Osteochondrosis and Epiphysitis: Comprehensive Surgical Management

Key Takeaway
Osteochondrosis and epiphysitis encompass a spectrum of disorders affecting actively growing epiphyses, primarily driven by localized vascular insufficiency or repetitive microtrauma. While predominantly self-limiting and responsive to conservative measures, refractory cases or late-stage deformities—such as Freiberg infraction or unresolved Osgood-Schlatter ossicles—may necessitate precise surgical intervention. This guide details the biomechanics, diagnostic imaging, and operative techniques required for optimal patient outcomes.
Introduction to Osteochondrosis and Epiphysitis
The terms osteochondrosis and epiphysitis designate a heterogeneous group of disorders affecting actively growing epiphyses in the pediatric and adolescent populations. While the disorder may be localized to a single epiphysis, it occasionally involves multiple epiphyses simultaneously or successively. The precise etiology remains multifactorial; however, overwhelming evidence points toward a transient lack of vascularity. This localized ischemia may be the sequela of repetitive microtrauma, subacute infection, or underlying congenital malformations.
In certain anatomical locations, osteochondrosis presents as a highly distinctive clinical entity. However, osteochondrosis of intraarticular epiphyses can closely mimic other severe pediatric joint diseases, necessitating rigorous diagnostic evaluation. For instance, multiple epiphyseal dysplasia (MED) may present with radiographic features strikingly similar to Legg-Calvé-Perthes disease of the hip.
Clinical Pearl: To differentiate MED from Perthes disease, evaluate the bone age. In Perthes disease, the bone age typically lags 1 to 2 years behind the chronological age. In contrast, bone age usually remains normal in multiple epiphyseal dysplasia. Furthermore, radiographs of the ankle in MED often reveal characteristic lateral narrowing or wedging of the distal tibial epiphysis.
It is also critical to distinguish true avascular osteochondroses from traction apophysitides. Histological studies of excised specimens by Cohen, Wilkinson, Thompson, Dickinson, Rapp, and Lazerte have definitively concluded that Osgood-Schlatter disease is traumatic in origin—a traction apophysitis—and is not associated with a primary loss of vascularity. Therefore, it should not be strictly grouped with true osteochondroses.
This chapter focuses exclusively on epiphyseal disorders that, while often self-limiting, may progress to structural deformity requiring surgical intervention.
Traction Epiphysitis of the Fifth Metatarsal Base (Iselin Disease)
First described by Iselin in the German literature in 1912, Iselin disease is a traction epiphysitis of the base of the fifth metatarsal. It predominantly occurs in young adolescents corresponding to the appearance of the proximal epiphysis of the fifth metatarsal.
Biomechanics and Pathophysiology
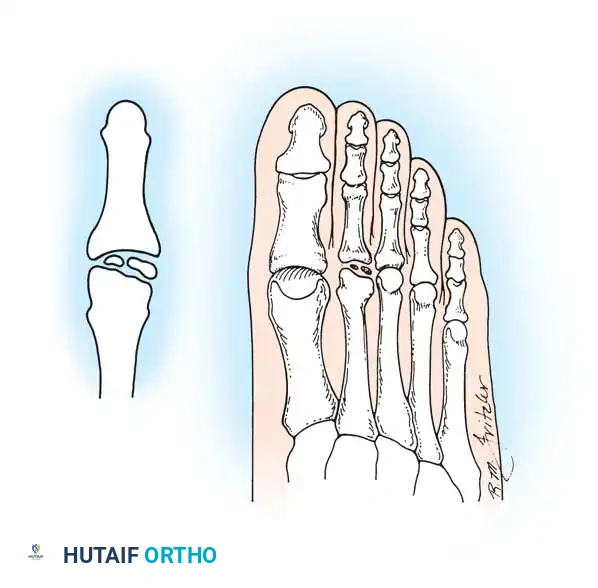
The secondary center of ossification is a small, shell-shaped fleck of bone oriented slightly obliquely with respect to the metatarsal shaft, located on the lateral plantar aspect of the tuberosity. Anatomical dissections confirm that this ossification center is embedded within the cartilaginous flare into which the peroneus brevis tendon inserts. Repetitive inversion stresses and the forceful pull of the peroneus brevis during athletic activities (running, jumping, cutting) lead to microavulsions and subsequent inflammation of the apophysis.
Ossification of the epiphysis on the fifth metatarsal shaft.
