Proximal Femoral Derotational Osteotomy: An Operative Masterclass with 90-Degree AO Blade Plate

Key Takeaway
Join us in the OR for a comprehensive masterclass on proximal femoral derotational osteotomy using a 90-degree AO blade plate. We'll meticulously cover patient selection, precise anatomical considerations, detailed preoperative planning, and a granular, step-by-step intraoperative execution. Learn critical pearls, avoid common pitfalls, and master postoperative management for optimal outcomes in correcting femoral anteversion.
Comprehensive Introduction and Patho-Epidemiology
Proximal femoral derotational osteotomy (PFDRO) utilizing a 90-degree AO blade plate represents a foundational procedure in the armamentarium of the pediatric and reconstructive orthopedic surgeon. This operative masterclass delineates the meticulous planning, precise anatomical navigation, and rigorous biomechanical principles required to execute this procedure flawlessly. The primary objective is the surgical correction of pathological femoral anteversion, a condition that, while often physiologic in early childhood, can persist and precipitate profound functional, kinematic, and degenerative sequelae if left unaddressed.
Biomechanics of Femoral Anteversion
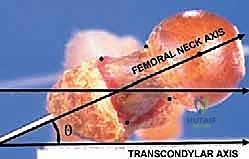
Femoral anteversion is defined geometrically as the angle in the transverse plane by which the axis of the femoral neck is rotated anteriorly relative to the transcondylar axis of the distal femur (the coronal plane of the knee). This angular relationship dictates the spatial orientation of the femoral head within the acetabulum during the gait cycle.
At birth, the physiologic anteversion angle typically ranges from 30 to 50 degrees. In a neurotypical child, the onset of weight-bearing activities—such as crawling, cruising, and independent ambulation—initiates a gradual, spontaneous "unwinding" of this torsional alignment. This physiological remodeling is driven by the repetitive extension of the hip against the robust anterior capsular structures, predominantly the iliofemoral ligament (Y-ligament of Bigelow). By the cessation of skeletal maturity, the normative adult anteversion angle stabilizes between 10 and 15 degrees.
Pathogenesis and Clinical Presentation
When this spontaneous derotation fails to occur, or is pathologically impeded by neuromuscular imbalances, the patient develops persistent increased femoral anteversion. To achieve congruous seating of the femoral head within the acetabular vault, the patient must internally rotate the entire lower extremity. This compensatory mechanism invariably leads to a constellation of clinical signs, most notably an internal foot progression angle (in-toeing) during the stance phase of gait.

