft tissue release, our focus is almost exclusively on the superficial and middle layers. Releasing the adductor magnus is generally contraindicated, as it can lead to devastating over-lengthening and an iatrogenic abduction contracture.
Crucially, the obturator nerve exits the obturator canal and immediately divides into anterior and posterior branches. The anterior branch descends anterior to the adductor brevis (between it and the adductor longus/gracilis), while the posterior branch descends posterior to the adductor brevis (between it and the adductor magnus). Precise identification and protection of the anterior branch during adductor longus and brevis lengthening are paramount. Inadvertent transection of this nerve leads to global adductor denervation, resulting in severe abduction contractures, pelvic obliquity, and profound gait deterioration in ambulatory patients.
The Proximal Hamstring Complex and Sciatic Nerve
The hamstrings are a significant, yet historically underappreciated, contributor to spastic hip subluxation. The proximal hamstring complex originates from the ischial tuberosity and consists of the biceps femoris (long head), semitendinosus, and semimembranosus. In the context of spasticity, the hamstring attachments on the pelvis are typically broad, hypertrophied muscular origins lacking substantial tendinous components. This anatomical reality often dictates that our surgical release is a myotomy rather than a simple tenotomy, requiring careful hemostasis due to the rich vascular supply of the muscle bellies.
The critical exception—and a focal point of surgical vigilance—is the semimembranosus, which tends to possess a more distinct tendinous insertion laterally on the ischium. Just lateral and deep to this complex lies the sciatic nerve, the largest nerve in the human body. In a contracted, spastic patient, the anatomical planes are often severely distorted. The chronic flexion contracture of the hip and knee can cause the sciatic nerve to bowstring medially, bringing it dangerously close to the surgical field during a proximal hamstring release.
Furthermore, the tense semimembranosus tendon can easily be mistaken for the sciatic nerve by an unwary surgeon. Meticulous blunt dissection, strict adherence to anatomical planes, and the judicious use of an intraoperative nerve stimulator are essential safeguards. The surgeon must visually confirm the identity of the tendinous structures before applying electrocautery. A catastrophic sciatic nerve injury during this prophylactic procedure is an inexcusable complication that carries devastating lifelong consequences for the patient.
Biomechanical Vectors of Hip Displacement
Biomechanically, advanced musculoskeletal modeling studies have elucidated the precise vectors driving spastic hip disease. The adductors exert a massive medial and proximal force vector, effectively squeezing the femoral head out of the acetabulum. However, the hamstrings are equally culpable. Their spasticity not only drives hip extension but, more importantly, maintains the knees in a chronically flexed position. This obligate knee flexion secondarily encourages hip flexion to maintain balance and an upright sitting posture, effectively shortening the lever arm of the lower extremity.
Combined with spastic hip flexors (primarily the iliopsoas), the limb falls into a characteristic posture of internal rotation, flexion, and adduction. The hamstrings, therefore, act as a rigid tether across the posterior pelvis, magnifying the adverse influence of the concomitant spastic adductors. This posterior tethering prevents the pelvis from tilting anteriorly, forcing the lumbar spine into hyperlordosis and further destabilizing the hip joint mechanics. The resulting "windblown" pelvic deformity is a hallmark of neglected spastic hip disease.
By releasing both the adductors and the proximal hamstrings simultaneously, we neutralize the combined posterosuperior and medial vectors. This comprehensive release allows the femoral head to rest concentrically within the acetabulum, dropping the proximal femur away from the lateral acetabular rim. It permits normal physiological forces to guide subsequent bony development. Furthermore, releasing the hamstrings improves knee extension, which in turn reduces the compensatory hip flexion, breaking the biomechanical chain of contractures that drives progressive subluxation.
Exhaustive Indications and Contraindications
Clinical and Radiographic Thresholds
The decision to proceed with soft tissue release for spastic hip subluxation is predicated on a careful, multidisciplinary synthesis of clinical examination and radiographic metrics. The indications for this procedure are highly specific and must be strictly adhered to. We target children typically between the ages of 2 and 8 years, representing the optimal window of skeletal immaturity where acetabular remodeling is still possible. While some adolescents remain at risk and require intervention, the capacity for bony remodeling drops precipitously after age 8.
The primary radiographic criterion is a Reimers Migration Index (MI) between 30% and 60%. An MI less than 30% is generally observed with watchful waiting, while an MI greater than 60% almost universally indicates significant secondary bony dysplasia (coxa valga, severe anteversion, acetabular flattening). At an MI > 60%, soft tissue release alone is doomed to fail; these patients necessitate concurrent femoral varus derotational osteotomy (VDRO) and often a pelvic osteotomy (e.g., Dega or San Diego).
