Pediatric Hip Fractures: Comprehensive Surgical Management and Techniques
Key Takeaway
Pediatric hip fractures are rare but carry a high risk of severe complications, including osteonecrosis, coxa vara, and premature physeal closure. Successful management requires a deep understanding of the Delbet classification, precise surgical timing, and meticulous technique. This guide details evidence-based protocols for closed and open reduction, capsular decompression, and internal fixation to optimize outcomes in the growing skeleton.
INTRODUCTION TO PEDIATRIC HIP FRACTURES
Hip fractures in children—encompassing fractures of the femoral head, femoral neck, and intertrochanteric region—are rare, high-energy injuries that constitute less than 1% of all pediatric fractures. Unlike adult hip fractures, which are typically fragility fractures treated with standardized arthroplasty or fixation protocols, pediatric hip fractures present a unique and formidable challenge. Most orthopaedic surgeons will encounter these injuries only a handful of times throughout their careers.
Although these fractures frequently occur in conjunction with life-threatening polytrauma, their most defining characteristic is the devastating profile of late complications. Osteonecrosis (avascular necrosis [AVN]), coxa vara, nonunion, and premature physeal closure are alarmingly common. The necessity of aggressive, precise operative intervention is paramount, though often difficult for parents to accept in the acute setting.
Clinical Pearl: The pediatric proximal femur is not merely a smaller version of the adult femur. The presence of the capital femoral physis, the precarious extraosseous blood supply, and the dense, hard cortical bone of the femoral neck dictate entirely different biomechanical and biological treatment strategies.
Fig. 1: Premature closure of the triradiate cartilage following severe pelvic and hip trauma, illustrating the profound impact of injury on the growing pediatric pelvis.
VASCULAR ANATOMY AND BIOMECHANICS
Understanding the vascular anatomy of the pediatric hip is the cornerstone of managing these fractures. The blood supply to the capital femoral epiphysis changes dynamically from birth to skeletal maturity.
- Infancy (0-4 years): The metaphyseal vessels cross the physis to supply the epiphysis.
- Childhood (4-8 years): As the physis thickens, it forms an impenetrable barrier to metaphyseal blood flow. The epiphysis becomes entirely dependent on the lateral epiphyseal vessels (terminal branches of the medial circumflex femoral artery [MCFA]).
- Adolescence (8+ years): The ligamentum teres provides a variable, often negligible, contribution to the epiphyseal blood supply.
Because the intracapsular femoral neck lacks a robust periosteal layer, healing depends entirely on endosteal callus formation. Furthermore, the dense bone of the pediatric femoral neck requires meticulous drilling and tapping during internal fixation to prevent distraction of the fracture or iatrogenic physeal separation.
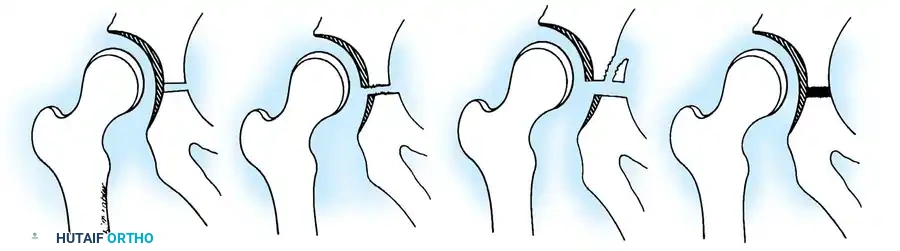
Fig. 2: Schematic representation of the hemipelvis and types of pediatric injuries, highlighting the vulnerability of the physis.
CLASSIFICATION OF PEDIATRIC HIP FRACTURES
The classification system proposed by Delbet and popularized by Colonna, later modified by Ingram and Bachynski, remains the universal standard for categorizing pediatric hip fractures. It is highly predictive of the risk of osteonecrosis and guides surgical decision-making.
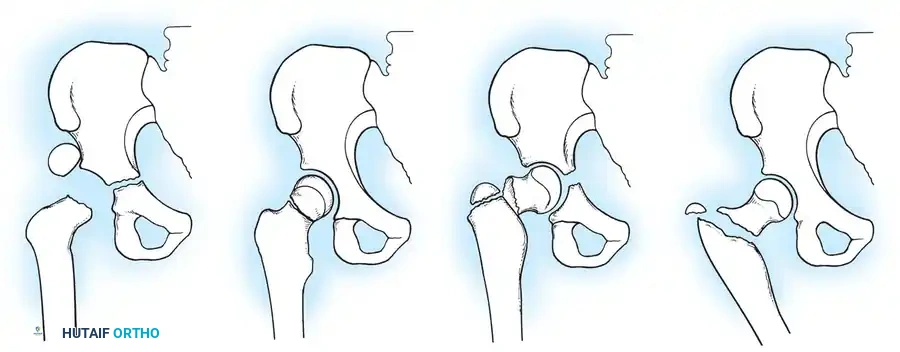
Fig. 3: The Delbet Classification of Pediatric Hip Fractures (Types I, II, III, and IV).
Type I: Transepiphyseal Separations
Type I fractures are transepiphyseal separations, occurring with or without dislocation of the femoral head from the acetabulum. These are the rarest but most devastating injuries, carrying an osteonecrosis rate approaching 100% when associated with dislocation. The physis contributes to a Salter-Harris Type I or II separation.
Type II: Transcervical Fractures
Transcervical fractures are the most common pediatric hip fractures. They occur through the mid-portion of the femoral neck. Because the fracture is entirely intracapsular, the tamponade effect of the fracture hematoma severely compromises the MCFA. The AVN rate for Type II fractures historically exceeds 50% if displaced.
Type III: Cervicotrochanteric Fractures
These fractures occur at the base of the femoral neck. While similar to adult basicervical fractures, they carry a significantly higher risk of osteonecrosis in children. They are highly unstable and prone to varus collapse if not rigidly fixed.
Type IV: Intertrochanteric Fractures
Occurring between the greater and lesser trochanters, Type IV fractures are extracapsular. Because of the robust periosteum and excellent osteogenic potential in the trochanteric region, these fractures heal rapidly (usually within 6 to 8 weeks) and carry the lowest risk of AVN and complications.

