Pediatric Fractures of the Humeral Shaft and Proximal Physis: A Comprehensive Surgical Guide
Key Takeaway
Pediatric humeral shaft and proximal physeal fractures possess immense remodeling potential, typically resolving with nonoperative management. However, severe displacement, radial nerve entrapment, or soft tissue buttonholing may necessitate surgical intervention. This guide details evidence-based protocols, from closed reduction maneuvers to percutaneous pinning and open reduction techniques, ensuring optimal outcomes while minimizing physeal injury and neurovascular complications in the growing skeleton.
FRACTURES OF THE SHAFT AND PROXIMAL END OF THE HUMERUS
The management of pediatric humeral fractures requires a profound understanding of physeal biomechanics, immense remodeling potential, and the specific pathoanatomy associated with the growing skeleton. While the vast majority of these injuries can be managed nonoperatively with excellent functional outcomes, the orthopedic surgeon must be adept at identifying the critical exceptions—such as neurovascular compromise, soft tissue interposition, and severe displacement—that mandate operative intervention.
This comprehensive guide delineates the evidence-based protocols for managing fractures of the humeral midshaft and the proximal humeral physis, detailing indications, surgical approaches, and postoperative rehabilitation.
FRACTURES OF THE HUMERAL SHAFT IN CHILDREN
Biomechanics and Nonoperative Management
Fractures of the midshaft of the humerus in children possess an extraordinary capacity for healing. Nonunion in this demographic is exceedingly rare, and the robust periosteal sleeve ensures rapid callus formation. When treated conservatively—most commonly utilizing a hanging-arm cast, coaptation splint, or functional brace—shortening, angulation, and rotary deformities are typically minimal and clinically insignificant due to the compensatory range of motion of the shoulder and elbow joints.
Consequently, open reduction and internal fixation (ORIF) for isolated, closed pediatric humeral shaft fractures is almost never indicated.
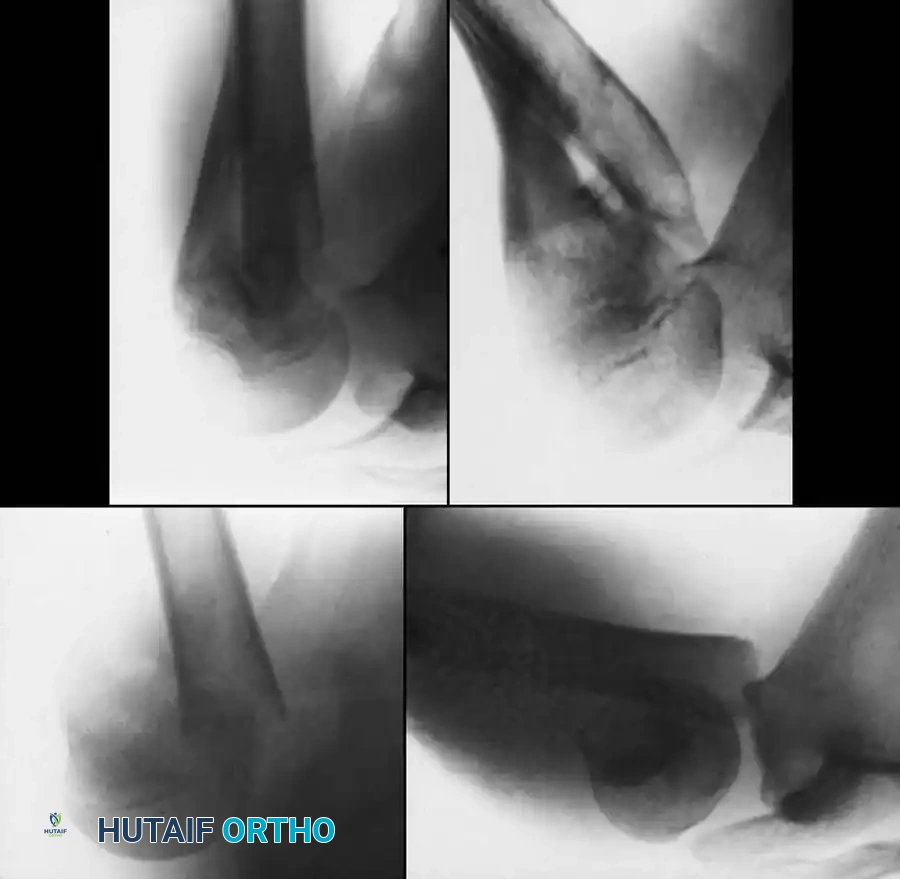
Fig. 33-92 Proximal humeral shaft fracture. A and B, Severely displaced fracture not involving the physis. C and D, Good remodeling of the fracture with a satisfactory range of motion after poor reduction, highlighting the immense remodeling potential in the pediatric population.
