Pelvic Ring Fractures: Comprehensive Evaluation, Biomechanics, and Surgical Management

Key Takeaway
High-energy pelvic ring fractures present complex challenges requiring rapid hemodynamic stabilization and precise surgical reconstruction. Initial management prioritizes hemorrhage control using pelvic binders and retroperitoneal packing. Definitive treatment relies on understanding pelvic biomechanics, accurate Tile and Young-Burgess classification, and meticulous surgical approaches to restore the anterior and posterior pelvic ring, minimizing mortality and optimizing long-term functional outcomes.
Introduction to Pelvic Ring Fractures
High-energy pelvic ring fractures represent some of the most formidable challenges in orthopedic trauma. Resulting most commonly from motor vehicle collisions, motorcycle accidents, falls from significant heights, automobile-pedestrian encounters, and industrial crush injuries, these fractures are frequently associated with life-threatening polytrauma.
The potential complications of high-energy pelvic fractures extend far beyond the osseous disruption. They frequently include catastrophic injuries to the major vessels and nerves of the pelvis, as well as damage to major viscera such as the intestines, bladder, and urethra. Degloving injuries to the surrounding soft tissues (Morel-Lavallée lesions), whether open or closed, frequently accompany these fractures and severely complicate surgical timing and approach.
Reported mortality from severe pelvic fractures ranges from 10% to as high as 50% in historical series of open pelvic fractures. Risk factors for increased mortality include advanced patient age, a high Injury Severity Score (ISS), associated traumatic brain injury (TBI) or visceral injury, massive blood loss, hypotension on presentation, coagulopathy, and the presence of unstable or open pelvic fracture patterns. Early mortality is almost exclusively driven by exsanguinating hemorrhage or severe closed head injury, whereas late mortality typically results from sepsis or multiple organ dysfunction syndrome (MODS).
Clinical Pearl: The initial assessment of a pelvic fracture must occur simultaneously with advanced trauma life support (ATLS) resuscitation. The pelvis can hide up to 3-4 liters of blood; therefore, unexplained hypotension in a blunt trauma patient should be considered a pelvic hemorrhage until proven otherwise.
Pelvic Anatomy and Biomechanics
A profound understanding of pelvic anatomy and biomechanics is the cornerstone of both conservative and operative management. The work of Bucholz, Pennal et al., Young and Burgess, and Tile has extensively elucidated the pathomechanics of pelvic ring disruptions.
Osteology and the "Suspension Bridge" Concept
The pelvis is a ring structure composed anteriorly of the pubic and ischial rami connected at the symphysis pubis, where a fibrocartilaginous disc separates the two pubic bodies. Posteriorly, the sacrum and the two innominate bones articulate at the sacroiliac (SI) joints.
Tile famously compared the relationship of the posterior pelvic ligamentous and bony structures to a suspension bridge, with the sacrum suspended between the two posterior superior iliac spines (PSIS) by a robust network of ligaments. Because the SI joint has minimal inherent bony stability, it relies entirely on this ligamentous complex.
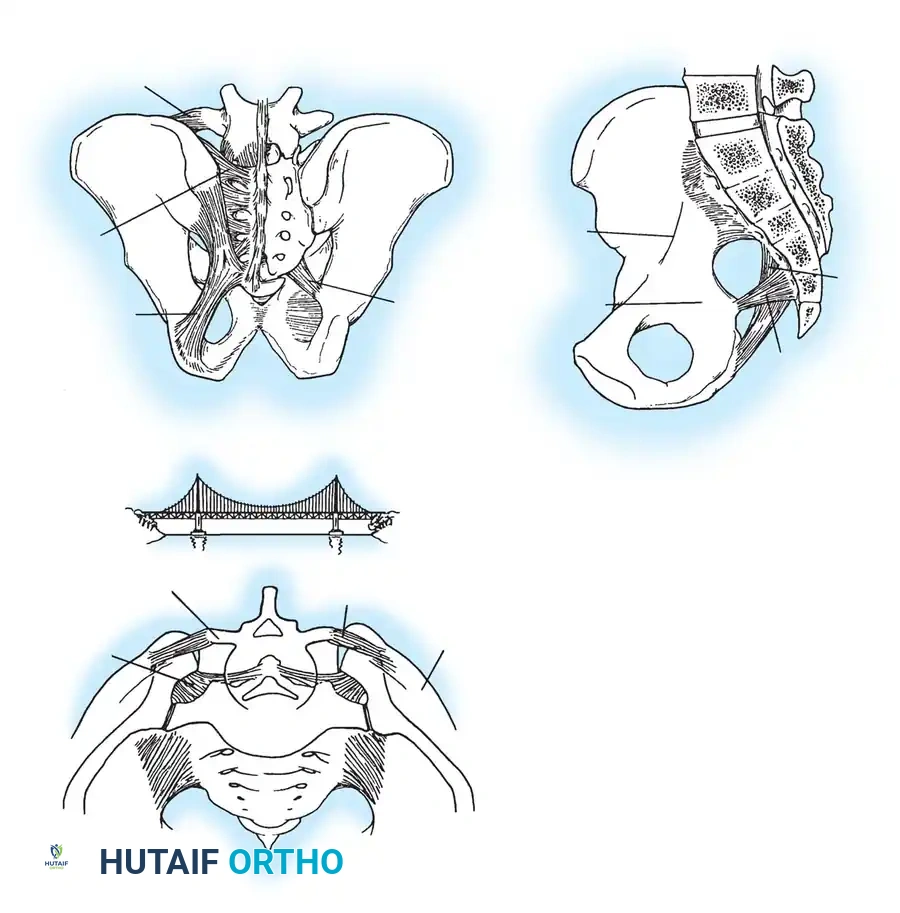
Ligamentous Restraints
Pelvic stability is dictated by ligamentous structures acting in various orthogonal planes:
* Anterior Restraints: The symphyseal ligaments resist external rotation.
* Pelvic Floor Restraints: The sacrospinous ligament resists external rotation, while the sacrotuberous ligament resists shearing and rotation in the sagittal plane.
* Posterior Restraints: The anterior SI ligaments resist external rotation. The massive interosseous SI ligaments, posterior SI ligaments, and iliolumbar ligaments are the primary restraints to vertical displacement.
Surgical Warning: A rotationally unstable hemipelvis may remain vertically stable if the posterior tension band (interosseous and posterior SI ligaments) remains intact. Recognizing this distinction is critical, as it dictates whether posterior vertical fixation is required.
Initial Evaluation and Resuscitation
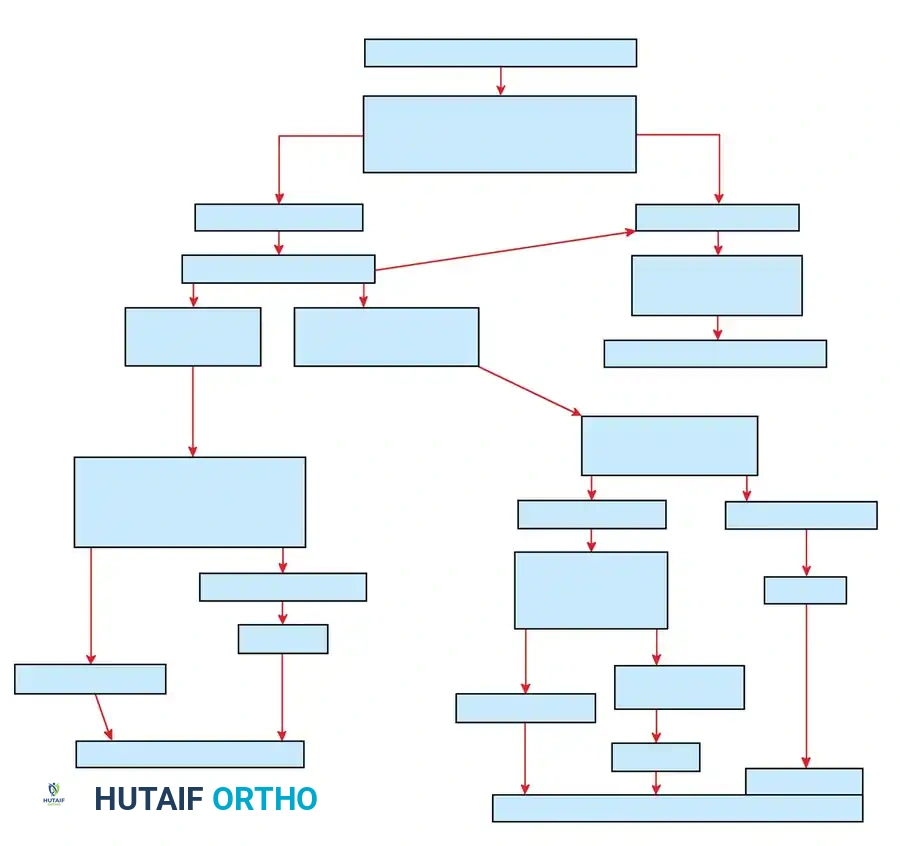
The initial management of a patient with a suspected pelvic ring fracture follows a strict algorithmic approach based on hemodynamic stability.
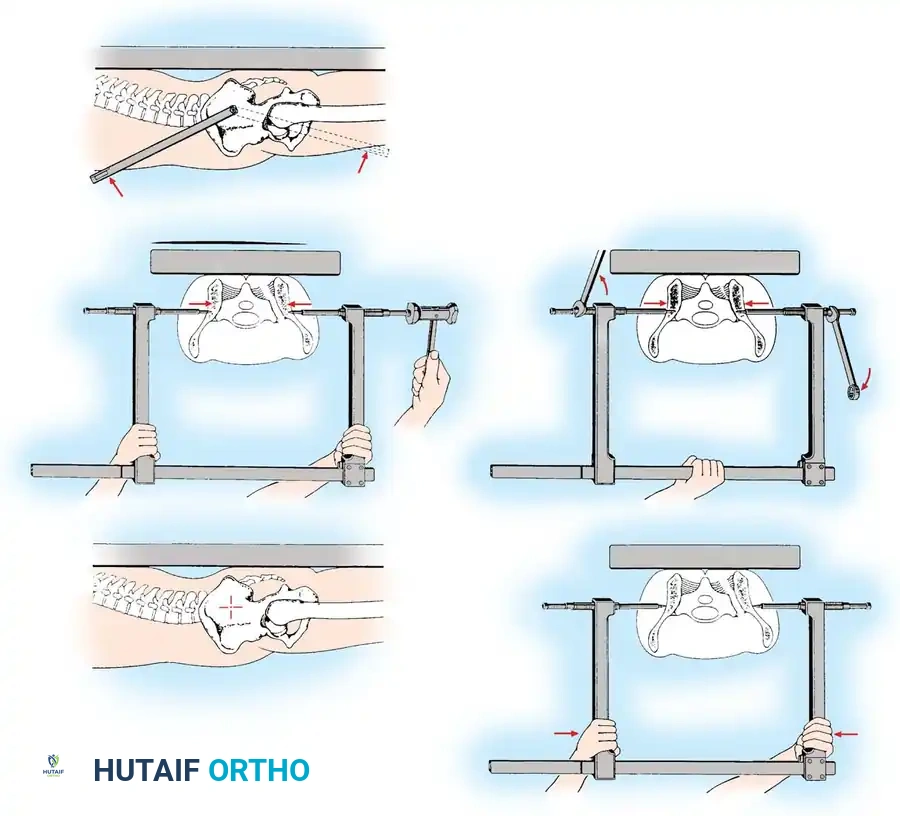
Hemorrhage Control and Pelvic Binding
If the patient is hemodynamically unstable, immediate circumferential pelvic wrapping is indicated. A pelvic binder or tightly wrapped sheet must be centered over the greater trochanters—not the iliac crests—to effectively close the pelvic volume and provide a tamponade effect.