Clinically, the patient must exhibit limited hip abduction—specifically, less than 30 degrees with the hips and knees extended. This measurement must be taken with the pelvis stabilized to prevent false abduction through pelvic tilt. Furthermore, a popliteal angle greater than 45 degrees strongly implicates the hamstrings in the pathological contracture cascade, necessitating their inclusion in the surgical release. Failure to address tight hamstrings when performing an adductor release will result in persistent posterior pelvic tethering and a high rate of recurrent subluxation.
The Role of Examination Under Anesthesia
A critical caveat that must be emphasized to all orthopaedic trainees: the clinical examination in the clinic is often confounded by the child's voluntary resistance, anxiety, and dynamic spasticity. Therefore, the definitive assessment determining the extent of surgical release must be performed under general anesthesia prior to prepping and draping. Once the patient is anesthetized, the dynamic component of spasticity is abolished, revealing the true underlying myostatic contracture.
If hip abduction normalizes to greater than 45 degrees under anesthesia, the contracture is purely dynamic. In this scenario, surgical lengthening may be overly aggressive, and non-operative modalities such as botulinum toxin injections, serial casting, or intensive physical therapy should be prioritized. Conversely, if abduction remains restricted to less than 30 degrees under anesthesia, fixed structural shortening of the muscle-tendon unit has occurred, and surgical lengthening is unequivocally indicated.
The Examination Under Anesthesia (EUA) also allows for a precise assessment of the hamstrings. By measuring the popliteal angle with the hip flexed to 90 degrees, the surgeon can determine the severity of hamstring contracture without the influence of patient guarding. A popliteal angle that remains greater than 45-50 degrees under anesthesia confirms the need for a proximal hamstring release. The EUA is the ultimate arbiter of the surgical plan; what is planned in the clinic is merely a hypothesis until proven in the operating room.
Summary Table of Indications and Contraindications
| Category | Parameters / Conditions | Rationale / Clinical Significance |
|---|---|---|
| Primary Indications | Reimers Migration Index 30% - 60% | Indicates progressive subluxation without absolute dislocation; optimal window for soft tissue intervention. |
| Age 2 to 8 years (typically) | Optimal window to prevent irreversible bony dysplasia and allow for acetabular remodeling. | |
| Hip Abduction < 30° (under anesthesia) | Confirms fixed myostatic contracture of the adductor complex requiring surgical lengthening. | |
| Popliteal Angle > 45° (under anesthesia) | Confirms significant hamstring contracture contributing to posterior pelvic tilt and subluxation. | |
| Absolute Contraindications | Reimers Migration Index > 60% | High likelihood of severe bony dysplasia requiring VDRO and/or Pelvic Osteotomy; soft tissue release alone will fail. |
| Fixed Pelvic Obliquity with Spinal Deformity | Soft tissue release alone will fail to balance the pelvis; requires comprehensive spinal/pelvic balancing first. | |
| Completely Dislocated Hip (MI = 100%) | Soft tissue release is insufficient; requires open reduction, capsulorrhaphy, and extensive bony reconstruction. | |
| Medical Instability | Severe respiratory or cardiac compromise precluding safe general anesthesia. | |
| Relative Contraindications | Purely Dynamic Contracture | Full range of motion achieved under anesthesia; consider non-operative modalities (Botox, casting) first. |
| Extrapyramidal / Dystonic CP | Unpredictable postoperative tone changes can lead to severe reverse deformities (iatrogenic abduction contractures). | |
| Previous Extensive Adductor Releases | High risk of over-lengthening and scarring; requires careful assessment for bony surgery instead. |
Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Analysis and the Reimers Migration Index
Surgical success begins with meticulous preoperative radiographic analysis. Our primary investigative tool is the supine anteroposterior (AP) pelvic radiograph, taken with the patellae facing strictly forward to neutralize the effect of femoral anteversion. Allowing the legs to externally rotate will artificially decrease the apparent neck-shaft angle and obscure the true extent of lateral migration. On this standardized image, we calculate the Reimers Migration Index, the universally accepted metric for hip displacement in CP.
This calculation is performed by drawing Hilgenreiner's line horizontally through the triradiate cartilages, followed by Perkins' line dropped perpendicularly from the lateral margin of the ossified acetabular roof. We then measure the total width of the femoral head and the width of the portion lying lateral to Perkins' line. The lateral width divided by the total width, expressed as a percentage, yields the MI. An MI of 25% or less is considered normal; greater than 30% defines subluxation.