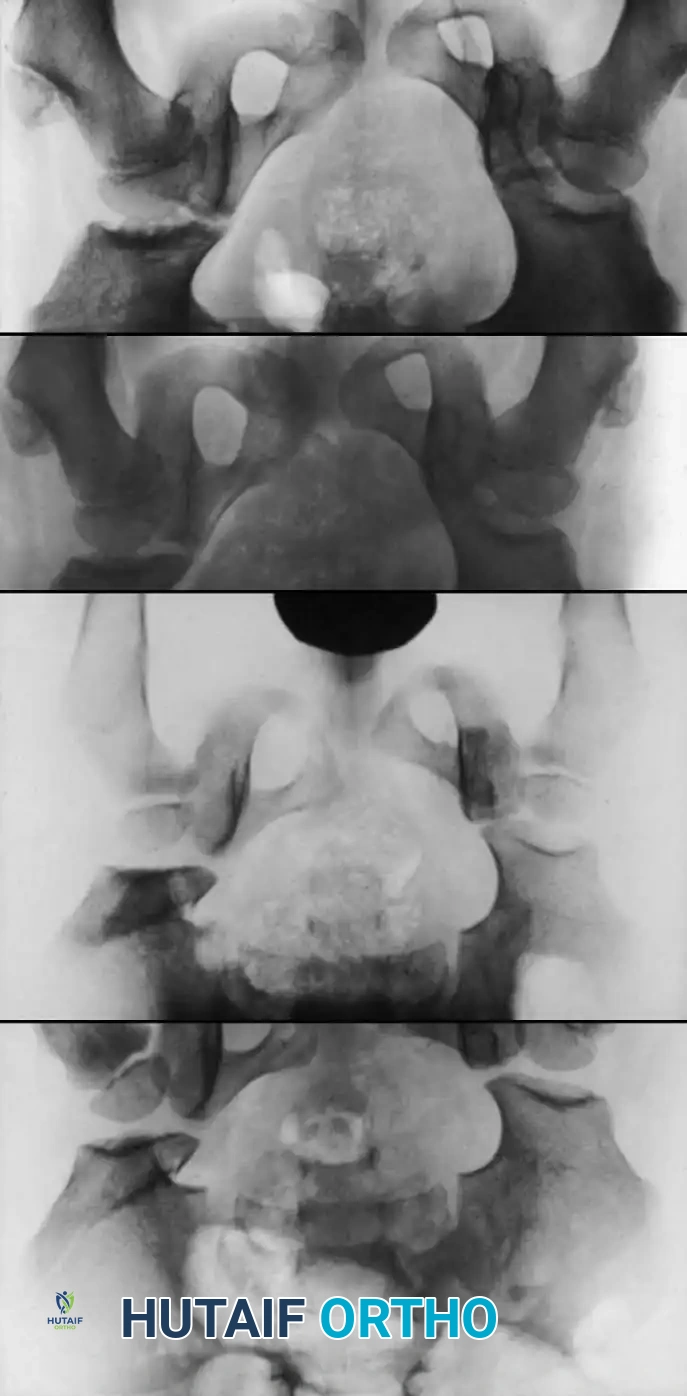
Fig. 4: Severe fracture-dislocation of the hip, demonstrating the high-energy nature of these injuries.