The Hemodynamically Unstable Patient
If the patient remains in extremis despite aggressive fluid and blood product resuscitation, the source of bleeding must be rapidly identified.
1. FAST Exam / DPL: To rule out massive intraperitoneal hemorrhage requiring emergent laparotomy.
2. Retroperitoneal Packing: If bleeding is extraperitoneal (pelvic source), preperitoneal pelvic packing combined with external fixation has shown highly favorable early results in controlling venous and cancellous bone bleeding.
3. Angiography: Indicated for arterial hemorrhage (most commonly the superior gluteal or internal pudendal arteries from the internal iliac plexus).


Management of Open Pelvic Fractures
Open pelvic fractures are devastating injuries with historical mortality rates approaching 50%. The breach of the retroperitoneal space eliminates the tamponade effect, leading to unchecked hemorrhage. Furthermore, sepsis caused by fecal or genitourinary contamination is a major driver of late mortality.
Faringer Zones and Fecal Diversion
Faringer et al. anatomically classified open pelvic wounds into three zones to guide the necessity of diverting colostomies:
* Zone I (Perineal/Gluteal): High risk of fecal contamination. Immediate diverting colostomy is strongly indicated.
* Zone II (Groin/Thigh): Selective diversion based on wound proximity to the anus and tissue viability.
* Zone III (Iliac/Flank): Diversion is rarely required.
Routine vaginal and rectal examinations are mandatory in all suspected pelvic fractures to rule out occult open fractures caused by penetrating bone spicules.
Classification Systems
Accurate classification dictates the surgical approach and prognosis. The two most widely utilized systems are the Tile classification (based on stability) and the Young-Burgess classification (based on the mechanism of injury).
Tile Classification (Stability-Based)
- Type A (Stable): Posterior arch intact. Includes avulsion fractures (A1), stable minimally displaced ring fractures (A2), and transverse sacrococcygeal fractures (A3).
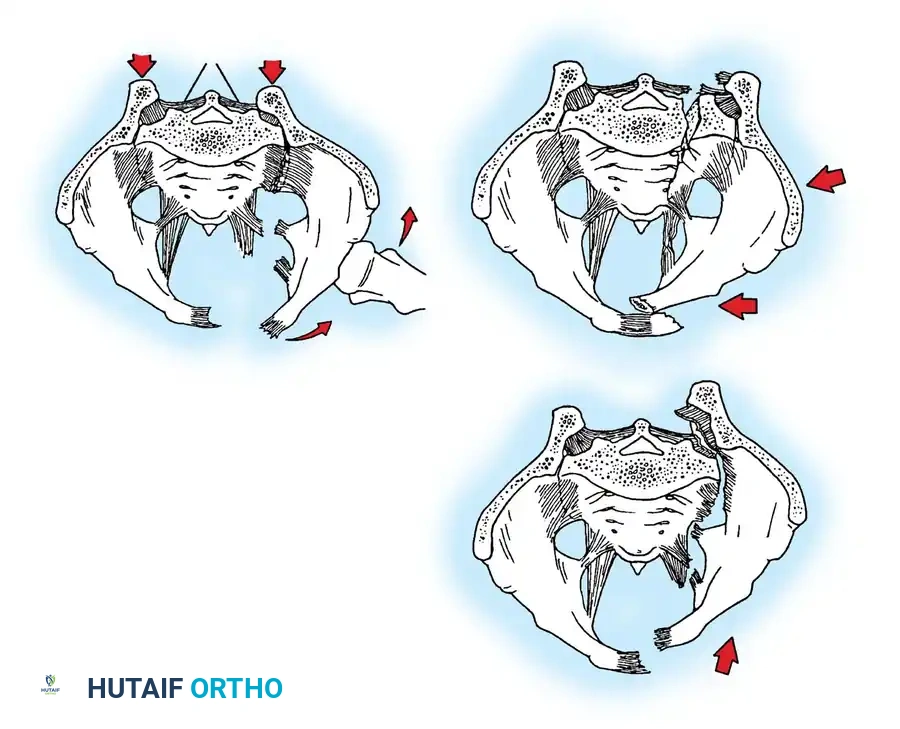
- Type B (Rotationally Unstable, Vertically Stable): Incomplete disruption of the posterior arch.
- B1: "Open book" (external rotation) injury.
- B2: Lateral compression (internal rotation) injury.
- B3: Bilateral Type B injuries.
- Type C (Rotationally and Vertically Unstable): Complete disruption of the posterior arch.
- C1: Unilateral complete disruption.
- C2: Bilateral, with one side Type B and one side Type C.
- C3: Bilateral complete disruptions.
Young and Burgess Classification (Mechanistic)
- Anterior-Posterior Compression (APC):
- APC I: Symphysis widening < 2.5 cm. Stable.
- APC II: Symphysis widening > 2.5 cm. Anterior SI ligaments torn, posterior SI ligaments intact. Rotationally unstable, vertically stable.
- APC III: Complete anterior and posterior disruption. Rotationally and vertically unstable.
- Lateral Compression (LC):
- LC I: Sacral compression fracture with ipsilateral rami fractures. Stable.
- LC II: Crescent fracture of the ilium. Rotationally unstable.
- LC III: "Windswept" pelvis. Ipsilateral LC and contralateral APC.
- Vertical Shear (VS): Complete vertical displacement of the hemipelvis.