Clinical Presentation and Imaging
The epiphysis typically appears in girls at approximately 10 years of age and in boys at 12 years of age, with fusion occurring about 2 years later. Patients present with localized pain and tenderness over a prominent proximal fifth metatarsal, exacerbated by weight-bearing and sports. Physical examination reveals soft-tissue edema, local erythema, and pain elicited by resisted eversion or extreme plantar flexion and dorsiflexion.
Standard anteroposterior and lateral radiographs often fail to visualize the lesion adequately; an oblique view is mandatory. Hoerr et al. demonstrated that this epiphysis is visible on 99% of oblique radiographs in this age group. Imaging typically reveals enlargement, widening of the cartilaginous-osseous junction, and occasionally fragmentation of the epiphysis.


Enlargement and fragmentation of the epiphysis characteristic of Iselin disease.
Technetium-99m bone scanning will demonstrate intensely increased uptake over the epiphysis, confirming the inflammatory stress reaction.
Surgical Warning: Iselin disease must be carefully distinguished from a Jones fracture, a pseudo-Jones avulsion fracture, and the presence of an Os vesalianum (a sesamoid bone within the peroneus brevis tendon). Misdiagnosis can lead to unnecessary surgical intervention.
Os vesalianum, which must be distinguished from Iselin disease and acute fractures.
Management Protocol
Treatment is strictly non-operative, aimed at decreasing the stress reaction and acute inflammation caused by the overpull of the peroneus brevis tendon.
* Mild Symptoms: Activity modification, cessation of offending sports, cryotherapy, and nonsteroidal anti-inflammatory drugs (NSAIDs).
* Severe Symptoms: Short-leg walking cast or controlled ankle motion (CAM) boot immobilization for 3 to 6 weeks.
* Surgical Intervention: Internal fixation of the epiphysis is not indicated. While nonunion of the fifth metatarsal has been reported in adults as a rare sequela of failed epiphyseal fusion, acute surgical management of Iselin disease is contraindicated.
Osteochondrosis of the Metatarsal Head (Freiberg Infraction)
Freiberg infraction is a painful osteochondrosis most commonly affecting the head of the second metatarsal, though it frequently involves the third, and occasionally the fourth and fifth metatarsals. The condition is driven by repetitive microtrauma to the metatarsal head in the setting of a vulnerable vascular watershed zone, leading to subchondral bone collapse and secondary osteoarthritis.
Imaging Evaluation
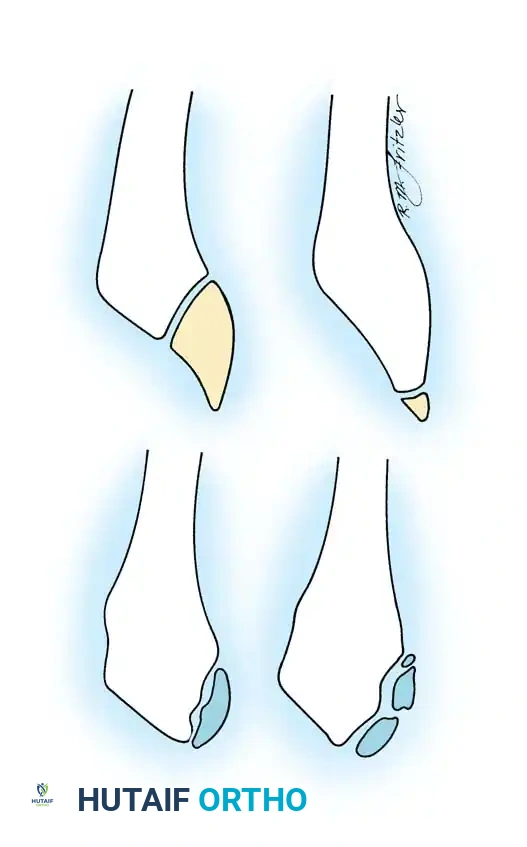
Early radiographic signs include joint space widening and subtle sclerosis of the metatarsal head. As the disease progresses, the subchondral bone collapses, leading to flattening of the articular surface, fragmentation, and the formation of loose bodies.


Condensation and sclerosis in the third metatarsal compared with the second and fourth metatarsals, indicating early acute Freiberg disease. Bone scan shows increased uptake in the metatarsal head.
Advanced stages are characterized by severe joint destruction, osteophyte formation, and intra-articular loose bodies that mechanically block joint motion.
Freiberg infraction of the second metatarsal with distinct intra-articular loose bodies.
Advanced degenerative changes and flattening of the metatarsal head in late-stage Freiberg infraction.