Fig. 5: Radiographic progression of a complex pediatric hip injury requiring extensive reconstruction.
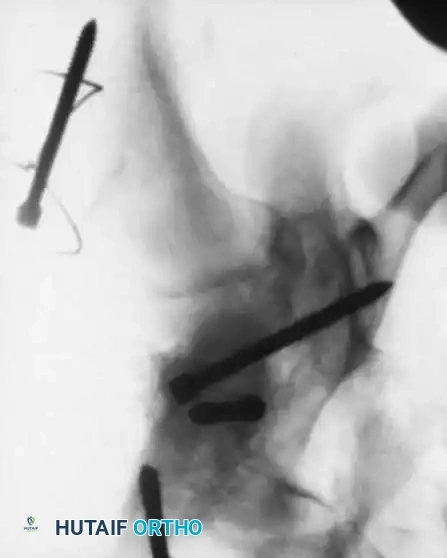
Fig. 6: Long-term follow-up showing severe ankylosis and traumatic arthritis secondary to osteonecrosis.
SURGICAL INDICATIONS AND TIMING
Pediatric hip fractures are orthopaedic emergencies. The primary goal is the anatomic reduction and stable internal fixation of the fracture to minimize the risk of osteonecrosis and coxa vara.
Surgical Warning: A child’s hip can tolerate immobilization much more readily than an adult's, but conservative management (spica casting alone) for displaced Type I, II, or III fractures almost invariably leads to varus collapse and nonunion. Internal fixation is mandatory for displaced fractures.
The Role of Capsular Decompression
The debate surrounding capsular decompression remains a critical topic in pediatric orthopaedics. Boitzy and Rang demonstrated that capsular distention causes a tamponade effect on the retinacular vessels. They advocated for emergency anterolateral capsular release, hematoma evacuation, and internal fixation, reporting significantly lower rates of AVN.
Conversely, Gerber et al. (reviewing AO hospital data) found that even with immediate open reduction and capsular release, the AVN rate remained around 30%, suggesting that the initial trauma to the vessels at the moment of displacement is the primary determinant of osteonecrosis.
Current Consensus: Despite the controversy, emergent capsular decompression (via aspiration or open arthrotomy) combined with anatomic reduction and stable fixation within 24 hours is the gold standard to give the femoral head the best possible chance of survival.
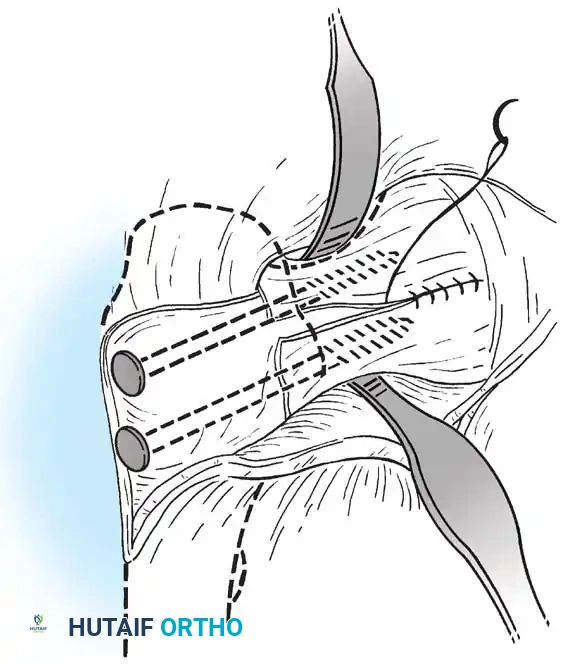
Fig. 7: Anterolateral capsular release and evacuation of hematoma. This emergency procedure is critical for relieving intracapsular tamponade.
STEP-BY-STEP SURGICAL MANAGEMENT BY FRACTURE TYPE
Management of Type I: Transepiphyseal Separations
Transepiphyseal separations yield the worst outcomes in pediatric hip trauma. If the femoral head is dislocated, open reduction is almost always necessary.
- Imaging: If the direction of the dislocation (anterior vs. posterior) is unclear on plain radiographs, an emergent CT scan is mandatory.
- Surgical Approach:
- For anterior dislocations, utilize a Watson-Jones approach. This allows direct visualization for reduction and hardware insertion.
- For posterior dislocations, a modified Gibson approach is preferred to protect the remaining posterior vascular tether.
- Reduction: Gentle, direct manipulation of the epiphysis into the acetabulum. Avoid forceful levering that could further damage the MCFA.
- Fixation: In older children, cannulated hip screws can be used. However, in infants and young children, crossing the physis with threaded screws will cause premature physeal closure and severe leg-length discrepancy.
- Technique: Use specially manufactured smooth pins (unthreaded) to secure the epiphysis. Note that smooth pins lack compression and may migrate; therefore, postoperative spica casting is mandatory.