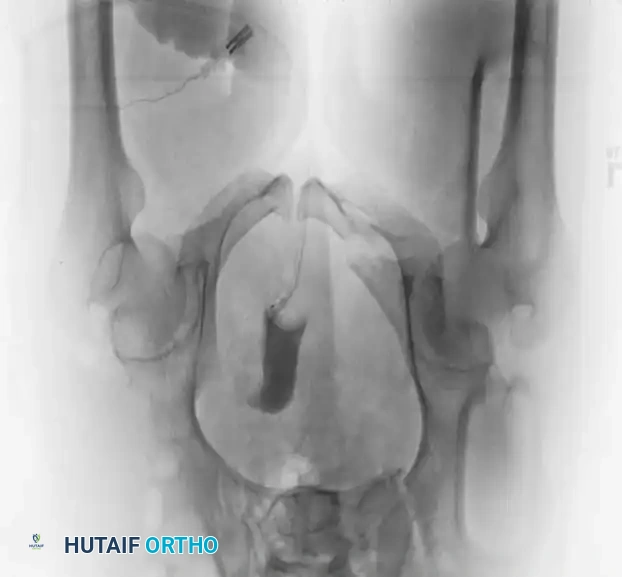


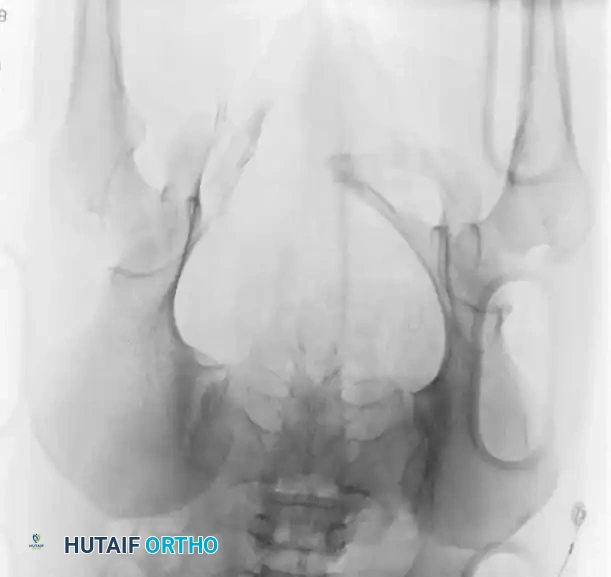
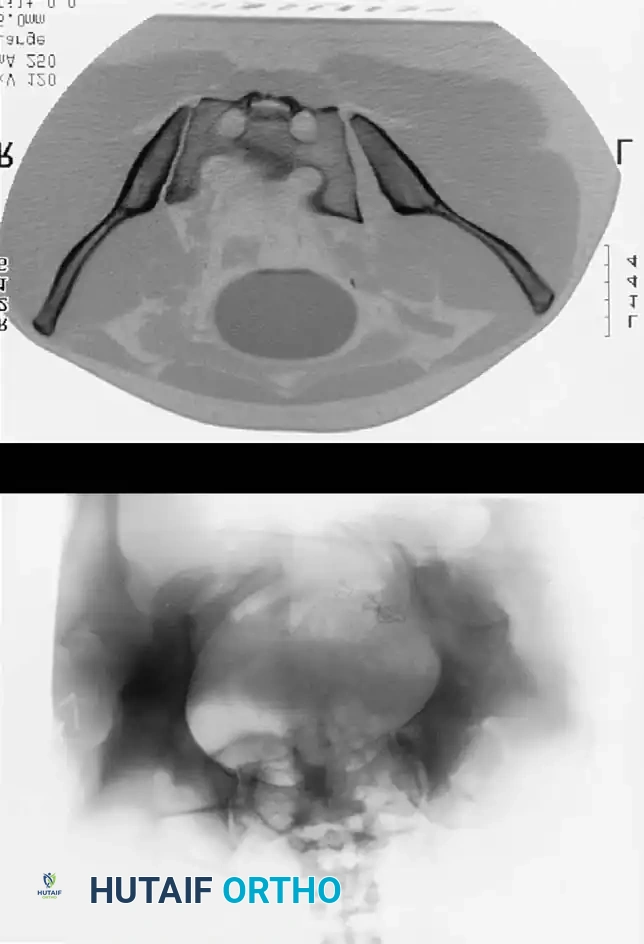
Radiographic Evaluation
Standard evaluation begins with an Anteroposterior (AP) pelvis radiograph. However, definitive surgical planning requires specialized views and advanced imaging.
- Inlet View: Directed 45 degrees caudad. Best evaluates anterior-posterior translation, internal/external rotation, and sacral impaction.
- Outlet View: Directed 45 degrees cephalad. Best evaluates vertical translation and sacral foraminal anatomy.
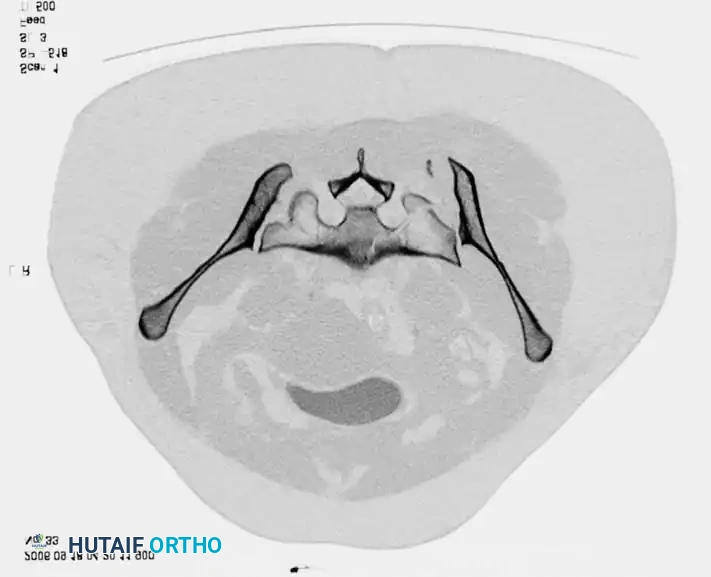
- CT Scan: The gold standard for evaluating posterior ring injuries, sacral dysmorphism, and preoperative planning for percutaneous fixation.