Clinically, these children demonstrate a pathognomonic preference for the "W-sitting" posture. This position is adopted because their arc of hip internal rotation is massively augmented, often exceeding 70 to 80 degrees, while external rotation is concomitantly restricted to 10 degrees or less. Sitting cross-legged (tailor sitting) places the hips in external rotation, which is anatomically restricted and uncomfortable for these patients. Furthermore, the persistent internal rotation of the femur alters the vector of the abductor musculature, leading to lever arm dysfunction. To maintain sagittal balance, patients frequently develop a compensatory anterior pelvic tilt, which in turn exacerbates lumbar lordosis, predisposing them to early-onset axial back pain.
Associated Pathologies and Syndromic Presentations
Increased femoral anteversion rarely exists in an anatomical vacuum. It is frequently a critical component of complex, multi-level orthopedic conditions. In the context of Cerebral Palsy (CP), spasticity of the medial hamstrings, adductors, and iliopsoas overpowers the external rotators, preventing the normal unwinding of the femur. This resulting anteversion, often coupled with coxa valga, drastically reduces the mechanical advantage of the gluteus medius, precipitating a Trendelenburg gait and predisposing the hip to progressive subluxation and eventual dislocation.
In Developmental Dysplasia of the Hip (DDH), excessive anteversion prevents concentric reduction of the femoral head, necessitating derotational osteotomy as an adjunct to open reduction or pelvic osteotomies. Furthermore, in "Miserable Malalignment Syndrome," the proximal femoral anteversion is coupled with compensatory external tibial torsion and frequently genu valgum. This torsional mismatch generates extreme sheer forces across the patellofemoral joint, resulting in intractable anterior knee pain, patellar instability, and premature chondromalacia.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the proximal femoral anatomy and the surrounding myofascial envelopes is non-negotiable for the safe and efficacious execution of a proximal femoral derotational osteotomy. The surgical approach mandates navigation through highly vascularized muscular intervals while respecting critical biomechanical fulcrums.
Osteology of the Proximal Femur
The proximal femur consists of the femoral head, neck, and the intertrochanteric and subtrochanteric regions of the shaft. The greater trochanter serves as the paramount lateral bony landmark and the primary insertion site for the abductor complex (gluteus medius and minimus). Its spatial orientation is our primary intraoperative proxy for assessing femoral anteversion. The lesser trochanter, situated posteromedially, marks the insertion of the iliopsoas tendon. The intertrochanteric line anteriorly and the intertrochanteric crest posteriorly demarcate the junction between the neck and the shaft. The linea aspera, a longitudinal ridge on the posterior diaphysis, serves as the origin for the vastus lateralis and the insertion for the adductor magnus.
Myology and the Lateral Approach
The standard exposure for a 90-degree AO blade plate is the direct lateral approach. The initial dissection traverses the subcutaneous tissues to expose the fascia lata, a dense, fibrous sheath that must be incised longitudinally. Deep to the fascia lata lies the vastus lateralis, the largest constituent of the quadriceps femoris.
The vastus lateralis originates from the intertrochanteric line, the anterior and inferior borders of the greater trochanter, the lateral lip of the gluteal tuberosity, and the proximal half of the linea aspera. To expose the lateral femoral cortex, the vastus lateralis must be mobilized. This is achieved via an L-shaped or J-shaped incision. The transverse limb of the incision releases the muscle from the vastus ridge at the base of the greater trochanter, while the longitudinal limb splits the muscle fibers or elevates the muscle off the lateral intermuscular septum. It is imperative to leave a robust 1-2 cm cuff of tendinous tissue proximally at the vastus ridge to facilitate a secure, watertight repair during closure.
Neurovascular Considerations
While the lateral approach is generally devoid of major axial neurovascular bundles, it is fraught with localized vascular hazards. The most critical structures encountered are the perforating branches of the profunda femoris artery. As the vastus lateralis is elevated off the linea aspera and the lateral intermuscular septum, these perforators are predictably encountered traversing from posterior to anterior. They must be meticulously identified, isolated, and ligated or coagulated with electrocautery. Failure to secure these vessels can result in profound intraoperative hemorrhage, postoperative hematoma formation, and subsequent wound complications.
The sciatic nerve lies deep and posterior to the femur. While not routinely visualized during a standard lateral approach, aberrant retractor placement—specifically, plunging a Hohmann retractor too aggressively posterior to the linea aspera—can cause iatrogenic compression or neuropraxia. The femoral nerve and artery reside safely in the anterior compartment, well protected by the intervening bulk of the vastus intermedius and rectus femoris.
Exhaustive Indications and Contraindications
The decision to proceed with a proximal femoral derotational osteotomy must be predicated on a rigorous evaluation of the patient's symptoms, functional deficits, and objective kinematic data. Prophylactic surgery in the absence of functional impairment is strongly discouraged.
Indications for Surgical Intervention
Surgical management is indicated when conservative measures have failed, and the torsional deformity significantly degrades the patient's quality of life or biomechanical efficiency.
- Symptomatic Idiopathic Anteversion: In neurologically intact children over the age of 8 to 10 years, where spontaneous remodeling has ceased, and severe in-toeing causes frequent tripping, clumsiness, and an inability to participate in peer-level physical activities.
- Cerebral Palsy and Neuromuscular Disorders: To correct severe internal rotation gait that causes lever arm dysfunction of the hip abductors. Furthermore, it is a critical component of reconstructive surgery for hip subluxation or dislocation, often combined with a varus-producing osteotomy (VDRO) and pelvic osteotomies (e.g., Dega or San Diego).
- Miserable Malalignment Syndrome: In adolescents or young adults presenting with intractable patellofemoral pain or instability driven by the combination of femoral anteversion and compensatory external tibial torsion.
- Developmental Dysplasia of the Hip (DDH): As an adjunct procedure during open reduction when excessive anteversion prevents stable, concentric seating of the femoral head within the true acetabulum.
Contraindications to Surgery
Patient selection is paramount to avoid unnecessary morbidity and suboptimal outcomes.
- Age Under 8 Years (Idiopathic): In neurologically normal children under 8 years of age, spontaneous resolution of anteversion is still highly probable. Surgery is contraindicated unless the deformity is extraordinarily severe and causing unmanageable functional deficits.
- Asymptomatic Presentation: Cosmetic concerns alone, in the absence of functional impairment, tripping, or pain, do not justify the risks of major reconstructive bone surgery.
- Severe Fixed Pelvic Obliquity: In non-ambulatory patients with severe, rigid spinal deformities and pelvic obliquity, isolated femoral derotation may fail to improve seating or hygiene and could potentially unmask hip instability.
- Active Infection: Any active local or systemic infection is an absolute contraindication to elective orthopedic hardware implantation.
Summary Table: Indications and Contraindications
| Category | Specific Condition | Rationale |
|---|---|---|
| Absolute Indications | CP with progressive hip subluxation (Reimers Migration Index > 30-40%) | Restores articular congruity, prevents painful dislocation, and improves abductor mechanics. |
| Absolute Indications | Intractable Miserable Malalignment Syndrome | Corrects the proximal torsional driver of patellofemoral shear forces. |
| Relative Indications | Idiopathic anteversion > 50° in a 10-year-old with frequent tripping | Improves gait mechanics and prevents peer-exclusion due to clumsiness. |
| Absolute Contraindications | Active osteomyelitis or septic arthritis | High risk of hardware seeding and catastrophic joint destruction. |
| Relative Contraindications | Idiopathic anteversion in a 5-year-old | High likelihood of spontaneous physiological remodeling; observation is standard of care. |
| Relative Contraindications | Asymptomatic in-toeing (purely cosmetic) | The risks of general anesthesia, nonunion, and hardware complications outweigh cosmetic benefits. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a proximal femoral derotational osteotomy is inextricably linked to the diligence of the preoperative planning phase. The surgeon must quantify the deformity, select the appropriate implant, and orchestrate the operating room setup to facilitate seamless intraoperative execution.
Clinical and Kinematic Assessment
The physical examination remains the cornerstone of preoperative assessment. With the patient positioned prone, the examiner assesses the rotational profile of the hip. The arc of internal rotation is measured by allowing the tibia to fall outward, while external rotation is measured by bringing the tibia inward across the midline. In pathological anteversion, internal rotation frequently exceeds 70 degrees, with external rotation limited to 0-10 degrees.
The trochanteric prominence test (Craig's test) is utilized to estimate the degree of anteversion clinically. The examiner palpates the greater trochanter while internally and externally rotating the hip. The point at which the trochanter is most prominent laterally corresponds to the point where the femoral neck is parallel to the coronal plane. The angle of the tibia relative to the vertical axis at this point provides a reliable estimate of the anteversion angle.
For complex neuromuscular cases, particularly Cerebral Palsy, a formal 3D Instrumented Gait Analysis is indispensable. This provides dynamic, objective data regarding transverse plane kinematics, distinguishing true osseous anteversion from dynamic internal rotation driven by spasticity, and identifying concomitant multi-level deformities that may require simultaneous correction (Single-Event Multilevel Surgery - SEMLS).
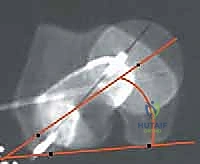
Radiographic Evaluation and Templating
Standard preoperative imaging includes an anteroposterior (AP) radiograph of the pelvis and bilateral frog-leg lateral radiographs of the hips. These images assess joint congruity, the neck-shaft angle (to rule out concomitant coxa valga or vara), and the presence of dysplasia. While CT scans can precisely quantify femoral version, they are associated with significant radiation exposure and are generally reserved for highly complex or revision cases where clinical estimation is insufficient.
Templating is performed using the AP radiograph to select the appropriate 90-degree AO blade plate. These plates are available in various sizes (infant, toddler, child, adolescent) and blade lengths. The template is overlaid on the proximal femur to determine the ideal insertion point for the seating chisel, ensuring the blade will reside centrally within the femoral neck and head without breaching the cortex or the physis (in skeletally immature patients).
Patient Positioning and Fluoroscopy Setup
The choice of patient positioning—supine versus prone—is dictated by the need for concomitant procedures and the surgeon's preference for intraoperative rotational assessment.
The Supine Position:
This is the preferred position for the majority of modern reconstructive procedures, particularly when multi-level surgery is anticipated. The patient is placed supine on a radiolucent Jackson table or a standard operating table with a radiolucent extension.
Crucially, both lower extremities must be prepped and draped free. This allows the surgeon to perform the "intraoperative log-roll test," comparing the torsional profile of the operative leg to the contralateral limb in real-time. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, perpendicular to the patient. This setup allows for rapid acquisition of true AP and frog-leg lateral images without compromising the sterile field or requiring awkward maneuvering of the operative limb.
The Prone Position:
While less commonly utilized today for multi-level surgery, the prone position offers distinct advantages for isolated derotational osteotomies.