Fig. 8: Type I transepiphyseal separation treated with closed reduction and fixation using cannulated hip screws in an older child.

Fig. 9: Intraoperative fluoroscopy confirming pin placement across the physis.
Special Consideration: Proximal Femoral Epiphysiolysis in Newborns
In neonates, a Type I separation can occur due to birth trauma. It presents as pseudoparalysis and can be misdiagnosed as developmental dysplasia of the hip (DDH) or septic arthritis. MRI or arthrogram is diagnostic. Operative fixation is rarely needed; spica casting is sufficient as rapid remodeling occurs.
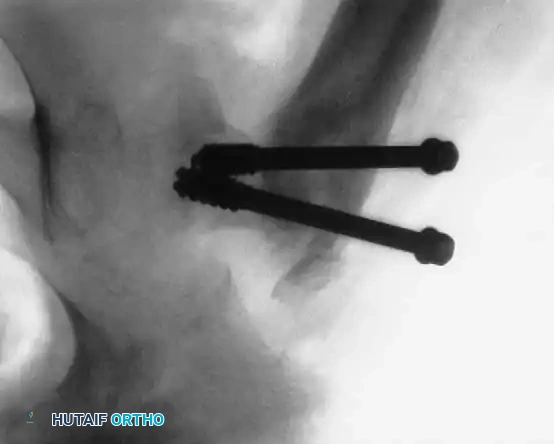
Fig. 10: Arthrogram demonstrating proximal femoral epiphysiolysis in a young infant.
Management of Type II: Transcervical Fractures
Type II fractures are highly unstable. Even seemingly nondisplaced fractures will drift into coxa vara if treated with a spica cast alone.
- Positioning: Place the patient supine on a radiolucent flat table or a pediatric fracture table.
- Reduction: Perform a gentle closed reduction using longitudinal traction, abduction, and internal rotation. Verify anatomic alignment on AP and lateral fluoroscopy.
- Capsular Decompression: If closed reduction is achieved, perform a percutaneous capsular aspiration or a limited (1-2 cm) arthrotomy to evacuate the hematoma.
- Fixation:
- Use two or three partially threaded cannulated screws (typically 4.5 mm or 6.5 mm depending on the child's size).
- Crucial Step: The pediatric femoral neck is extremely hard. You must overdrill the near cortex to achieve a lag effect and prevent fracture distraction.
- Stop the threads short of the physis to prevent growth arrest. Do not use adult triflanged nails, as the impaction force will distract the fracture or separate the physis.
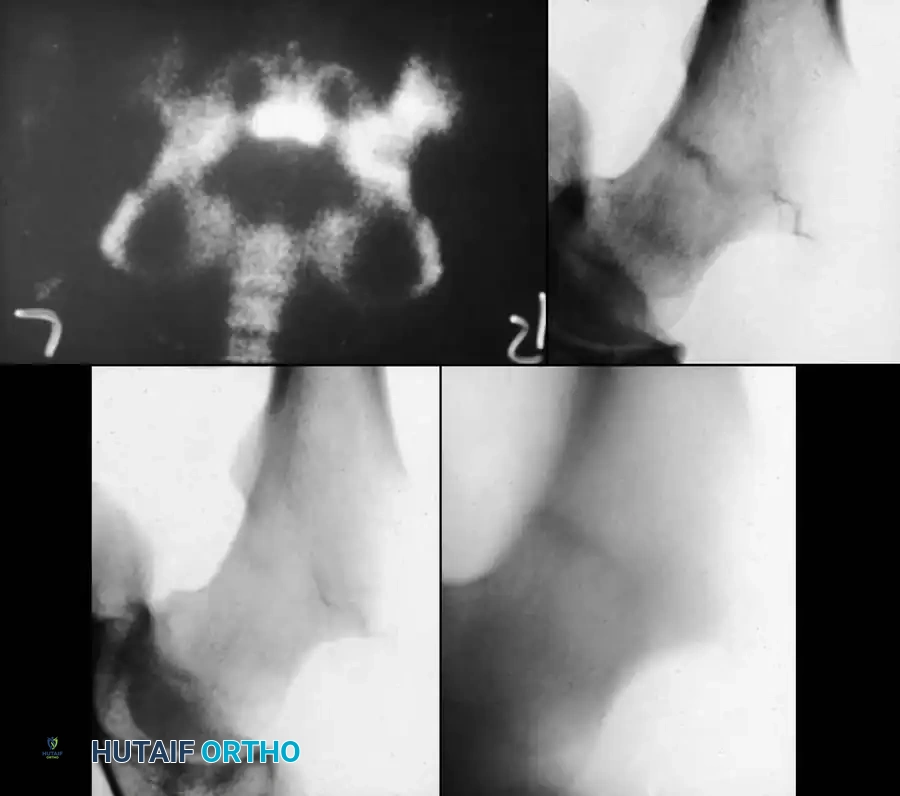
Fig. 11: Transcervical fracture stabilized with cannulated screws stopping short of the capital femoral physis.

Fig. 12: Lateral fluoroscopic view confirming central placement of the screws within the femoral neck.

Fig. 13: Postoperative radiograph showing healed Type II fracture with maintained neck-shaft angle.
Management of Type III: Cervicotrochanteric Fractures
Type III fractures experience massive shear forces. While historically treated with pins, the high rate of varus collapse and nonunion has shifted the paradigm toward more rigid constructs.
- Reduction: Closed reduction on a fracture table.
- Fixation: For "low" cervicotrochanteric fractures, simple screw fixation is often inadequate due to the lack of cortical support inferiorly.
- Technique: Utilize a pediatric dynamic hip screw (DHS) or a cannulated screw with an attached side plate. This converts shear forces into compressive forces and rigidly maintains the neck-shaft angle.

Fig. 14: Displaced Type III cervicotrochanteric fracture prior to intervention.

Fig. 15: Intraoperative reduction of the Type III fracture.