Surgical Indications and Timing
Operative intervention is indicated for:
1. Symphyseal diastasis > 2.5 cm (APC II/III).
2. Vertical instability (Tile C / VS).
3. Severe rotational deformity causing leg length discrepancy or internal organ impingement (severe LC injuries).
4. Open fractures requiring debridement and stabilization.
Timing: Damage control orthopedics (external fixation, pelvic packing) is performed immediately. Definitive Open Reduction and Internal Fixation (ORIF) is typically delayed 5-10 days to allow for hemodynamic optimization and resolution of the initial inflammatory hit, provided the patient is physiologically stable.




Surgical Approaches to the Pelvis
Anterior Approaches
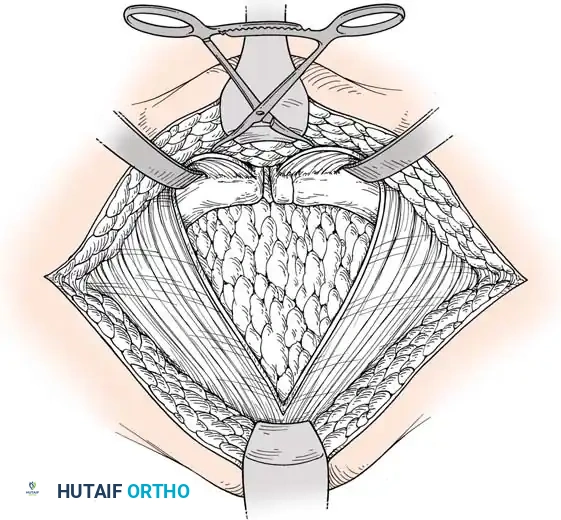
- Pfannenstiel Approach: The workhorse for symphyseal plating. A transverse incision is made 2 fingerbreadths proximal to the symphysis. The rectus abdominis is split along the linea alba to expose the retropubic space (Space of Retzius).
- Ilioinguinal Approach: Used for anterior ring and anterior SI joint disruptions. It provides access to the entire anterior column from the SI joint to the symphysis.
- Modified Stoppa Approach: An intrapelvic approach providing excellent visualization of the quadrilateral plate and posterior column, often used in combined pelvic/acetabular trauma.
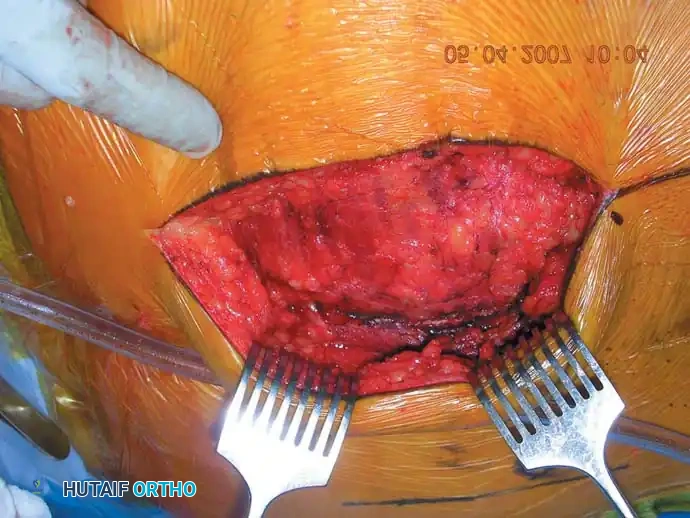
Posterior Approaches
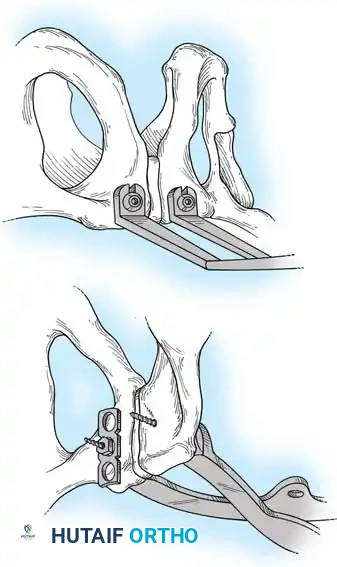
- Posterior Approach to the SI Joint: Utilized for direct reduction and plating of crescent fractures or severe SI joint fracture-dislocations. Involves a longitudinal or gently curved incision lateral to the PSIS, elevating the gluteus maximus to expose the ilium and SI joint.



Step-by-Step Surgical Techniques
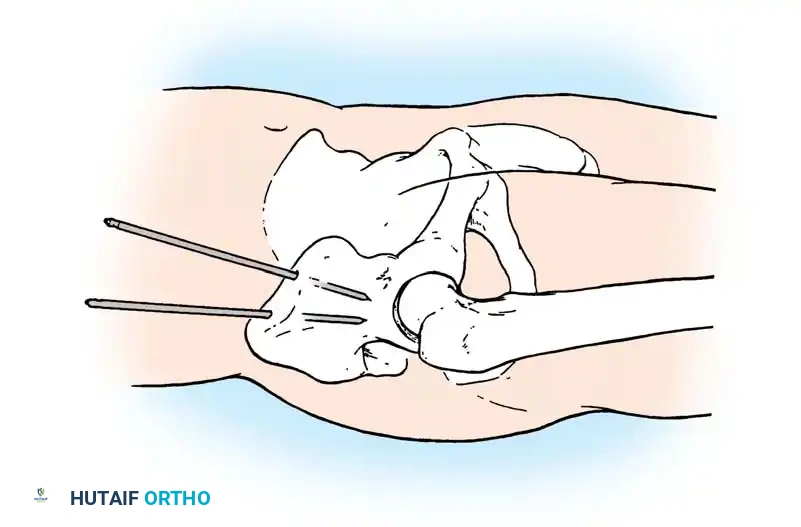
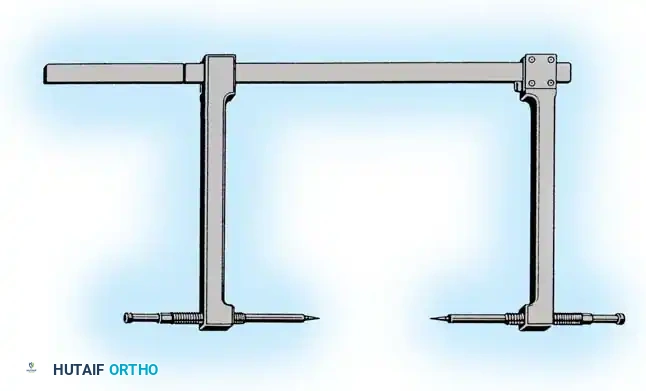
1. External Fixation
External fixation is primarily a damage-control tool but can be definitive for certain rotationally unstable (APC II) patterns.
* Iliac Crest Pins: Placed between the inner and outer tables of the iliac crest. Prone to loosening and pin-tract infections.
* Supra-acetabular Pins: Placed from the AIIS directed toward the PSIS. Biomechanically superior and allows for better patient mobilization.


2. Symphyseal Plating (Anterior Ring)
- Positioning: Supine on a radiolucent table.
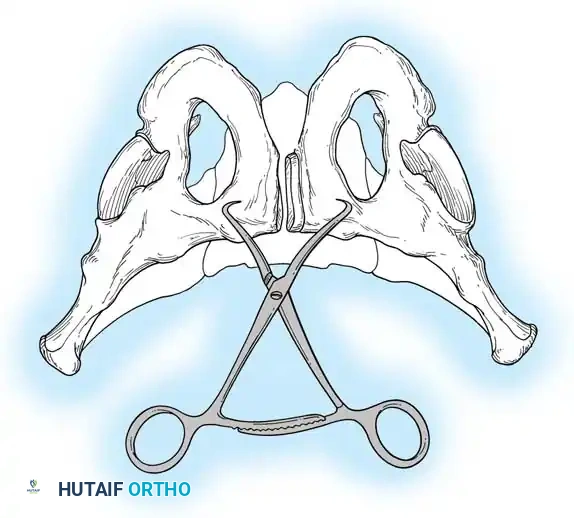
- Reduction: A Weber clamp or specialized pelvic reduction forceps are placed on the pubic tubercles or via drill holes in the superior rami to reduce the diastasis.
- Fixation: A multi-hole, stout pelvic reconstruction plate (typically 4 to 6 holes) is placed superiorly. Screws must be directed carefully to avoid joint penetration or bladder injury.

