Comprehensive Guide to Physeal Injuries: Classification & Surgery
Key Takeaway
Physeal injuries account for nearly 30% of pediatric long bone fractures, demanding precise anatomical reduction to prevent premature growth arrest and angular deformity. Management hinges on accurate classification, predominantly utilizing the Salter-Harris system. While types I and II often respond to closed reduction, types III and IV typically necessitate open reduction and internal fixation (ORIF) to restore joint congruity and preserve the germinal matrix of the physis.
PHYSEAL INJURIES: EPIDEMIOLOGY AND BIOMECHANICS
The occurrence of specific pediatric fractures is intrinsically linked to the skeletal maturity and age of the child. The physis (growth plate) represents a unique biomechanical weak point in the pediatric skeleton, often failing before the adjacent ligaments or joint capsules under traumatic loading. In a comprehensive review of 2,650 long bone fractures in children up to 16 years of age, Mann and Rajmaira demonstrated that physeal injuries accounted for 30% of all pediatric fractures. These injuries occur twice as often in the upper extremities compared to the lower extremities. Furthermore, skeletal maturity dictates injury timing; girls sustaining physeal fractures are, on average, 1.5 years younger than boys presenting with the identical fracture pattern in the same anatomical location.
A consistent fracture pattern exists for each physis and its adjacent joint, dictated by local anatomy and the mechanism of injury. For instance, the vast majority of lateral humeral condylar fractures occur between the ages of 3 and 7 years, presenting with only one or two predictable fracture patterns. In the lower extremity, ankle fractures caused by an adduction force almost universally traverse the distal tibial physis at the medial plafond, an injury that can occur across a broad age spectrum. Conversely, physeal fractures on the lateral aspect of the distal tibia are almost exclusively seen in older adolescents. These are typically Salter-Harris type III fractures occurring as the medial physis closes while the lateral physis remains open (the classic Tillaux fracture).
Clinical Pearl: The biomechanical failure of the physis typically occurs through the zone of hypertrophic cartilage or the zone of provisional calcification. However, the fracture line frequently undulates, occasionally crossing into the germinal or proliferating zones, which accounts for the unpredictable nature of growth arrest even in seemingly benign injuries.
CLASSIFICATION OF PHYSEAL INJURIES
Historically, injuries involving the physis and epiphysis have been notorious for causing the cessation of longitudinal growth and resultant angular deformities. Accurate classification is paramount for guiding treatment, predicting prognosis, and communicating effectively among orthopedic surgeons. While these injuries have been classified by Weber et al., Poland, and Ogden, the most universally adopted system remains that of Salter and Harris.
The Salter-Harris Classification
The Salter-Harris (SH) classification is based on the radiographic appearance of the fracture and depicts the anatomical involvement of the physis, the epiphysis, and the adjacent joint. The prognostic value of this system is well-established: the higher the classification grade, the greater the likelihood of physeal arrest or joint incongruity.
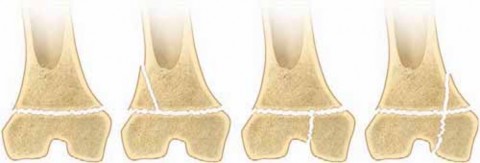
- Type I: Epiphyseal separations through the physis only, with or without displacement. The germinal cells remain with the epiphysis. Stress radiographs are often required to diagnose non-displaced Type I fractures.
- Type II: The fracture traverses the physis and exits through the metaphysis, producing a metaphyseal bony spike attached to the separated epiphysis (the Thurston-Holland sign). This is the most common physeal fracture.
- Type III: An intra-articular fracture that traverses the physis and exits through the epiphysis into the joint space. This creates joint incongruity if displaced and requires precise anatomical reduction.
- Type IV: An intra-articular fracture that passes through the metaphysis, crosses the physis, and exits through the epiphysis into the joint. This carries a high risk of both joint incongruity and physeal bridge formation.
- Type V: A severe compression injury to the physis that crushes the germinal cartilage cells. This injury is notoriously difficult to diagnose acutely and is usually identified only in retrospect when premature growth arrest or angular deformity becomes clinically apparent.