In the prone position, the intraoperative assessment of the rotational profile mirrors the preoperative clinical examination perfectly. The surgeon can directly visualize the angle of the tibia relative to the vertical axis. Furthermore, gravity assists in retracting the vastus lateralis anteriorly, providing exceptional exposure of the lateral femoral shaft. However, this position precludes any simultaneous anterior procedures, such as psoas lengthening or pelvic osteotomies.
Step-by-Step Surgical Approach and Fixation Technique
The operative execution demands a systematic, unhurried progression through exposure, hardware preparation, osteotomy, and definitive fixation. Strict adherence to AO principles of rigid internal fixation is required to ensure rapid union and prevent hardware failure.
1. Incision, Fascial Release, and Muscular Elevation
Following precise localization of the greater trochanter via palpation and fluoroscopy, a longitudinal skin incision is made along the lateral aspect of the proximal thigh, centered over the femoral diaphysis. The length of the incision is dictated by the size of the selected blade plate, typically ranging from 8 to 15 cm.
The subcutaneous tissue is sharply divided to expose the glistening white fibers of the fascia lata. The fascia lata is incised longitudinally in line with the skin incision. Retraction of the fascial edges reveals the vastus lateralis muscle belly.
We proceed with the L-shaped release of the vastus lateralis. The transverse limb of the "L" is made just distal to the vastus ridge, leaving a sufficient tendinous cuff attached to the greater trochanter for later repair.

