Pediatric Forearm Fractures: Comprehensive Operative and Closed Management
Key Takeaway
Pediatric forearm fractures are among the most common orthopedic injuries, with the majority occurring in the distal third. While closed reduction remains the gold standard for most cases, operative intervention—such as elastic stable intramedullary nailing (ESIN) or compression plating—is indicated for irreducible, open, or highly unstable fractures. Mastery of forearm biomechanics, precise surgical technique, and an understanding of physeal remodeling are essential for optimizing functional outcomes and preventing complications like malunion or growth arrest.
INTRODUCTION TO PEDIATRIC FOREARM FRACTURES
Forearm fractures are extremely common in the pediatric population, representing a significant portion of orthopedic trauma admissions. The fundamental principle governing the management of these injuries is that the vast majority of fractures, regardless of their level, do not require open reduction and internal fixation (ORIF). The robust remodeling potential of the pediatric skeleton, particularly near the physes, allows for the successful conservative management of deformities that would be strictly unacceptable in adults.
However, the threshold for surgical intervention changes based on the patient's age, the proximity of the fracture to the physis, and the inherent stability of the fracture pattern. A profound understanding of forearm biomechanics, muscular deforming forces, and precise radiographic evaluation is mandatory for the treating orthopedic surgeon to prevent long-term functional deficits, such as the loss of pronosupination or premature physeal closure.
BIOMECHANICS AND PRINCIPLES OF CLOSED REDUCTION
The forearm functions as a complex, articulated ring. The radius and ulna are bound by the interosseous membrane, and their relationship dictates the critical motion of pronation and supination. When a fracture occurs, the muscular attachments exert predictable deforming forces on the fracture fragments.
For successful closed reduction, the distal fragment must be aligned with the proximal fragment, which is controlled by these muscular forces. Most authors agree on the following immobilization positions based on the level of the fracture:
* Distal Third Fractures: The arm should be placed in pronation to counteract the pull of the brachioradialis and pronator quadratus.
* Middle Third (Diaphyseal) Fractures: The arm should be placed in a neutral position.
* Proximal Third Fractures: The arm should be placed in supination to match the proximal fragment, which is strongly supinated by the unopposed action of the biceps brachii and the supinator muscle.
Clinical Pearl: King’s Principle dictates that the radial bicipital tuberosity proximally and the radial styloid distally are best visualized in maximal supination. It is highly recommended that these two anatomical landmarks be properly aligned on the anteroposterior (AP) radiograph to ensure rotational reduction is accurate.
FRACTURES OF THE DISTAL THIRD OF THE FOREARM
Epidemiology and Pathoanatomy
Fractures of the distal third of the forearm are exceptionally common. Blount noted that approximately 75% of all pediatric forearm fractures occur in this region. The vast majority are dorsally displaced (Colles-type equivalents) and occur in the plane of motion of the radiocarpal joint. Because they are in the plane of joint motion and close to the highly active distal radial physis, they remodel remarkably well, provided the child has sufficient growth remaining.
Physeal Injuries and Growth Arrest
In addition to metaphyseal both-bone fractures, physeal fractures of the distal radius and ulna are frequently encountered. Salter-Harris type I and II fractures are the most common; types III and IV are exceedingly rare.
While these physeal injuries typically respond well to closed reduction and casting, complications can arise. Lee et al. reported cases of premature closure of the distal radial physis following either severe physeal compression injuries (Salter-Harris type V) or repeated, forceful attempts at closed reduction.
Surgical Warning: Repeated manipulation of a pediatric distal radius fracture significantly increases the risk of iatrogenic physeal damage. If the initial reduction achieves greater than 50% apposition with acceptable alignment, further forceful attempts at perfect anatomical reduction should be strictly avoided.
Zehntner et al. described growth disturbances caused by partial closure of the distal radial physis, leading to a pseudo-Madelung deformity. This tethering effect results in ulnar deviation of the radius and relative ulnar overgrowth.

Management of these growth arrests depends on the patient's age and remaining growth potential:
* Ulnar Shortening Osteotomy: For relative ulnar overgrowth.
* Opening Wedge Radial Osteotomy: To correct the articular inclination of the radius.
* Sauvé-Kapandji Procedure: A salvage option for severe distal radioulnar joint (DRUJ) incongruity.
* Epiphysiodesis: Of the contralateral or adjacent physis to prevent progressive deformity.