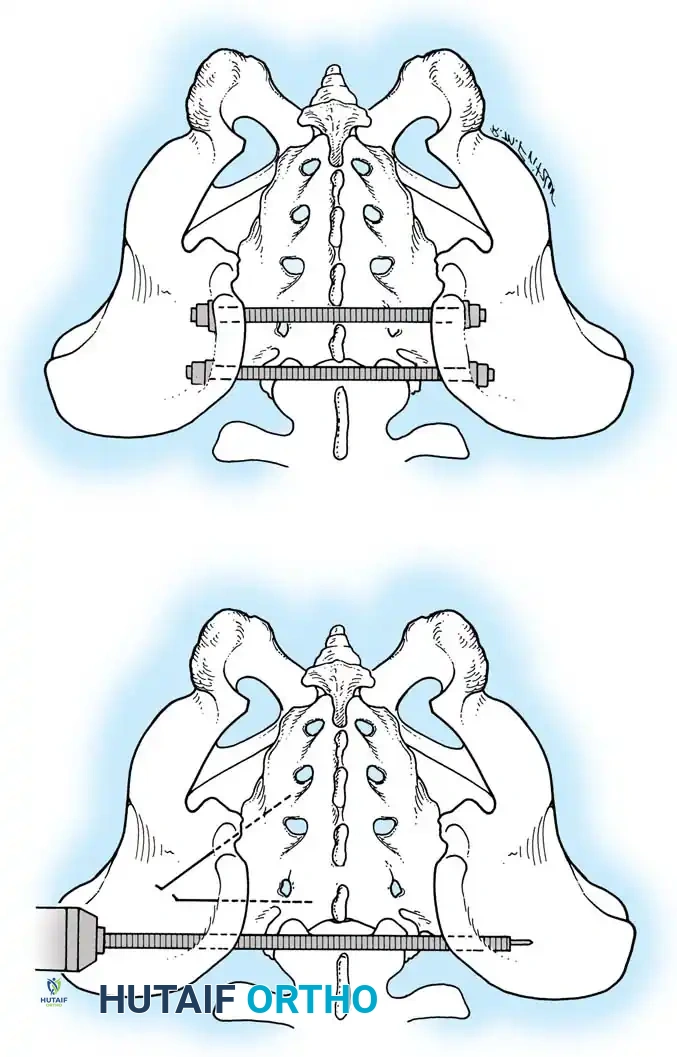
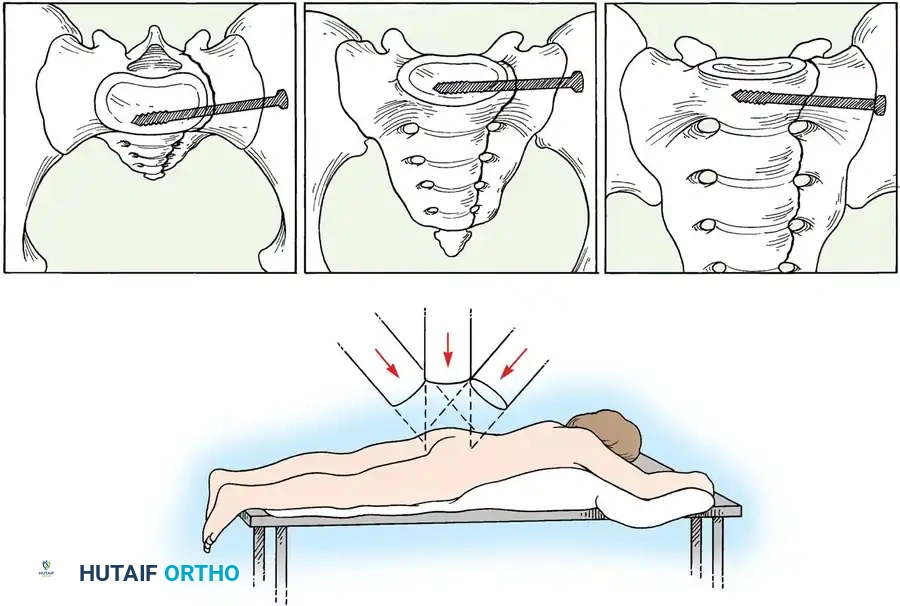
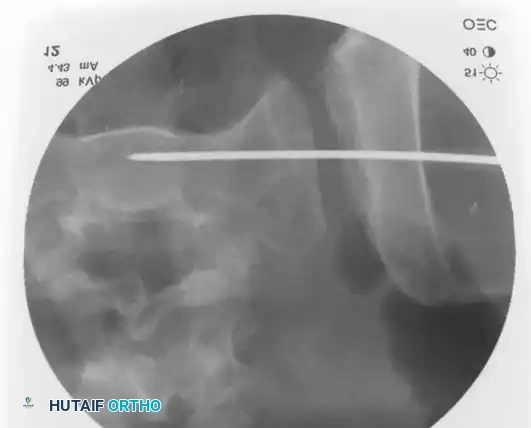
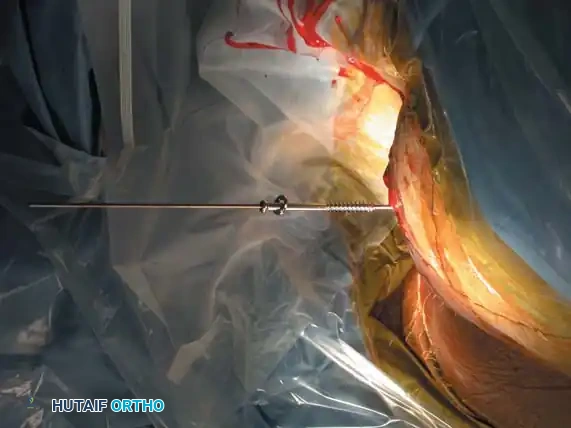
3. Percutaneous Sacroiliac (SI) Screws (Posterior Ring)
The gold standard for posterior ring fixation in appropriately selected patients.
* Indications: Sacral fractures, SI joint disruptions, crescent fractures.
* Technique: Performed under strict fluoroscopic guidance (Inlet, Outlet, and Lateral sacral views).
* Trajectory: The guide wire is advanced from the lateral ilium, across the SI joint, into the S1 (or S2) vertebral body.
* Safety Corridors: The surgeon must possess an intimate understanding of sacral dysmorphism. The "safe zone" is bounded by the sacral neural foramina inferiorly, the spinal canal posteriorly, and the sacral ala anteriorly.
Pitfall: Failure to recognize a dysmorphic sacrum (characterized by upper sacral segment elevation, non-recessed alae, and oblique neural foramina) can lead to catastrophic L5 nerve root injury or vascular penetration during SI screw placement.
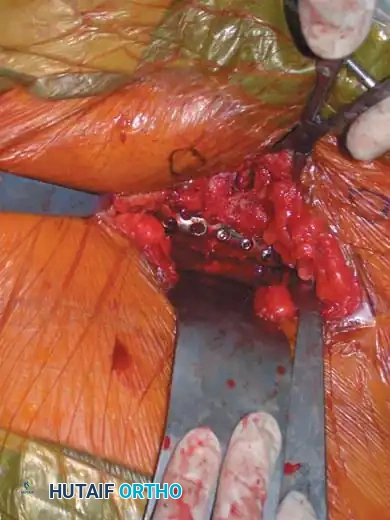
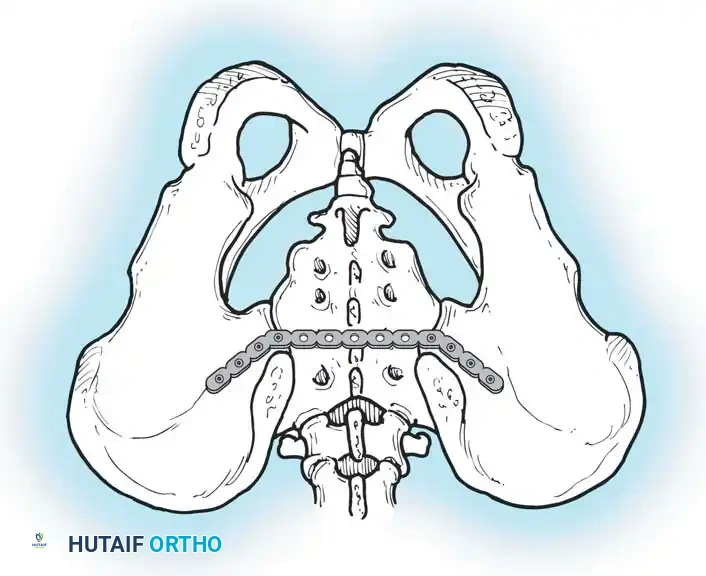
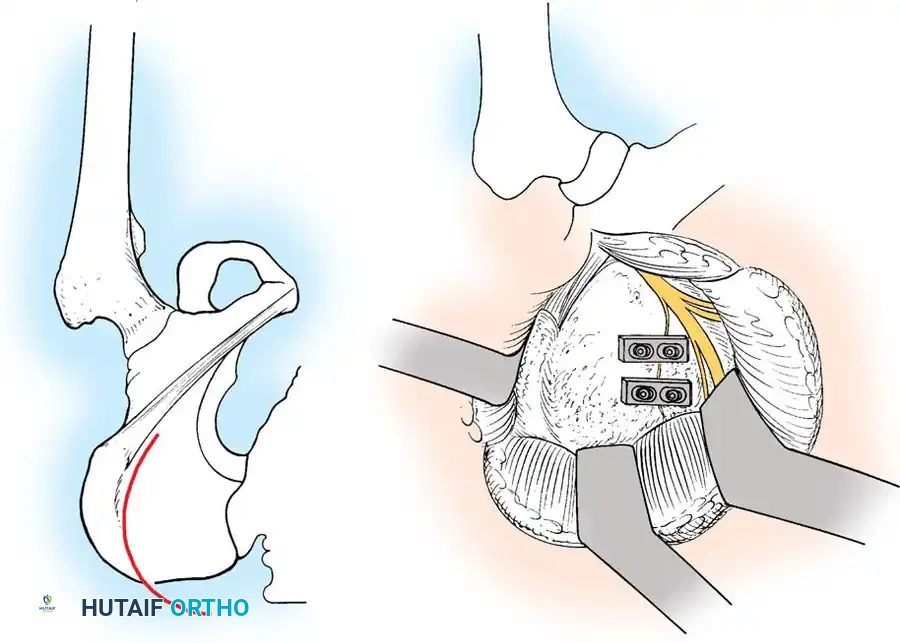
4. Posterior Tension Band Plating
For comminuted sacral fractures or when percutaneous corridors are unsafe, open reduction and posterior tension band plating (or lumbopelvic fixation) may be required. This involves placing plates across the posterior ilium to the sacrum, effectively recreating the posterior ligamentous tension band.