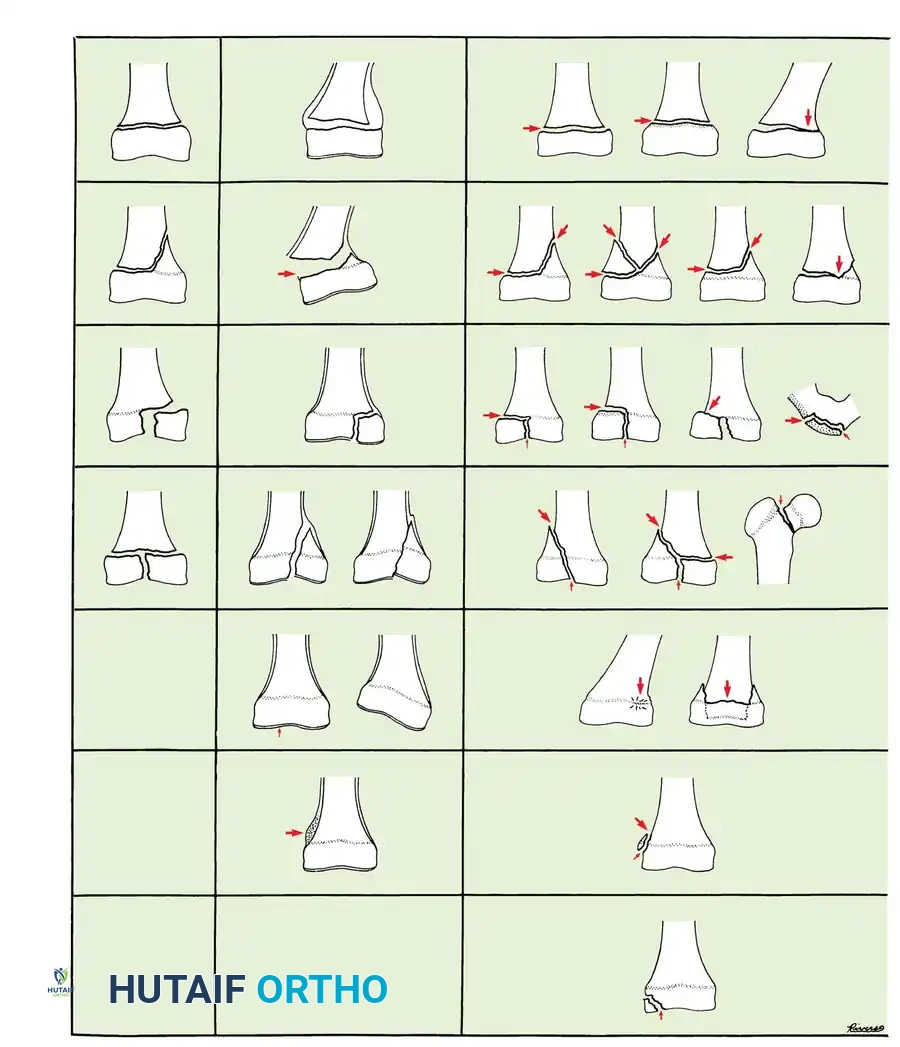
Fig. 33-1 Classification of physeal injuries by Poland, Salter and Harris, and Ogden. All three systems are similar, but from left to right are increasingly complex. The Salter-Harris classification is a refinement of Poland’s system, and Ogden’s classification, which is all-inclusive, adds more subclasses to simpler systems.
Modifications and Advanced Classifications
Peterson's Critique of Type V: Peterson questioned the validity of the Salter-Harris Type V compression injury. He noted the uniform, complete closure of the physis in injuries where other fracture patterns (not caused by compressive forces) occurred in the same extremity. He suggested that further investigation is required to understand the exact pathophysiology of uniform premature physeal closure.
Rang's Type VI: Rang modified the Salter-Harris classification by describing a "bruise" or contusion to the perichondrial ring (the periphery of the physis). This seemingly minor avulsion or contusion can cause localized scarring, tethering, and peripheral physeal arrest, which is the most crucial area regarding the development of severe angular deformity.