Surgical Management
Surgery is generally not recommended during the acute inflammatory stage, which may persist for 6 months to 2 years. Conservative management with metatarsal pads, stiff-soled shoes, or a CAM boot is the first line of defense.
Operative intervention is indicated for chronic pain, severe deformity, and functional disability refractory to conservative care. Surgical options include:
1. Simple Debridement: Removal of loose bodies and synovectomy.
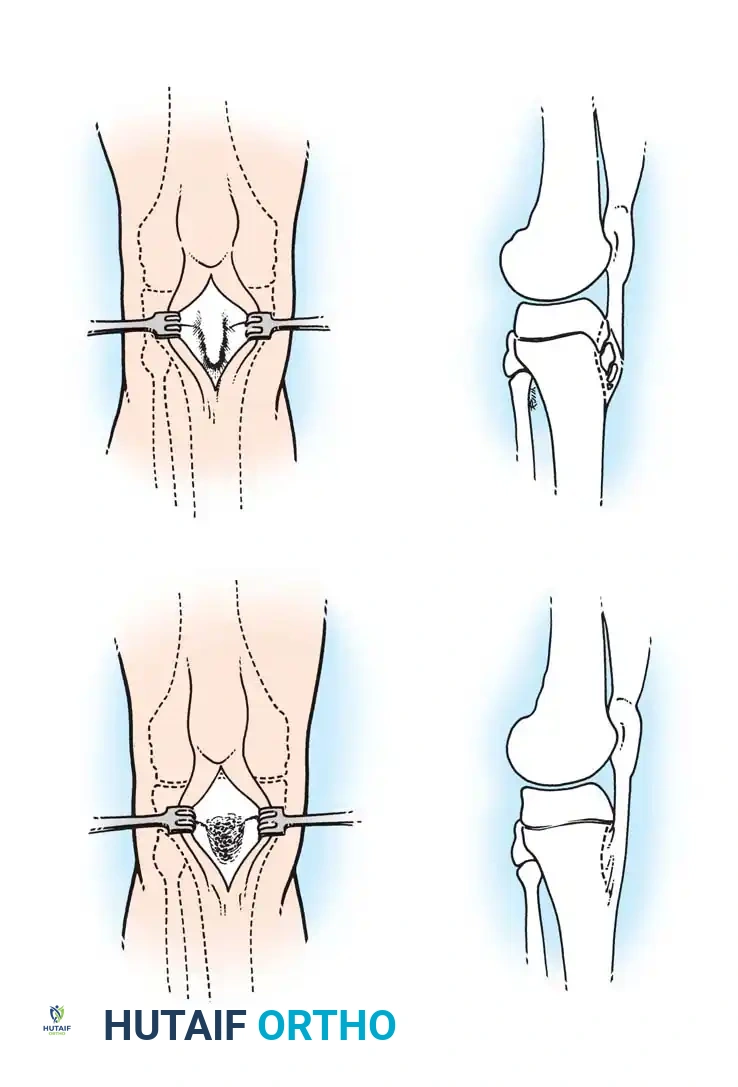
2. Smillie Procedure: Debridement of the necrotic subchondral bone and packing the defect with autogenous cancellous bone graft.
3. Dorsal Closing Wedge Osteotomy (Gauthier and Elbaz): The gold standard for symptomatic, deformed metatarsal heads.
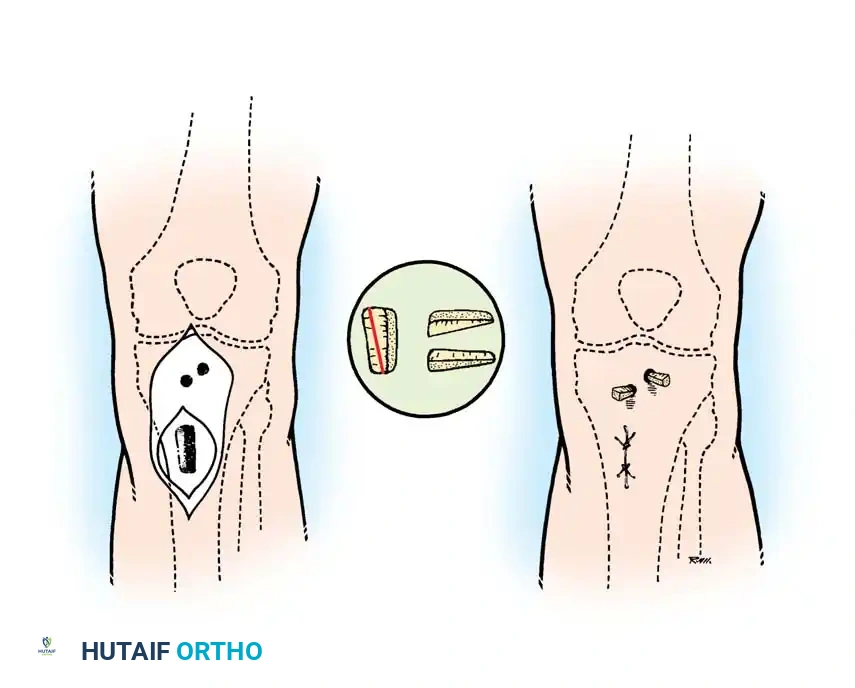
Step-by-Step: Dorsal Wedge Osteotomy
The goal of the dorsal wedge osteotomy is to rotate the healthy plantar articular cartilage dorsally to articulate with the proximal phalanx, effectively removing the necrotic dorsal lesion from the primary weight-bearing axis.