The longitudinal limb of the "L" is developed by elevating the vastus lateralis off the lateral intermuscular septum and the linea aspera posteriorly. This elevation must be performed meticulously, utilizing a periosteal elevator and electrocautery.

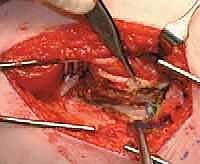
As the muscle is reflected anteriorly, the perforating branches of the profunda femoris artery will be encountered. These must be isolated and coagulated or ligated to maintain a bloodless field. Once elevated, Hohmann retractors are placed anteriorly and posteriorly over the femoral shaft to maintain exposure.
2. Guide Wire Placement and Orientation
The accuracy of the blade plate insertion dictates the final alignment of the proximal femur. We begin by inserting a 2.0 mm or 2.5 mm threaded guide wire into the lateral cortex, aiming into the center of the femoral neck and head.

The starting point is typically 1.5 to 2.0 cm distal to the vastus ridge, in the anterior half of the lateral cortex, to account for the anteversion of the neck. The trajectory of this wire is confirmed in both the AP and frog-leg lateral planes using fluoroscopy.

To control the rotational correction, a second K-wire (the anteversion wire) is placed anteriorly, parallel to the floor (assuming the patella is pointing straight up). A third wire can be placed distally in the femoral condyles to serve as a rotational reference.
3. Seating Chisel Insertion
Once the guide wire is perfectly positioned, the lateral cortex is opened utilizing a router or a drill to prevent cortical shattering during chisel insertion. The seating chisel, equipped with the appropriate guide, is then advanced over or parallel to the guide wire.


The chisel must be advanced with controlled mallet strikes, ensuring that the trajectory strictly follows the pre-determined path into the femoral neck. Fluoroscopic verification is mandatory after every few millimeters of advancement to ensure
Clinical & Radiographic Imaging Archive