Postoperative Protocol and Complications
Rehabilitation
- Weight-Bearing: Patients with unstable posterior ring injuries (Tile C) are typically restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) on the affected side for 8 to 12 weeks.
- DVT Prophylaxis: Pelvic trauma carries an exceptionally high risk of venous thromboembolism. Chemical prophylaxis (LMWH) should be initiated as soon as bleeding risk permits and continued for at least 4 weeks.
Complications
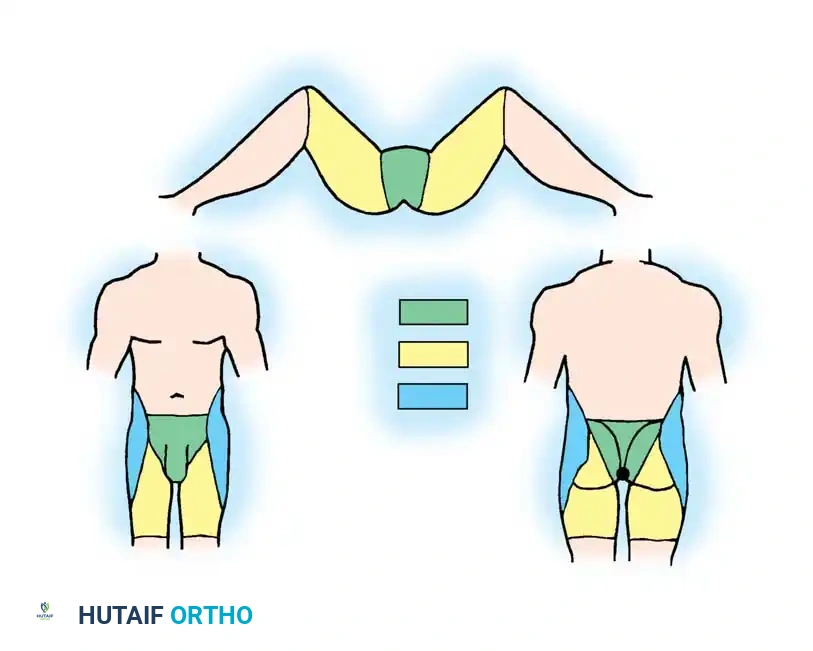
- Neurologic Injury: The L5 and S1 nerve roots are most commonly injured, either from the initial trauma (vertical shear) or iatrogenically during posterior fixation.
- Infection: High risk in open fractures and posterior surgical approaches due to poor soft-tissue envelopes and proximity to the perineum.
- Urologic Dysfunction: Urethral strictures, bladder dysfunction, and sexual dysfunction (erectile dysfunction in males, dyspareunia in females) are common long-term sequelae of anterior ring disruptions.
- Nonunion/Malunion: Can lead to chronic pelvic pain, sitting imbalance, and leg length discrepancies requiring complex reconstructive osteotomies.
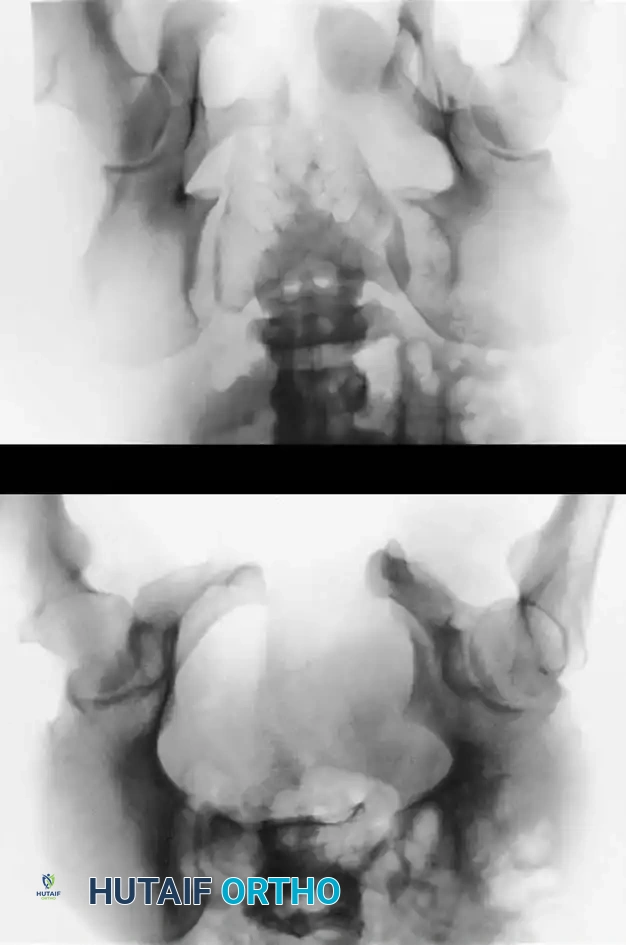
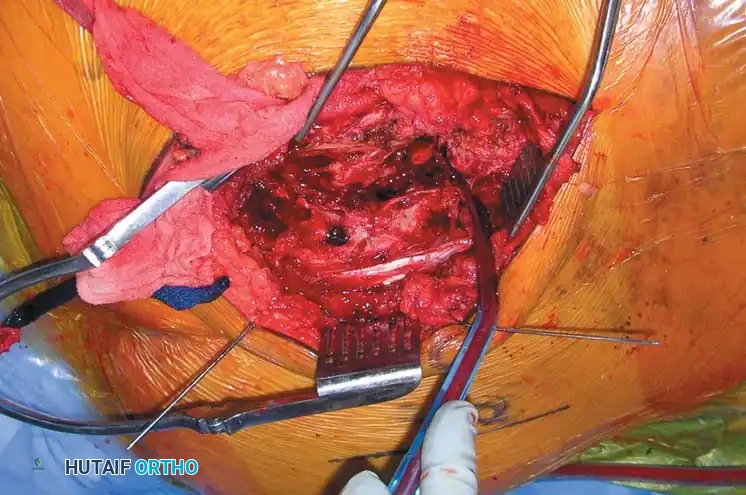
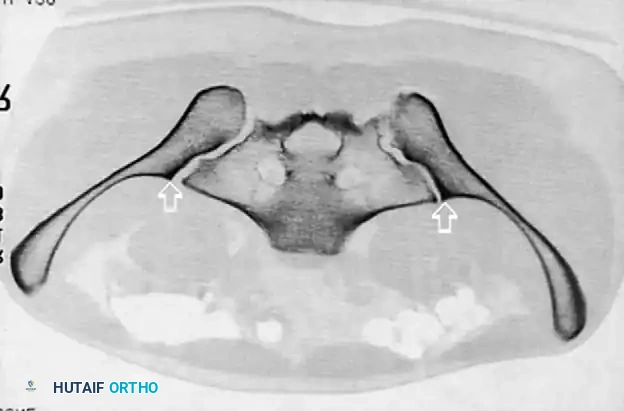
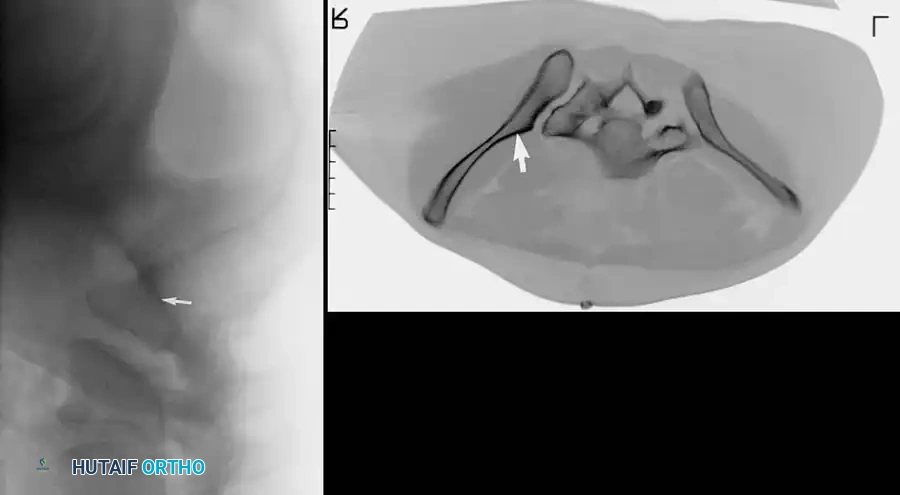
Radiographic and Intraoperative Gallery
The following gallery demonstrates the progression of complex pelvic ring reconstructions, highlighting advanced imaging, intraoperative fluoroscopy, and definitive fixation constructs.
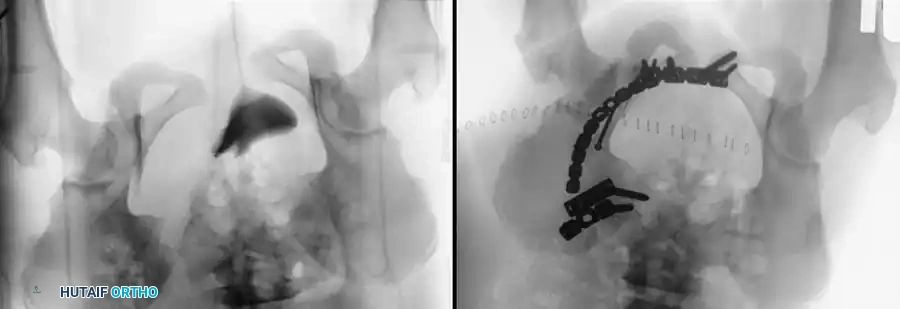
Advanced Imaging and Preoperative Planning