- Positioning and Approach: The patient is positioned supine. A dorsal longitudinal incision is made centered over the affected metatarsophalangeal (MTP) joint. The extensor tendons are retracted laterally.
- Joint Preparation: A dorsal capsulotomy is performed. The joint is inspected, and any loose bodies or hypertrophic synovium are excised.
- Osteotomy Execution: Using a microsaw, a dorsal-based wedge of bone is resected from the metatarsal neck, just proximal to the articular surface. The wedge must include the necrotic dorsal cartilage.
- Closure and Fixation: The osteotomy is closed by dorsiflexing the distal fragment, bringing the healthy plantar cartilage into the functional joint space. The osteotomy is rigidly fixed using a threaded K-wire or a low-profile micro-screw.
- Postoperative Protocol: The patient is placed in a rigid postoperative shoe, strictly non-weight-bearing on the forefoot for 4 to 6 weeks until radiographic union is confirmed.
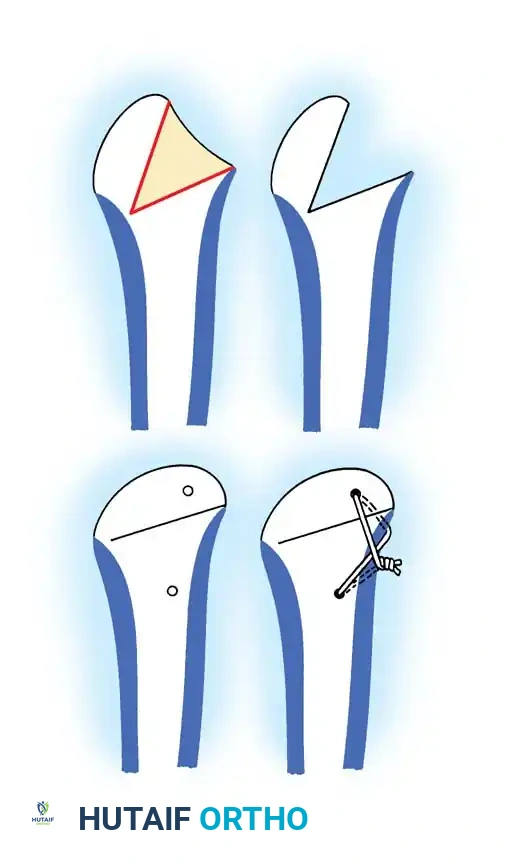
Osteotomy for Freiberg infraction: Outline of the bony wedge, resection, closure, and wire fixation.
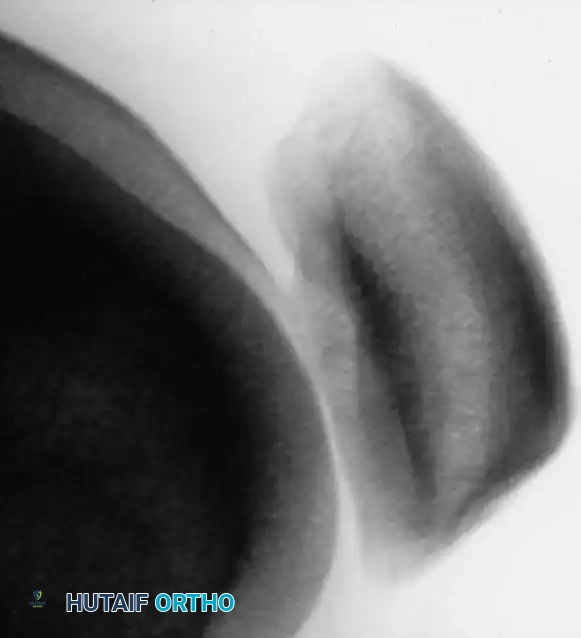
Postoperative radiographic appearance following corrective osteotomy and joint realignment.