Fig. 16: Final fixation utilizing a cannulated screw and attached side plate to neutralize shear forces.
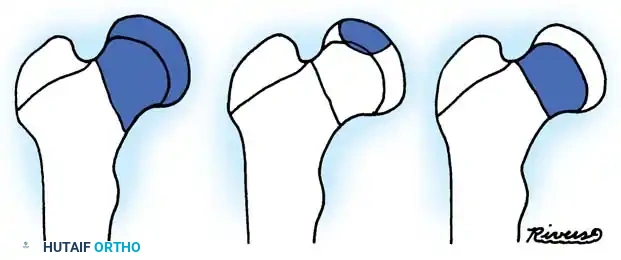
Fig. 17: Alternative fixation strategy using multiple screws for a high cervicotrochanteric variant.

Fig. 18: Healed Type III fracture demonstrating robust callus formation at the base of the neck.
Management of Type IV: Intertrochanteric Fractures
Type IV fractures have the best prognosis. Because of the rich blood supply and thick periosteum, nonunion and AVN are rare.
- Conservative Management: In younger children, skeletal traction (90-90 femoral traction) for 2 to 3 weeks until early callus forms, followed by a 1.5 spica cast for 6 weeks, is highly effective.
- Operative Management: In older children, adolescents, or polytrauma patients, operative fixation is preferred to allow early mobilization.
- Technique: Closed reduction and internal fixation using a pediatric locking proximal femoral plate or a dynamic hip screw.

Fig. 19: Intertrochanteric fracture managed with a pediatric proximal femoral locking plate.

Fig. 20: Lateral view of plate fixation ensuring no hardware encroaches on the trochanteric apophysis.