Ogden's Classification: Ogden devised a highly comprehensive classification system that accommodates almost every conceivable fracture pattern in every physis. His first five classes mirror Salter and Harris, but he introduced subclasses for complex fracture patterns in specialized joints (e.g., the proximal femur) and traction apophyses. Ogden's Type VI is analogous to Rang's perichondrial ring injury. Type VII represents an intra-articular osteochondral fracture. Types VIII and IX do not directly involve the physis or epiphysis but alter local vascularity, thereby stimulating the physis and contributing to longitudinal bone overgrowth.
Peterson's Unclassified Types: Peterson described two previously unclassified physeal fractures that carry significant clinical implications:
1. A fracture completely across the metaphysis with a linear, longitudinal extension to the physis. This fracture usually does not propagate along the physis itself.
2. A severe injury where a portion of the physis is entirely missing. This is invariably an open fracture resulting from high-energy trauma (e.g., lawnmower injuries). It mandates aggressive open reduction, internal fixation, and frequently requires late reconstructive surgery due to inevitable premature physeal closure.
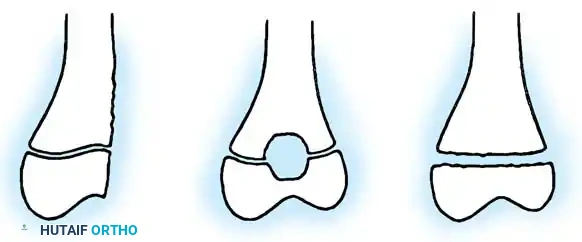
Fig. 33-2 A, Fractures of metaphysis with extension to physis. B, Fractures of physis with portion of physis missing. (From Peterson HA: Physeal fractures: 2. Two previously unclassified types, J Pediatr Orthop 14:431, 1994.)
ADVANCED DIAGNOSTIC IMAGING
While orthogonal plain radiographs remain the gold standard for initial evaluation, advanced imaging is increasingly utilized for complex or occult physeal injuries. Smith et al. demonstrated that Magnetic Resonance Imaging (MRI) scans obtained within 10 days of the fracture can alter the Salter-Harris classification, particularly in confusing fracture patterns that are difficult to interpret on plain films (e.g., unossified epiphyses in toddlers). Furthermore, early MRI (performed 3 to 17 weeks post-injury) can detect transphyseal bridging or altered growth lines long before these catastrophic complications become apparent on plain radiographs, allowing for earlier surgical intervention.
PRINCIPLES OF SURGICAL MANAGEMENT
We routinely utilize the Salter-Harris classification to guide treatment, operating under the strict realization that any physeal injury may result in growth disturbance, though the risk is exponentially higher following SH Type III, IV, and V fractures.
Closed vs. Open Reduction
Most SH Type I and II fractures can be managed successfully with prompt, gentle closed reduction and cast immobilization. However, there are critical exceptions. A Type II distal femoral physeal fracture that is significantly displaced carries a notoriously high rate of growth arrest and angular deformity. A meticulously gentle, closed anatomical reduction is required to avoid crushing the germinal cells in the proximal fragment; even with perfect technique, the physis may close prematurely.
SH Type III and IV fractures inherently involve the articular surface and the transphyseal vertical component. These injuries frequently require Open Reduction and Internal Fixation (ORIF) to reposition the fragments anatomically and fix them securely. This dual objective ensures that longitudinal growth may continue and that the joint remains congruous to prevent early-onset osteoarthritis.
Surgical Warning: The lateral humeral condyle fracture is a classic "fracture of necessity." It is a SH Type IV equivalent that almost always requires ORIF. If treated non-operatively or inadequately, the fracture fluid prevents union, leading to nonunion, progressive cubitus valgus, tardy ulnar nerve palsy, and severe joint incongruity.