Osteochondrosis of the Tarsal Navicular (Köhler Disease)
Originally described by Köhler in 1908, this osteochondrosis affects the tarsal navicular. Ossification centers of the navicular typically appear between 1.5 and 2 years of age in girls, and 2.5 and 3 years in boys.
Pathophysiology
Waugh's seminal anatomical studies described the unique blood supply to the pediatric navicular. The development of the ossific nucleus is frequently associated with a single artery. Waugh postulated that delayed ossification subjects the cartilaginous navicular to excessive mechanical pressure during weight-bearing. As the osseous vessels are compressed passing through the cartilage-bone junction, ischemia results, leading to reactive hyperemia, sclerosis, and pain.
Clinical Diagnosis and Imaging
Cowell and Williams emphasized that Köhler disease is primarily a clinical diagnosis requiring the presence of pain and tenderness directly over the tarsal navicular, coupled with characteristic radiographic changes.

Lateral and oblique radiographs demonstrating the smaller, highly sclerotic, and flattened navicular characteristic of Köhler disease.
Diagnostic Pitfall: The appearance of multiple ossification centers in the navicular without an increase in radiographic density should not be confused with Köhler disease. In an asymptomatic foot, this is merely a normal variant of irregular ossification.
Management Protocol
Köhler disease is inherently self-limiting. Cowell and Williams demonstrated that patients treated with short-leg cast immobilization experienced significantly quicker resolution of symptoms compared to those managed without casting.
Operative treatment is exceedingly rare in the pediatric phase. However, pain and disability occasionally develop in adulthood if the navicular heals with severe distortion and sclerosis. This can lead to flattening of the talar head, fibrillation of the articular surfaces, and massive osteophyte formation.
Surgical Arthrodesis for Late Sequelae
When disabling midfoot arthrosis persists, arthrodesis is the only definitive surgical solution.
* Talonavicular and Calcaneocuboid Fusion: The calcaneocuboid joint is routinely included because isolated talonavicular fusion eliminates nearly all midtarsal motion, placing excessive stress on adjacent joints.
* Technique: The joints are approached via a dorsal-lateral incision. The sclerotic articular cartilage is aggressively denuded down to bleeding subchondral bone. Autogenous cancellous bone graft (often harvested from the proximal tibia or iliac crest) is packed into the defects. Rigid internal fixation is achieved with crossed compression screws or a low-profile midfoot plating system.
* Naviculocuneiform Involvement: If symptoms arise from the naviculocuneiform joints, these must be included in the fusion mass. Arthrodesis here is notoriously difficult to secure; robust metallic internal fixation and inlay grafts are mandatory.

Advanced midfoot degenerative changes requiring extensive arthrodesis and structural grafting.
Osteochondritis of the Ankle
Osteochondritis dissecans (OCD) of the ankle primarily affects the talar dome. The natural history of this lesion in children with open physes is highly favorable compared to adult populations.
Natural History and Imaging
Bauer et al., in a long-term follow-up study (≥ 20 years) of 30 children with ankle osteochondritis, found that only one patient developed severe osteoarthritis. The vast majority experienced complete healing with only minor residual radiographic changes. This is in stark contrast to osteochondritis of the knee, where secondary osteoarthritis is a frequent complication.