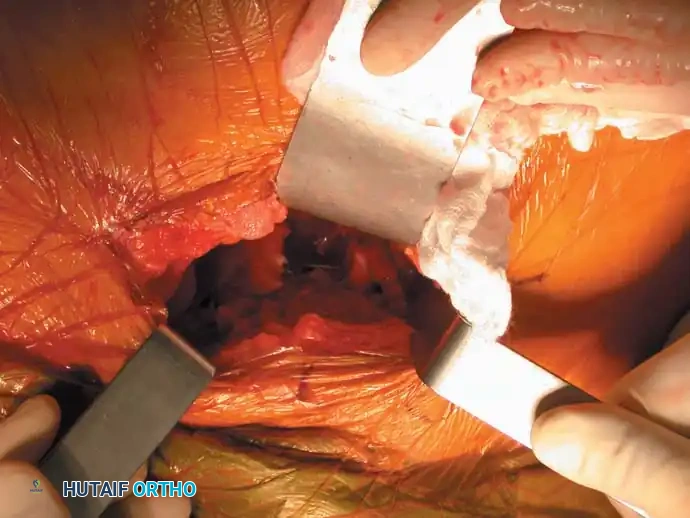
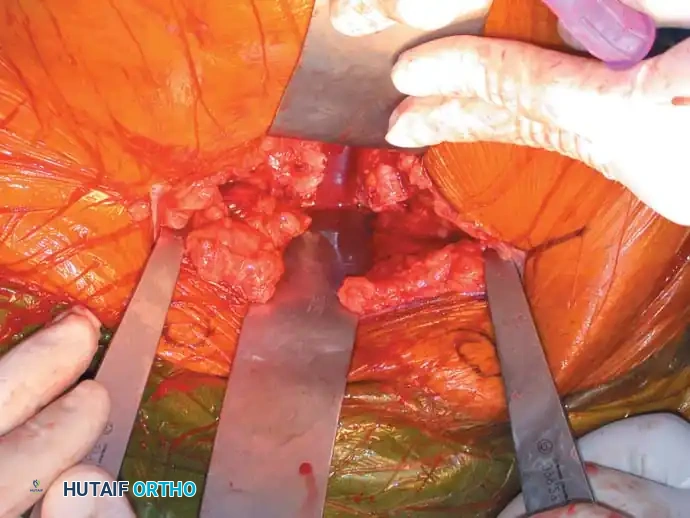
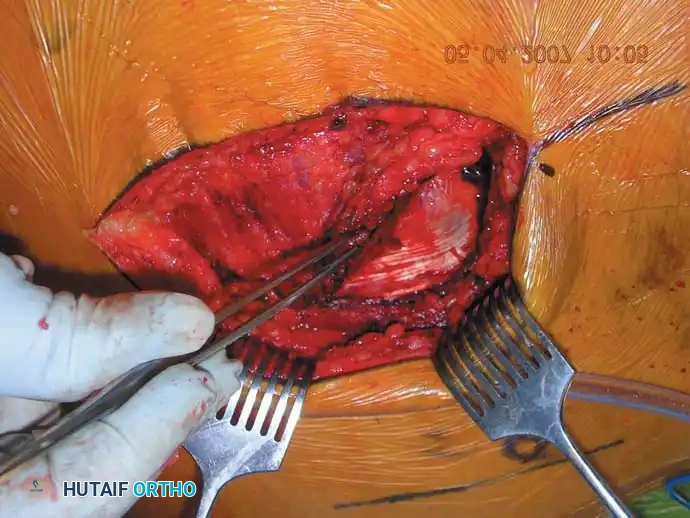
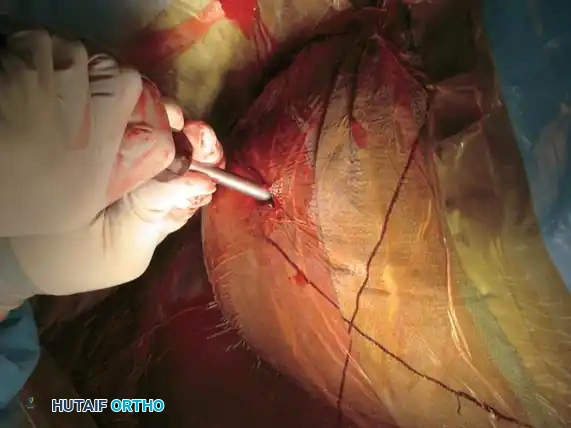
Intraoperative Fluoroscopy and Reduction Techniques