Beyond the MI, we must scrutinize the radiograph for early signs of acetabular dysplasia. The Acetabular Index (AI) should be measured; an AI greater than 25-30 degrees in a child over 4 years old is highly concerning for dysplasia. We also evaluate the femoral neck-shaft angle to assess for severe coxa valga, and look for any "breaking" of the Shenton-Menard line. If severe bony architectural changes are present alongside an MI nearing 60%, the surgeon must seriously consider whether soft tissue release alone is a futile endeavor, and prepare the family for the likelihood of future bony reconstruction.
Operating Room Setup and Anesthesia Considerations
Communication with the anesthesia team is a critical component of the preoperative briefing. The anesthesiologist must be explicitly instructed not to use long-acting neuromuscular blocking agents (paralytics) during the procedure. We require the ability to utilize a handheld nerve stimulator to positively identify and protect the anterior branch of the obturator nerve and the sciatic nerve. Complete paralysis renders this vital safety check impossible, blinding the surgeon to the proximity of these critical neurological structures.
The operating room should be equipped with a standard radiolucent table to allow for intraoperative fluoroscopy if necessary. While this is primarily a soft-tissue procedure, fluoroscopy can be invaluable if there is a question about the concentricity of the reduction post-release, or if an occult dislocation is suspected. High-quality focal lighting, such as a surgeon-worn headlight, is highly recommended, as the medial groin approach involves working in a deep, relatively narrow cavity. Appropriate pediatric soft-tissue retractors—specifically small Richardson, Langenbeck, and right-angle retractors—must be available on the sterile field.
Blood loss is typically minimal in this procedure, but the highly vascular nature of the spastic muscle bellies means that meticulous hemostasis is required. Bipolar electrocautery should be available to manage bleeding near neurovascular structures safely. A warming blanket (Bair Hugger) is essential, as pediatric patients with CP often have poor thermoregulation and minimal subcutaneous fat, making them highly susceptible to intraoperative hypothermia.
Patient Positioning and Intraoperative Assessment
The patient is positioned supine on the operating table. Careful padding of all bony prominences is mandatory. Children with CP often have poor nutritional status, fragile skin, and severe contractures that place unusual pressure on the sacrum, heels, and occiput, predisposing them to rapid pressure necrosis. Both lower extremities must be prepped and draped freely to allow for unimpeded, dynamic intraoperative assessment of the range of motion. We utilize a sterile adhesive U-drape to isolate the perineum and groin, defining our surgical boundaries cleanly while minimizing contamination risk from the perineal region.
Before making the incision, a formal examination under anesthesia (EUA) is conducted and documented. We carefully measure and record maximum hip abduction with hips and knees extended, maximum hip extension (Thomas test), and the bilateral popliteal angles. These baseline measurements are crucial for determining the necessary extent of the release.
Our intraoperative benchmark for a successful procedure is achieving bilateral hip abduction of greater than 45 degrees with minimal passive force at the conclusion of the releases. Furthermore, the popliteal angle should be reduced to less than 20-30 degrees. If these benchmarks are not met after releasing the adductor longus, gracilis, and proximal hamstrings, the surgeon must systematically evaluate the adductor brevis and the medial hamstrings for residual tethering, progressively releasing tight structures until the desired range of motion is achieved without tension.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
We utilize the medial groin approach, which allows access to both the adductor complex and the proximal hamstrings through a single, cosmetically acceptable incision, avoiding the pressure-sensitive posterior weight-bearing area of the ischium.
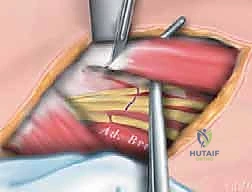
"Scalpel, please. We begin with a transverse incision, approximately 2 to 3 cm posterior to the palpable anterior border of the adductor longus muscle, situated in the proximal groin crease. This incision extends for about 3-4 cm, meticulously following Langer's lines to optimize the final cosmetic outcome."
"Using careful sharp and blunt dissection through the subcutaneous adipose tissue, we identify the deep fascia overlying the adductor compartment. We utilize gentle spreading with Metzenbaum scissors to sweep away the overlying lymphatics and superficial veins, isolating the anterior border of the adductor longus. Hemostasis in the subcutaneous layer must be absolute to prevent postoperative hematoma."