Similarly, while some historical literature suggests that non-displaced Type III and IV distal tibial fractures can be treated closed, Bright noted that these fractures frequently displace within the cast as swelling subsides, leading to the formation of a physeal bony bridge. Consequently, it is highly recommended that almost all Type III and IV distal tibial fractures undergo ORIF, regardless of the initial degree of displacement.
Fixation Biomechanics and Implant Selection
When internal fixation is required, the primary biomechanical goal is absolute stability of the articular surface without compressing or tethering the physis.
- Avoid Crossing the Physis: Whenever anatomically possible, fixation should not cross the growth plate. In SH Type III fractures, pins or screws should be placed transversely across the epiphysis. In SH Type II fractures, fixation should be confined to the metaphyseal fragment.
- Transphyseal Fixation: If crossing the physis is absolutely necessary to maintain reduction, only smooth K-wires should be used. Threaded K-wires or screws crossing the physis will cause immediate tethering and growth arrest. Smooth pins should be placed centrally (avoiding the periphery) and perpendicular to the physis to minimize the cross-sectional area of physeal damage.
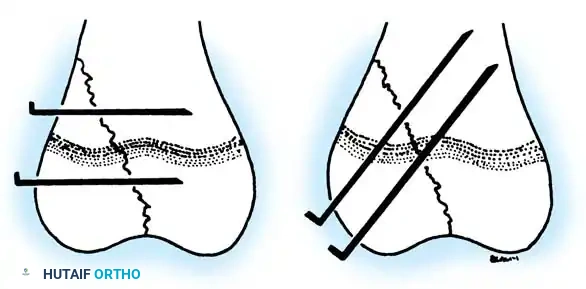
Fig. 33-3 Fixation of physeal fracture. A, Correct placement of parallel smooth pins across epiphysis and metaphysis. B, Smooth pins may cross physis if necessary to hold reduction. (From Ogden JA: Skeletal injury in the child, Philadelphia, 1982, Lea & Febiger.)
Biodegradable Fixation: Böstman et al. described the use of biodegradable polyglycolic acid (PGA) pins across the physis for distal humeral fractures. They reported excellent temporary fixation without secondary displacement or signs of growth disturbance, eliminating the need for a secondary hardware removal procedure. However, caution is advised. The degradation process of PGA and polylactic acid (PLA) implants can cause significant sterile osteolysis, foreign-body giant cell reactions, and sinus tract formation. The variability of resorption makes their routine use in transphyseal fixation controversial.
SURGICAL APPROACH: STEP-BY-STEP ORIF OF A SALTER-HARRIS IV FRACTURE
The following outlines the standard operative protocol for a displaced SH Type IV fracture (e.g., lateral humeral condyle or medial malleolus).
1. Preoperative Planning and Positioning
- Obtain high-quality orthogonal radiographs. Consider a CT scan with 3D reconstructions for complex intra-articular comminution.
- Position the patient appropriately (e.g., supine with a hand table for upper extremity; supine with a radiolucent triangle for the ankle).
- Ensure the availability of a pediatric mini-C-arm image intensifier.
2. Surgical Approach
- Utilize an extensile, internervous approach to expose the joint surface directly. For the lateral condyle, a lateral Kocher approach is utilized, elevating the extensor origin anteriorly to visualize the joint line.
- Crucial Step: Do not strip the posterior soft tissues or the vascular supply to the epiphysis, as this can lead to avascular necrosis (AVN) of the fragment.
3. Joint Debridement and Reduction
- Irrigate the fracture hematoma. Remove interposed periosteum or organizing clot from the fracture site using a dental pick or small curette.
- Under direct visualization of the articular cartilage, anatomically reduce the epiphyseal component. Use a small pointed reduction forceps (Weber clamp) to hold the reduction.
- Verify the reduction fluoroscopically in two planes.
4. Internal Fixation
- Drive two smooth K-wires (typically 1.6mm or 2.0mm depending on the child's age) divergently across the fracture site.
- For a SH IV, attempt to place one wire transversely through the epiphysis and one transversely through the metaphysis, avoiding the physis entirely.
- If transphyseal fixation is unavoidable, ensure the smooth wires cross the physis at the most perpendicular angle possible.