The Radial Nerve Conundrum
A critical clinical scenario arises in fractures located at the junction of the middle and distal thirds of the humeral shaft (analogous to the Holstein-Lewis fracture in adults).
🚨 SURGICAL WARNING: Iatrogenic Radial Nerve Palsy
If the radial nerve is documented as intact upon initial presentation, but its motor or sensory function disappears immediately following a closed reduction maneuver, the surgeon must assume the nerve has become entrapped between the fracture fragments.
This loss of function is an absolute indication for surgical exploration. The entrapped nerve must be meticulously extricated from the fracture site, followed by internal fixation of the fracture to prevent secondary nerve injury and ensure skeletal stability. The principles of fixation in these pediatric cases mirror those in adults, utilizing either dynamic compression plating or flexible intramedullary nailing depending on the child's age and skeletal maturity.
FRACTURES OF THE PROXIMAL HUMERUS
Epidemiology and Classification
While proximal shaft fractures occasionally occur, the vast majority of proximal humerus fractures in the pediatric population are physeal injuries. The proximal humeral physis contributes approximately 80% of the longitudinal growth of the humerus, endowing it with unparalleled remodeling capabilities.
These injuries are most accurately categorized using the Salter-Harris Classification:
* Salter-Harris Type I: Occur predominantly in infants and younger children. The fracture line propagates entirely through the hypertrophic zone of the physis.
* Salter-Harris Type II: The most common pattern in older children and adolescents. The fracture line traverses the physis and exits through the metaphysis, creating a Thurston-Holland fragment.
* Salter-Harris Type III and IV: Extremely rare in the proximal humerus. These intra-articular fractures carry a higher risk of growth arrest and joint incongruity.
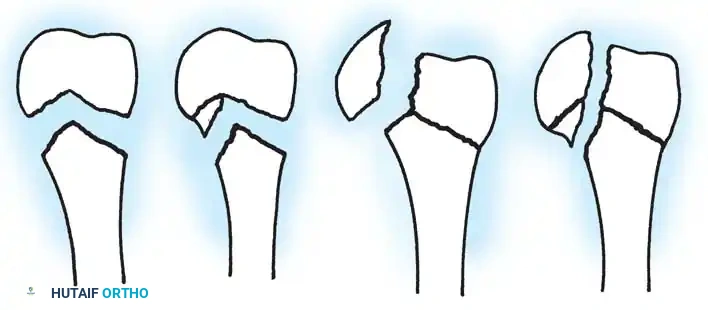
Fig. 33-93 Salter-Harris classification of proximal humeral physeal injuries. Types I and II are extremely common; types III and IV are extremely rare.
🛑 CLINICAL PEARL: Non-Accidental Trauma (NAT)
A severe fracture or physeal injury of the proximal humerus in an infant or very young child (particularly those under 3 years of age) should immediately raise a high index of suspicion for child abuse. A thorough skeletal survey and pediatric safeguarding consultation are mandatory.
Neer and Horowitz Classification
To guide treatment based on displacement, Neer and Horowitz classified proximal humeral physeal fractures into four grades:
* Grade I: Displacement of less than 5 mm.
* Grade II: Displacement up to one-third of the shaft width.
* Grade III: Displacement up to two-thirds of the shaft width.
* Grade IV: Total displacement (greater than two-thirds or complete loss of cortical contact).
Remodeling Potential and the Periosteal Sleeve
The thick, robust periosteum in children rarely tears completely. In proximal humeral fractures, the periosteum typically tears on the tension side but remains intact on the compression side, creating a "periosteal hinge." This hinge not only aids in closed reduction but also directs the massive remodeling potential of the proximal physis.