Fig. 21: Complete consolidation of a Type IV fracture at 12 weeks post-op.
POSTOPERATIVE PROTOCOLS
Unlike adults, children are highly noncompliant with partial weight-bearing instructions. Therefore, hardware alone is rarely trusted to withstand the forces of an active child.
- Immobilization: A one-and-a-half (1.5) hip spica cast is routinely applied postoperatively for 6 weeks in children under 10 years of age. The hip is positioned in slight abduction and internal rotation to relax the capsule and maintain compression across the fracture site.
- Adolescents: In older, compliant adolescents treated with rigid side-plate constructs, spica casting may be omitted in favor of strict non-weight-bearing on crutches for 6 to 8 weeks.
- Hardware Removal: Routine removal of hardware is generally recommended in children once complete radiographic union is achieved (typically 6-12 months post-op) to prevent hardware migration, overgrowth, or interference with future reconstructive procedures.
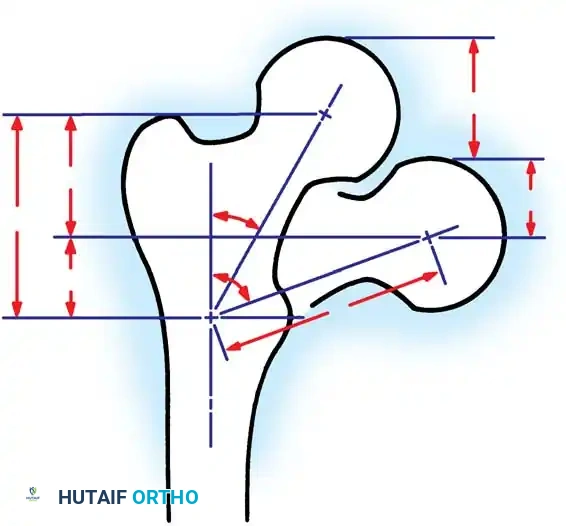
Fig. 22: Application of a postoperative hip spica cast to protect the internal fixation.
COMPLICATIONS AND SALVAGE PROCEDURES
The management of pediatric hip fractures is fraught with complications, even when executed perfectly.
1. Osteonecrosis (Avascular Necrosis)
AVN is the most dreaded complication, occurring in up to 50% of displaced Type I and II fractures. It typically presents radiographically 6 to 12 months post-injury as sclerosis, fragmentation, and eventual collapse of the femoral head.
* Management: Treatment is challenging. Options include prolonged non-weight-bearing, core decompression, or proximal femoral varus osteotomy to contain the fragmented head within the acetabulum (similar to Legg-Calvé-Perthes disease principles).
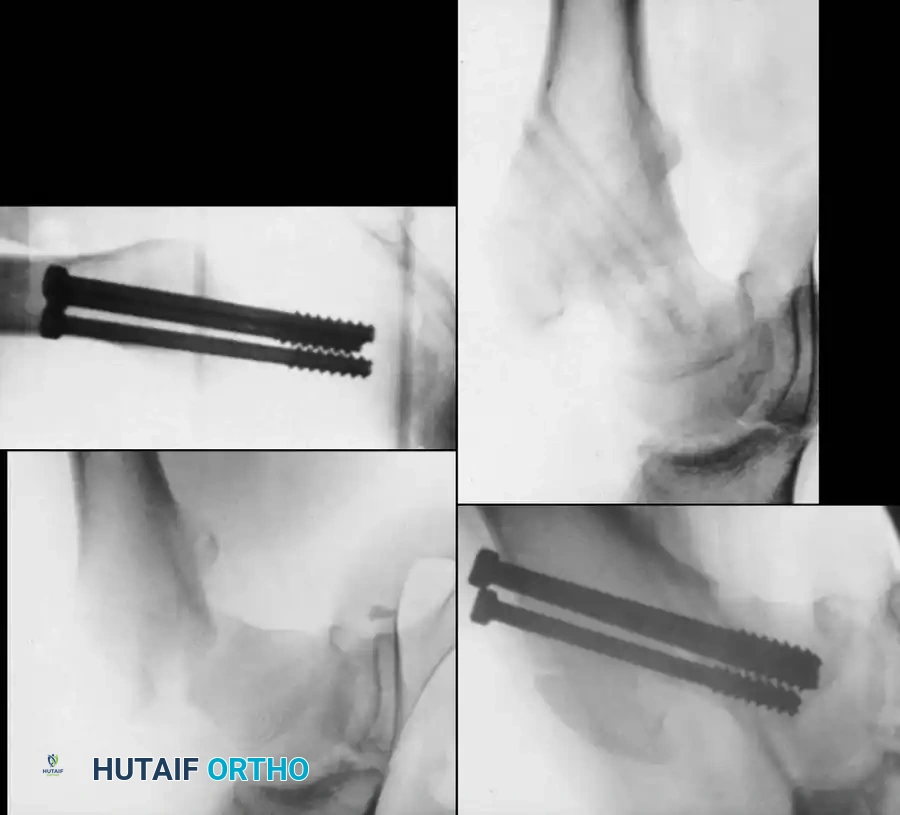
Fig. 23: Severe osteonecrosis with head collapse following a Type II transcervical fracture.
2. Coxa Vara