- Bend the K-wires outside the skin to facilitate removal in the clinic, or cut them beneath the skin if prolonged fixation is anticipated.
5. Postoperative Protocol
- Apply a well-padded, bivalved cast or rigid splint.
- Maintain non-weight-bearing status (or non-use for upper extremity) for 3 to 4 weeks.
- Remove smooth K-wires at 3 to 4 weeks in the outpatient clinic once early callus is visible on radiographs.
- Initiate a structured physical therapy program to restore joint range of motion.
COMPLICATIONS: PHYSEAL ARREST AND RECONSTRUCTIVE SURGERY
Despite optimal management, physeal injuries can result in premature growth arrest, leading to limb length discrepancy (LLD) or angular deformity. The parents must be fully informed of this possibility at the time of the initial injury.
Bony Bridge (Physeal Bar) Resection
If a localized bony bridge forms across the physis, it acts as a tether. In younger children with significant remaining growth potential, Langenskiöld and Bright pioneered the technique of bony bridge resection.
* Indications: The bar should involve less than 50% of the cross-sectional area of the physis, and the child must have at least 2 years of growth remaining.
* Technique: The bar is precisely mapped using MRI or CT. A surgical approach is made, and the bony tether is meticulously resected using a high-speed burr until healthy, pearly-white physis is visualized circumferentially.
* Interposition: To prevent recurrence, an inert material must be interposed into the defect. Autologous fat grafts, Cranioplast (methylmethacrylate), or bone wax have been used successfully.
Osteotomy and Deformity Correction
Peterson established that in young children, if the angular deformity is less than 20 degrees, bony bridge resection alone may allow the physis to spontaneously correct the alignment. However, if the deformity exceeds 20 degrees, a concomitant corrective osteotomy is mandatory.
The tolerance for angular deformity varies by anatomical location:
* Upper vs. Lower Extremity: More angular deformity can be tolerated in the upper extremity due to the compensatory range of motion of the shoulder and elbow.
* Coronal Plane: Valgus deformity is generally better tolerated than varus deformity.
* Sagittal Plane: Flexion deformities are better tolerated than extension deformities.
* Proximity to Trunk: In the lower extremity, proximal deformities (hip) are compensated for better than distal deformities (ankle).
Limb Length Discrepancy (LLD) Management
If growth ceases symmetrically across the entire physis, significant shortening will occur.
* Epiphysiodesis: In a young child, epiphysiodesis (surgical arrest) of the contralateral, healthy limb can be performed to equalize leg lengths at maturity. This is frequently done percutaneously under fluoroscopic control using a drill or curette.
* Lengthening: For severe discrepancies in older children, distraction osteogenesis (Ilizarov or intramedullary lengthening nails) may be indicated.
* Growth Prediction: Accurate timing of epiphysiodesis requires meticulous evaluation using the Green-Anderson tables or the Moseley straight-line graph, utilizing serial scanograms and bone age assessments.
In the upper extremity, absolute length is less critical to function. Pritchett's studies on physeal activity demonstrate that skeletal maturity occurs 1 to 2 years earlier in girls than in boys. Approximately 80% of the longitudinal growth of the humerus occurs at the proximal physis, whereas in the forearm, approximately 85% of the growth of the radius and ulna occurs at their distal physes.
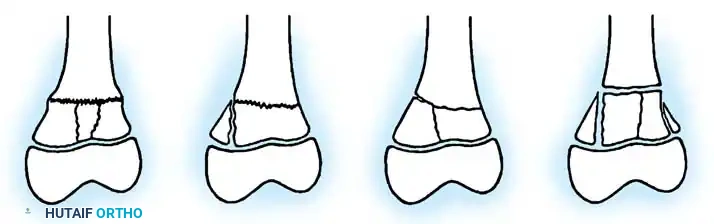
Fig. 33-4 Physeal growth contributions in the upper extremity.
SPECIAL CONSIDERATIONS: OPEN PHYSEAL AND DIAPHYSEAL FRACTURES
Historically, it was assumed that pediatric bone possesses such robust healing potential that even severe open fractures would unite without complication. This dogma has been challenged.