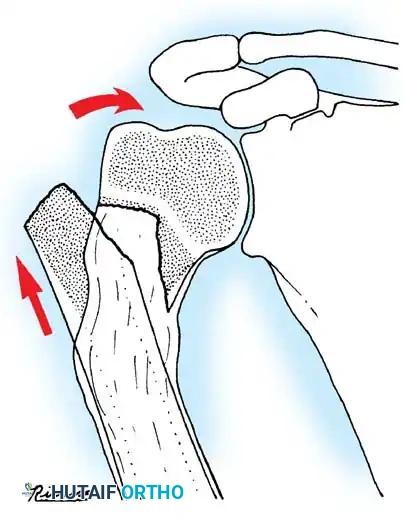
Fig. 33-94 Remodeling potential of proximal humeral physeal fracture because of the intact periosteal sleeve, which guides new bone formation and realigns the mechanical axis over time.
Larsen et al., in a landmark review of 65 patients with proximal humeral metaphyseal or physeal fracture-separations, demonstrated that full remodeling reliably occurred. They concluded that nonoperative treatment is highly appropriate for proximal humeral fractures in children up to age 15 years, even in the presence of extensive displacement.
INDICATIONS FOR OPERATIVE INTERVENTION
Despite the overwhelming success of conservative management, Dameron and Reibel noted that while most displaced Salter-Harris Type I and II fractures resolve with conservative care, specific pathoanatomic scenarios necessitate surgical intervention.
Absolute and Relative Indications for Surgery
- Irreducible Severe Displacement: When closed reduction fails to achieve acceptable alignment in an older adolescent nearing skeletal maturity.
- Soft Tissue Buttonholing: The distal shaft fragment is frequently pulled proximally and medially by the pectoralis major, while the proximal fragment is abducted and externally rotated by the rotator cuff. The distal fragment can "buttonhole" completely through the anterior periosteum and the deltoid muscle, impinging against the dermis. If this cannot be repositioned closed, open reduction is required.
- Salter-Harris Type III and IV Fractures: These rare intra-articular injuries require anatomic reduction to prevent premature physeal closure and glenohumeral arthritis.
- Biceps Tendon Interposition: The long head of the biceps tendon can become incarcerated in the fracture site, blocking closed reduction.
- Fracture-Dislocations: Require immediate reduction of the joint and stabilization of the fracture.
- Open Fractures: Mandate emergent irrigation, debridement, and stabilization.
⚠️ PITFALL: The Risks of Open Reduction
Beringer et al. reported on 48 patients with severely displaced proximal humeral epiphyseal fractures. Of the nine patients who underwent open treatment, three experienced severe complications (including avascular necrosis, infection, and hardware failure). Consequently, operative intervention should be avoided whenever possible, reserved strictly for the absolute indications listed above.
SURGICAL TECHNIQUES
Closed Reduction and Percutaneous Pinning (CRPP)
When a fracture is severely displaced and unstable, closed reduction followed by percutaneous pinning under fluoroscopic guidance is the preferred minimally invasive approach.
TECHNIQUE 33-25: Sherk and Probst
This technique leverages the predictable deforming forces of the shoulder musculature to achieve reduction without opening the fracture site.
Step 1: Patient Positioning and Preparation
* Place the patient supine on a radiolucent operating table.
* Position the C-arm image intensifier to allow unobstructed orthogonal views (AP and axillary/scapular Y) of the proximal humerus.
* Prep and drape the entire forequarter to allow free manipulation of the arm.
Step 2: The Reduction Maneuver
* The proximal fragment is typically abducted, flexed, and externally rotated by the rotator cuff. To align the distal fragment with the proximal fragment, manipulate the arm into slight external rotation, 90 degrees of forward flexion, and 70 degrees of abduction.
* Apply longitudinal traction. This maneuver is designed to extract the upper part of the humeral shaft back through the rent in the deltoid muscle and anterior periosteum, correcting the anterior angulation.
* Have an assistant apply counter-traction and support the proximal fragment to help achieve and maintain the reduction.
Step 3: Stability Testing
* Once reduced under fluoroscopy, test for stability by gently bringing the distal fragment down out of flexion and abduction toward the anatomic position.
* If Stable: Apply a Velpeau dressing or sling-and-swathe. This is worn for 4 to 5 weeks until clinical union is sufficient to permit gentle, gravity-assisted shoulder motion.
* If Unstable (Redisplacement occurs): Repeat the reduction maneuver. The arm must be maintained in the "salute position" (abduction and flexion). The surgeon may choose to apply a shoulder spica cast or skin traction in this position, though this is poorly tolerated by patients.