Indications for Operative Intervention in Distal Fractures
Surgical intervention for distal third fractures is rare but indicated in specific scenarios:
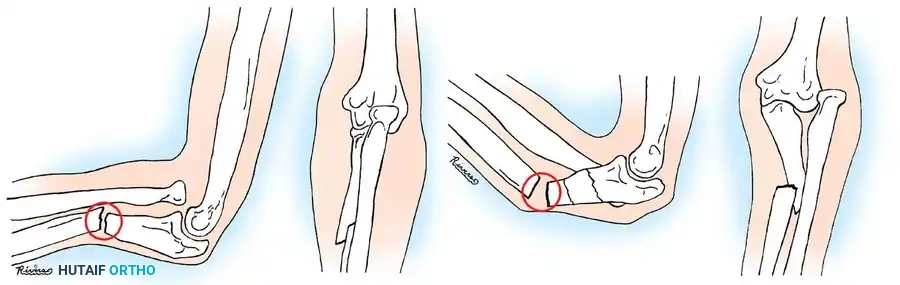
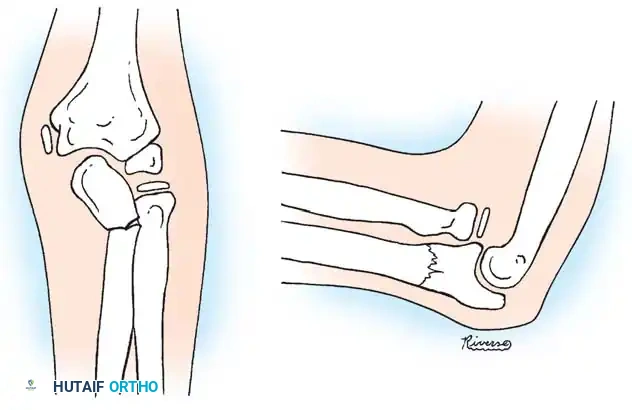
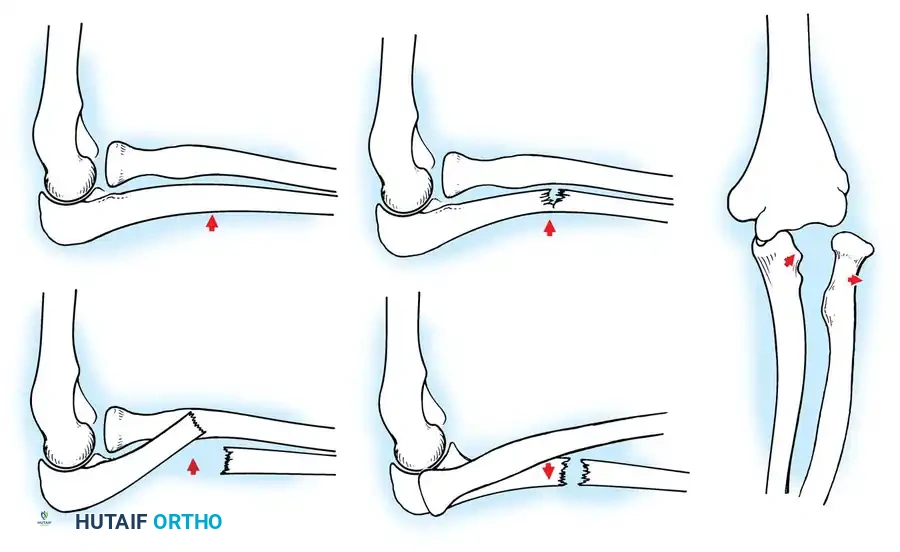
1. Soft-Tissue Interposition: Holmes and Louis identified entrapment of the pronator quadratus as a primary cause of irreducible distal radial fractures. This typically presents with volar angulation and dorsal translation of the distal fragment.
2. Open Fractures: Require thorough irrigation, débridement, and often stabilization.
3. Loss of Reduction: Voto et al. noted that 7% of closed reductions displace. Remanipulation is safe up to 24 days post-injury for nonphyseal fractures. If instability persists, percutaneous pinning is warranted.
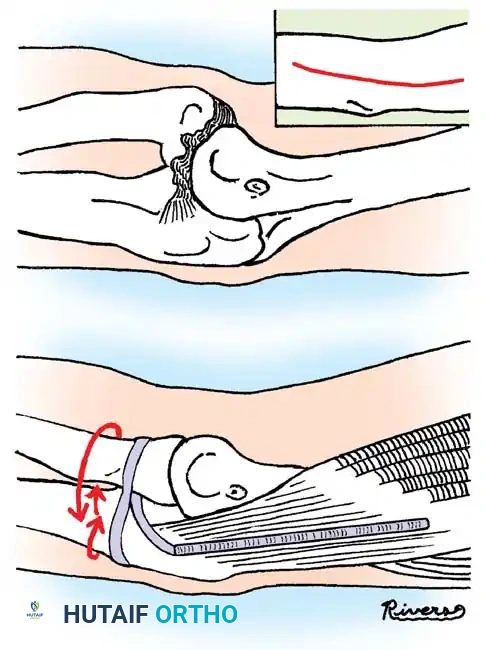
Surgical Technique: Open Reduction for Pronator Quadratus Entrapment
When closed reduction fails due to soft-tissue interposition, an open approach is required.