Golz et al. reported on the results and complications following primary external fixation of 40 open lower extremity diaphyseal fractures in children. Their findings definitively refute the assumption that Gustilo Type II and III open fractures heal readily in the pediatric population. Patients younger than 17 years exhibited high incidences of delayed union and nonunion, although the incidence of chronic osteomyelitis was lower than that seen in adults with comparable injuries.
Management Protocol for Open Fractures:
* Immediate administration of intravenous antibiotics (cephalosporin ± aminoglycoside depending on Gustilo grade).
* Urgent surgical debridement. Frequent, vigorous debridement and pulsatile irrigation of the open wound every 36 to 48 hours is mandatory until the wound is pristine.
* Adequate, rigid stabilization of the fracture (via external fixation or flexible intramedullary nailing) is critical to decrease the rates of nonunion and infection.
Clinical Pitfall: Rarely, hematogenous osteomyelitis can occur at the site of a closed fracture, even without the use of skeletal traction pins or local anesthetic injections. Surgeons must maintain a high index of suspicion if a child with a closed physeal injury presents with unexplained systemic toxicity, escalating pain, or rising inflammatory markers out of proportion to the initial trauma.
📚 Medical References
- physeal injuries in rabbits, J Bone Joint Surg 70A:1383, 1988.
- Wheelock SM, Lookinland S: Effect of surgical hand scrub time on subsequent bacterial growth, AORN J 65:1087, 1997.
- Wong KC, Leung KS: Transmission and prevention of occupational infections in orthopaedic surgeons, J Bone Joint Surg 86A:1065, 2004.
- Diagnosis Abreu SH: Skeletal uptake of In-111–labeled white blood cells, Semin Nucl Med 19:152, 1989.
- Becker W, Palestro CJ, Winship J, et al: Rapid imaging of infections with a monoclonal antibody fragment (LeukoScan), Clin Orthop Relat Res 329:263, 1996.
- Beltran J, Noto AM, McGhee RB, et al: Infections of the musculoskeletal system: high-fi eld strength MR imaging, Radiology 164:449, 1987.
- Boutin RD, Brossmann J, Sartoris DJ, et al: Update on imaging of orthopedic infections, Orthop Clin North Am 29:41, 1998.
- Bushberg JT, Hoffer PB, Schreiber GJ, et al: Comparative uptake of Ga-67 and Tc-99m MDP in rabbits with a benign noninfected bone lesion (fracture), Invest Radiol 20:498, 1985.
- Crokaert F, Schoutens A, Wagner J, et al: Gallium-67 citrate as an aid to the diagnosis of infection in hip surgery, Int Orthop 6:163, 1982.
- Datz FL, Thorne DA: Effect of antibiotic therapy on the sensitivity of indium-111–labeled leukocyte scans, J Nucl Med 27:1849, 1986.
- DeLuca PA, Gutman LT, Ruderman RJ: Counterimmunoelectrophoresis of synovial fl uid in the diagnosis of septic arthritis, J Pediatr Orthop 5:167, 1985.
- Demopulos GA, Bleck EE, McDougall IR: Role of radionuclide imaging in the diagnosis of acute osteomyelitis, J Pediatr Orthop 8:558, 1988.
- DeWinter F, Van de Wiele C, Vogelaers D, et al: Fluorine-18 fl uorodeoxyglucose-positron emission tomography: a highly accurate imaging modality for the diagnosis of chronic musculoskeletal infections, J Bone Joint Surg 83A:651, 2001.
- Dietz FR, Koontz FP, Found EM, et al: The importance of positive bacterial cultures of specimens obtained during clean orthopaedic operations, J Bone Joint Surg 73A:1200, 1991.
- Faden H, Grossi M: Acute osteomyelitis in children: reassessment of etiologic agents and their clinical characteristics, Am J Dis Child 145:65, 1991.
- Hakki S, Harwood S, Morissey M, et al: Comparative study of monoclonal antibody scan in diagnosing
You Might Also Like