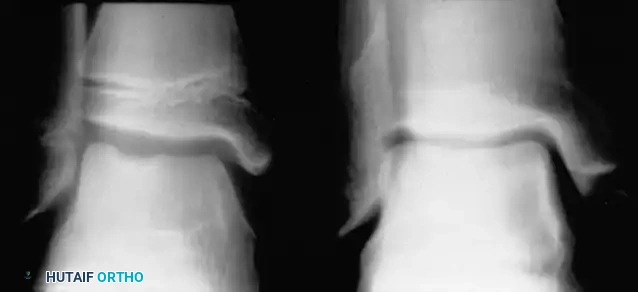
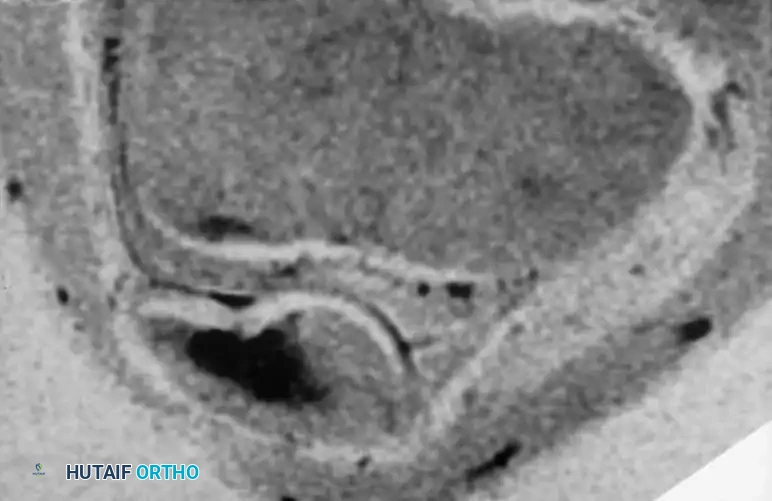
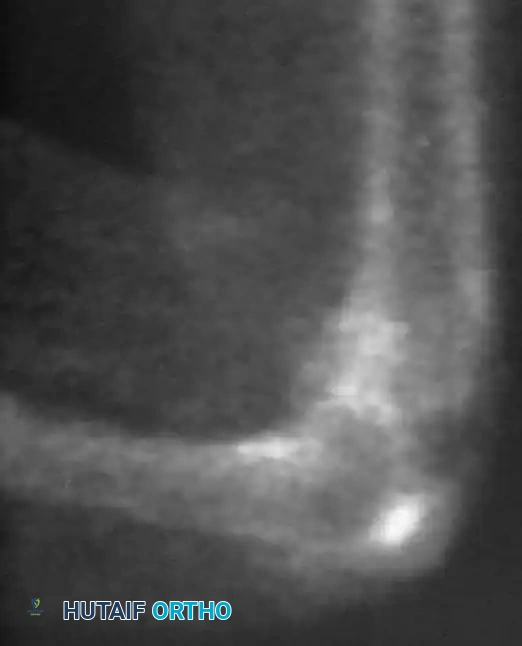
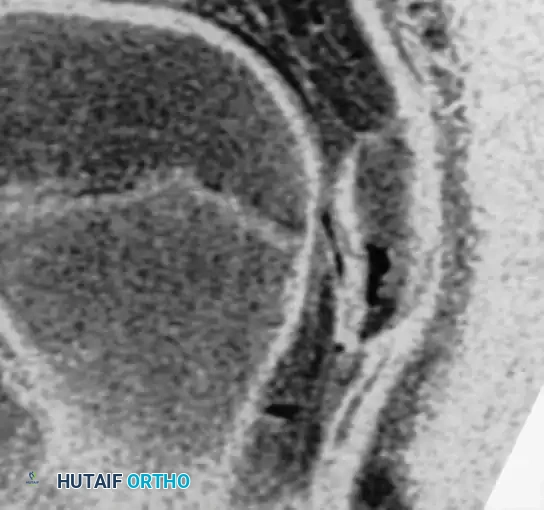
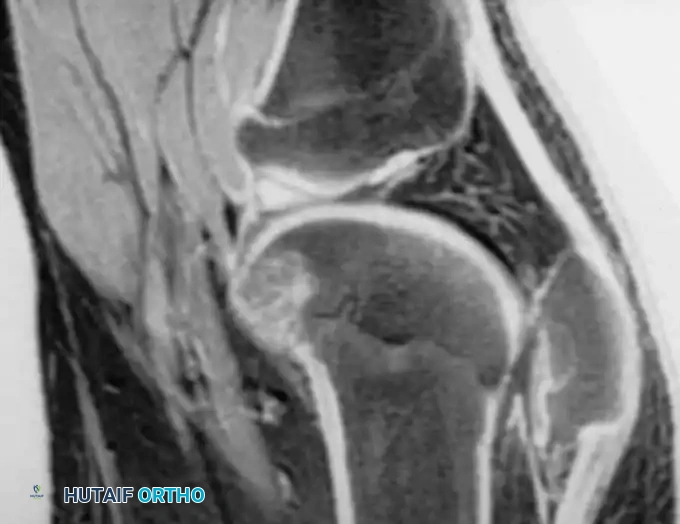
Radiographic and MRI evaluation of osteochondral lesions of the talar dome, demonstrating subchondral separation and surrounding edema.





📚 Medical References
You Might Also Like