1. Approach: A dorsal longitudinal incision is made over the distal radius.
2. Dissection: The extensor retinaculum is incised. The interval between the third (extensor pollicis longus) and fourth (common digital extensors) dorsal compartments is developed.
3. Retraction: The tendons are retracted to expose the fracture site.
4. Reduction: The interposed pronator quadratus or periosteum is carefully extracted from the fracture site using a Freer elevator.
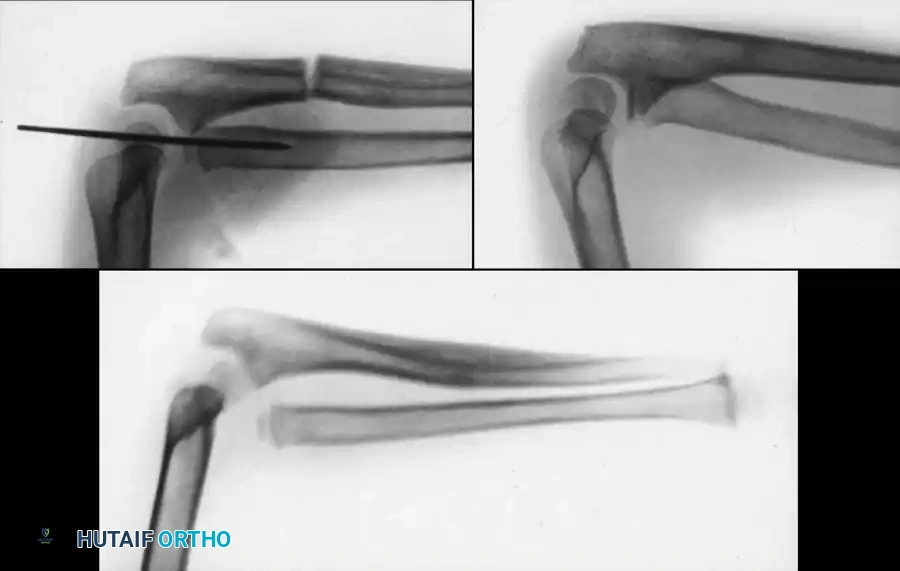
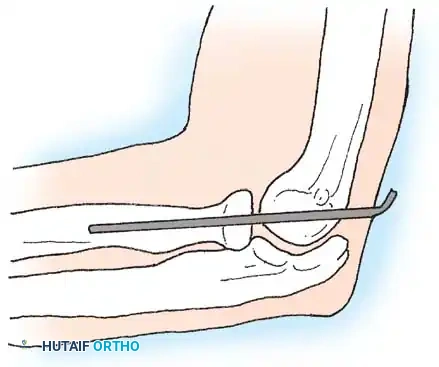
5. Fixation: Once reduced, the fracture is often stable. If inherently unstable, smooth Steinmann pins or Kirschner wires (K-wires) can be driven percutaneously across the fracture site, avoiding the physis if possible, or crossing it centrally and smoothly if necessary. Small plates should be used with extreme caution to avoid physeal damage.

FRACTURES OF THE MIDDLE THIRD (DIAPHYSEAL) OF THE FOREARM
Remodeling Potential and Acceptable Alignment
Diaphyseal fractures of the radius and ulna require careful assessment. Vittas et al. and Karaharju et al. emphasized that while the physis drives remodeling, this potential decreases significantly in late childhood and is less pronounced in the midshaft compared to the distal metaphysis.
Price et al. established widely accepted criteria for conservative management of diaphyseal both-bone fractures in skeletally immature patients. They concluded that anatomical alignment is ideal, but the following parameters are acceptable and will not lead to severe functional disability:
* Up to 40 degrees of malrotation.
* Up to 10 degrees of angulation.
* Complete displacement (bayonet apposition), provided alignment is maintained.

Indications for Operative Treatment
According to Weber et al. and Nielson and Simonsen, operative treatment for middle-third fractures is indicated in the following scenarios:
1. Open fractures requiring surgical débridement.
2. Older children (approaching skeletal maturity) where remodeling potential is exhausted. Fuller and McCullough noted that gross malunion does not correct in girls older than 8 years or boys older than 10 years.
3. Irreducible fractures due to soft-tissue interposition.
4. Multiple refractures occurring within a short timeframe.
5. Failed closed reduction after multiple attempts.

SURGICAL TECHNIQUES FOR DIAPHYSEAL FRACTURES
When operative intervention is mandated, the surgeon must choose between Elastic Stable Intramedullary Nailing (ESIN) and Plate Osteosynthesis.