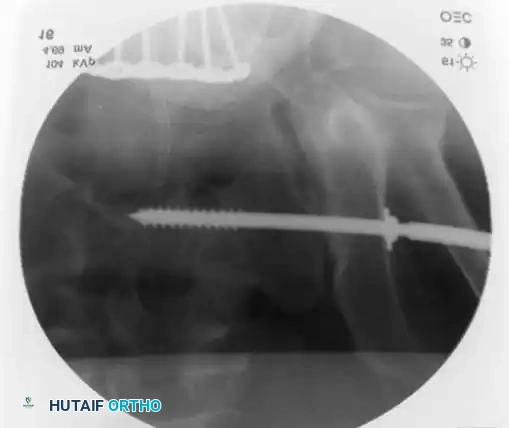
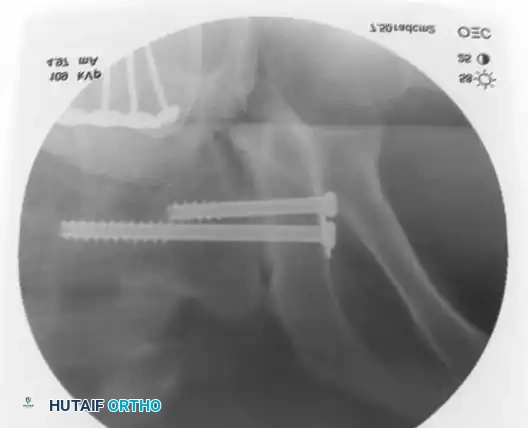
Definitive Fixation Constructs
Complex Reconstructions and Outcomes
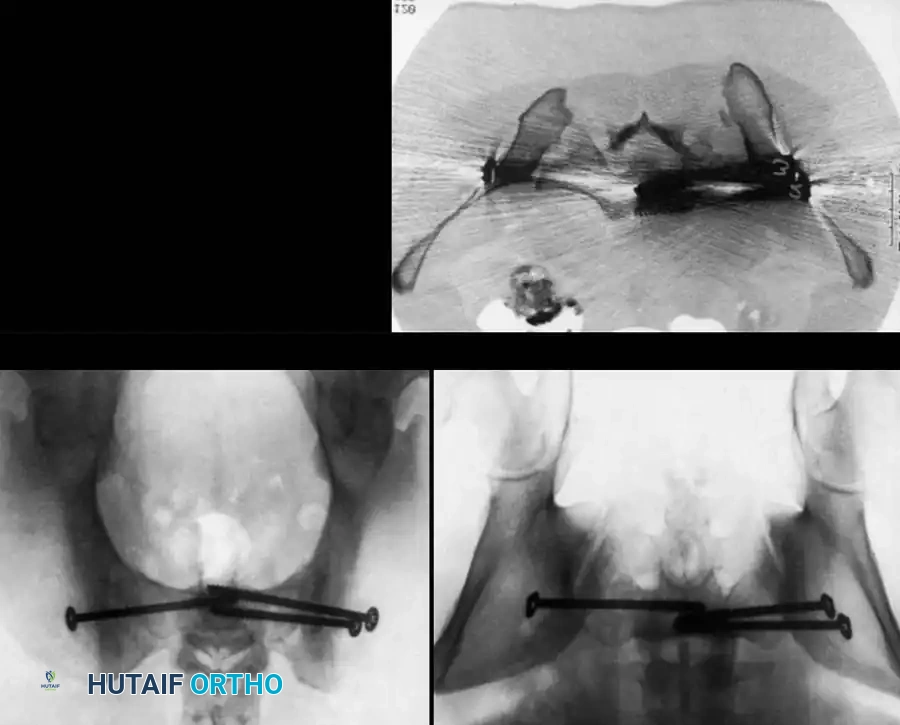



Postoperative Verification


📚 Medical References
- pelvic ring fractures with use of circumferential compression, J Bone Joint Surg 84A:43, 2002.
- Bottlang M, Simpson T, Sigg J, et al: Noninvasive reduction of open-book pelvic fractures by circumferential compression, J Orthop Trauma 16:367, 2002.
- Brenneman FD, Katyal D, Boulanger BR, et al: Long-term outcomes in open pelvic fractures, J Trauma 42:773, 1997.
- Browner BD, Cole JD, Graham JM, et al: Delayed posterior internal fi xation of unstable pelvic fractures, J Trauma 27:998, 1987.
- Bucholz RW: The pathological anatomy of Malgaigne fracturedislocations of the pelvis, J Bone Joint Surg 63A:400, 1981.
- Bucholz RW: Pathomechanics of pelvic ring disruptions, Adv Orthop Surg 10:167, 1987.
- Bucholz RW, Peters P: Assessment of pelvic stability, Instr Course Lect 37:119, 1988.
- Buckle R, Browner BD, Morandi M: Emergency reduction for pelvic ring disruptions and control of associated hemorrhage using the pelvic stabilizer, Tech Orthop 9:258, 1994.
- Buckley SL, Burkus JK: Computerized axial tomography of pelvic ring fractures, J Trauma 27:496, 1987.
- Buerger PM, Peoples JB, Lemmon GW, et al: Risk of pulmonary embolism in patients with pelvic fractures, Am Surg 59:505, 1993.
- Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: effective classifi cation system and treatment protocols, J Trauma 30:848, 1990.
- Carrillo EH, Wohltmann CD, Spain DA, et al: Common and external iliac artery injuries associated with pelvic fractures, J Orthop Trauma 13:351, 1999.
- Cass AS, Behrens F, Comfort T, et al: Bladder problems in pelvic injuries with external fi xator and direct urethral drainage, J Trauma 23:50, 1983.
- Cecil ML, Rollins JR, Ebraheim NA, et al: Projection of the S2 pedicle onto the posterolateral surface of the ilium: a technique for lag screw fi xation of sacral fractures or sacroiliac joint dislocations, Spine 21:875, 1996.
- Cole JD, Blum DA, Ansel LJ: Outcome after fi xation of unstable posterior pelvic ring injuries, Clin Orthop Relat Res 329:160, 1996.
- Collinge C, Tornetta P:
You Might Also Like