Step 4: Percutaneous Pinning (The Alternative to Spica Casting)
* If the fracture is unstable upon bringing the arm down, percutaneous pinning is highly recommended to allow the arm to rest in a neutral, comfortable position.
* Drive one or two smooth Steinmann pins (typically 2.0 mm or 2.5 mm depending on patient size) through the lateral cortex of the distal shaft, directing them proximally and medially across the physis into the humeral head.
* Neurovascular Warning: Ensure pin entry is lateral and distal enough to avoid the axillary nerve, which courses approximately 5 to 7 cm distal to the lateral acromion.
* Verify pin placement and fracture reduction on both AP and axillary fluoroscopic views.
* Cut the pins beneath the skin to prevent pin-tract infections.
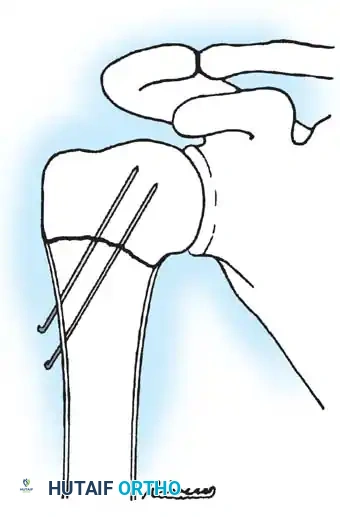
Fig. 33-95 Closed reduction and percutaneous pinning of a proximal physeal separation. Two smooth wires cross the physis to provide rotational and angular stability while minimizing physeal damage.
Step 5: Postoperative Protocol for CRPP
* Immobilize the arm in a neutral position using a sling or shoulder immobilizer.
* The buried pins are removed in the clinic under local anesthesia or light sedation at 3 to 4 weeks postoperatively, once early callus is visible radiographically.
* Initiate passive and active-assisted range of motion exercises immediately following pin removal.
Open Reduction and Internal Fixation (ORIF)
When closed reduction is impossible—most commonly due to the distal fragment buttonholing completely through the deltoid or the interposition of the biceps tendon—open reduction is mandatory.
Surgical Approaches
The surgeon may utilize either a short deltopectoral approach or a deltoid-splitting approach.
1. The Deltopectoral Approach (Preferred)
* Utilizes the internervous plane between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves).
* Identify and retract the cephalic vein (usually retracted laterally with the deltoid to protect its primary venous drainage).
* This approach provides excellent visualization of the anterior shoulder, allowing easy extraction of the buttonholed shaft and direct visualization of the long head of the biceps tendon if it is incarcerated.
2. The Deltoid-Splitting Approach
* A short, direct lateral incision splitting the anterior and middle thirds of the deltoid.
* Crucial Anatomy: The split must not extend further than 4 to 5 cm distal to the acromion to absolutely avoid transecting the axillary nerve, which runs transversely across the deep surface of the muscle.
* The shaft is reduced directly through the split deltoid muscle.
Fixation Strategy
Once the fracture is anatomically reduced under direct vision, it is typically stabilized using the same percutaneous pinning technique described above (smooth Steinmann pins driven laterally to medially).
For the rare Salter-Harris Type III or IV fractures, or complex fracture-dislocations, the surgical procedures and fixation constructs (which may require cannulated screws parallel to the physis) are similar to those necessary for Neer Type III or IV fractures in adults. However, extreme care must be taken to ensure that any compression screws do not cross the open physis, which would tether growth and lead to severe angular deformity.
Postoperative Rehabilitation and Outcomes
Following either closed or open management, the robust healing response of the pediatric humerus dictates a relatively rapid rehabilitation timeline.
* 0-3 Weeks: Strict immobilization. Pendulum exercises may begin at 2-3 weeks if stable.
* 3-4 Weeks: Hardware removal (if pinned). Transition to active-assisted range of motion (AAROM).
* 6-8 Weeks: Radiographic union is typically robust. Transition to full active range of motion (AROM) and progressive strengthening.
* Long-term: Remodeling of the proximal humerus will continue for months to years. Minor angular deformities will reliably correct in patients with more than 2 years of remaining growth. Follow-up should continue until full symmetric shoulder motion is restored and radiographic remodeling is confirmed.
You Might Also Like