Adductor Longus and Gracilis Release
"Once the epimysium of the adductor longus is clearly visualized, we incise it longitudinally to expose the muscle belly. Notice the distinct orientation of the muscle fibers. The adductor longus is typically the most prominent and tightest structure encountered initially."
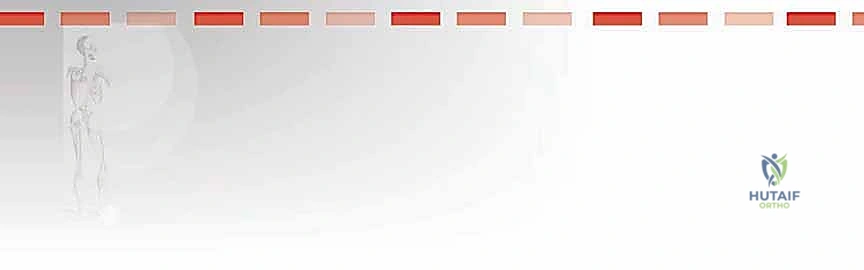
"We pass a right-angle clamp deep to the adductor longus to isolate it. Crucial Step: Before applying electrocautery, we must sweep the deep tissues with a peanut sponge or nerve hook to ensure the anterior branch of the obturator nerve is not adhering to the deep surface of the muscle. Once confirmed safe, we perform a complete myotendinous transection of the adductor longus using electrocautery, allowing the ends to retract."
"Immediately posterior and slightly deep to the adductor longus lies the gracilis. We incise its investing fascia. The gracilis is identified by its distinct, more vertically oriented fibers and its position as the most medial structure."
"Similar to the longus, we isolate the gracilis with a right-angle clamp. We must be cautious of the terminal branches of the medial circumflex femoral artery in this region. After confirming isolation, the gracilis is transected. At this point, we reassess hip abduction. If abduction remains tight (less than 40 degrees), we proceed to evaluate the adductor brevis."
Proximal Hamstring Approach and Sciatic Nerve Protection
"With the superficial adductors released, we now turn our attention to the proximal hamstrings. Retracting the posterior skin edge, we palpate the ischial tuberosity. The dissection proceeds bluntly, posterior to the adductor magnus, heading towards the ischium."
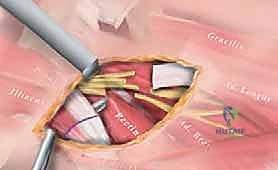
"We identify the common origin of the proximal hamstrings on the ischial tuberosity. The tissue here is often thick and fibrotic in spastic patients. We use a combination of blunt finger dissection and careful spreading with scissors to define the medial and lateral borders of the hamstring mass."

"Before any cutting occurs, we must definitively locate and protect the sciatic nerve, which lies just lateral and deep to the hamstring complex. We utilize a nerve stimulator set to 1.0-2.0 mA. We probe the lateral aspect of the field. A twitch in the foot or calf confirms the location of the sciatic nerve."
"Once the sciatic nerve is safely identified and gently retracted laterally, we isolate the semimembranosus and semitendinosus. The semimembranosus often has a distinct tendinous band that must be released. We perform a fractional lengthening or myotomy of these structures, carefully preserving the biceps femoris if possible to prevent excessive weakness in knee flexion."
"Following the release, we observe a significant gap in the muscle-tendon units, indicating a successful lengthening. We perform a final, rigorous check of the range of motion. We expect to see a popliteal angle of less than 30 degrees and hip abduction exceeding 45-50 degrees without tension."
"The wound is thoroughly irrigated. Hemostasis is meticulously achieved using bipolar electrocautery. We close the deep subcutaneous layer with interrupted 3-0 absorbable sutures to eliminate dead space, and the skin is closed with a running 4-0 subcuticular stitch, followed by Dermabond or steri-strips. No drains are typically required."
Complications, Incidence Rates, and Salvage Management
Over-Lengthening and Reverse Deformities
The most feared complication of soft tissue release in the spastic hip is iatrogenic over-lengthening, which can lead to severe reverse deformities. If the adductor complex is excessively released—particularly if the adductor magnus is inadvertently transected—the relatively unopposed abductors (gluteus medius and minimus) will pull the hip into a fixed abduction contracture. This creates a devastating functional impairment, rendering the patient unable to sit in a standard wheelchair, complicating perineal care, and causing severe pelvic obliquity that can precipitate secondary scoliosis.
The incidence of severe over-lengthening is highly variable, reported between 2% and 10% in the literature, and is highly