Coxa vara (neck-shaft angle < 120 degrees) results from loss of reduction, inadequate fixation, or premature closure of the medial aspect of the capital physis. It leads to a Trendelenburg gait and limb shortening.
* Management: If the varus deformity is progressive or the neck-shaft angle falls below 110 degrees, a subtrochanteric valgus-producing osteotomy is indicated to restore biomechanics and abductor tension.
3. Premature Physeal Closure
Injury to the physis from the initial trauma or iatrogenic damage from threaded hardware can cause complete or partial growth arrest. Complete arrest leads to limb-length discrepancy (the proximal femur contributes 15% of total leg length). Partial arrest leads to angular deformities (varus or valgus).
* Management: Contralateral epiphysiodesis may be required for limb-length equalization if the discrepancy is projected to exceed 2-3 cm at skeletal maturity.

Fig. 24: Limb-length discrepancy and coxa breva resulting from premature physeal closure.
4. Nonunion
Nonunion is rare when rigid internal fixation is utilized but was historically common with cast-only treatment. It is treated with valgus-producing subtrochanteric osteotomy to convert shear forces at the nonunion site into compressive forces, often supplemented with autologous bone grafting.
CONCLUSION
The operative management of pediatric hip fractures demands a profound respect for the fragile vascular anatomy and the biomechanical forces at play in the growing femur. Adherence to the principles of emergent capsular decompression, anatomic reduction, rigid internal fixation tailored to the child's age, and appropriate postoperative immobilization will mitigate—though not entirely eliminate—the high risks of osteonecrosis and growth disturbance. Continuous, long-term radiographic follow-up until skeletal maturity is mandatory for all pediatric patients sustaining these severe injuries.
You Might Also Like