1. Plate Osteosynthesis
Compression plating is highly effective, particularly in older adolescents with adult-type fracture patterns or in cases of malunion requiring osteotomy. Vainionpää et al. and Bhaskar and Roberts demonstrated excellent results with 3.5mm LC-DCP (Limited Contact Dynamic Compression Plates) or one-third tubular plates.
Surgical Warning: A compression plate must never cross an open physis, even in an older child nearing maturity, to prevent catastrophic growth arrest.
Technique Overview:
* Radius Approach: The volar Henry approach is preferred for middle and distal third fractures, utilizing the internervous plane between the brachioradialis (radial nerve) and flexor carpi radialis (median nerve). The dorsal Thompson approach can be used for proximal fractures.
* Ulna Approach: A direct subcutaneous approach along the subcutaneous border of the ulna.
* Fixation: Anatomical reduction is achieved. A minimum of three bicortical screws (six cortices) should be placed on each side of the fracture.
* Single Bone Plating: Bhaskar and Roberts noted that if plating the ulna alone restores acceptable alignment and stability to the radius, radial plating may be avoided to minimize surgical morbidity.

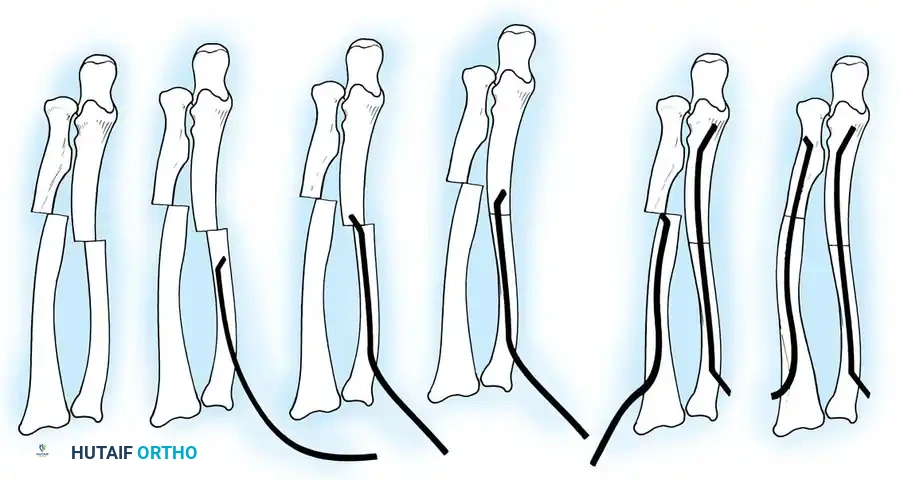
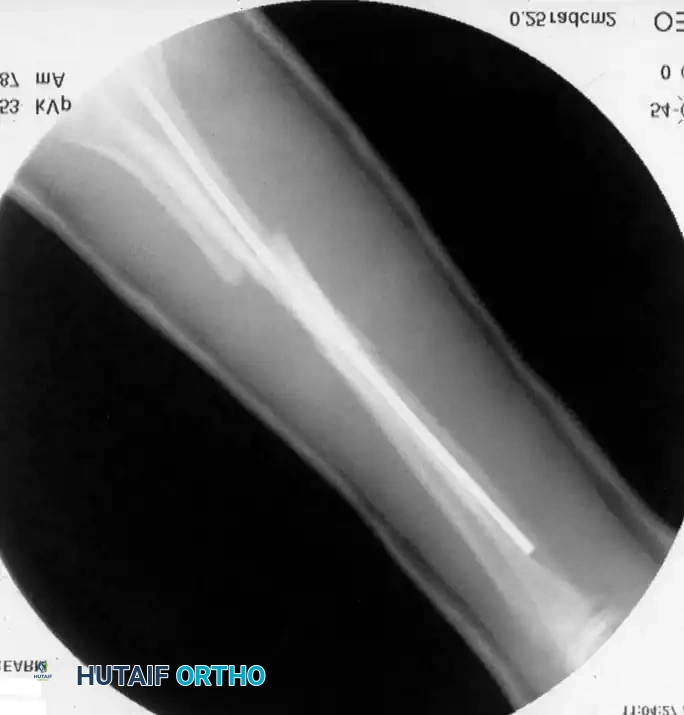
2. Elastic Stable Intramedullary Nailing (ESIN)
ESIN has become the gold standard for displaced, unstable pediatric forearm fractures. Lascombes et al. and Flynn and Waters popularized this technique, citing minimal soft-tissue dissection, preservation of the fracture hematoma, and the ability to achieve three-point biomechanical fixation.
Preoperative Planning:
Nail diameter should be approximately 40% of the narrowest intramedullary canal diameter. Titanium elastic nails (TENs) are preferred for their modulus of elasticity.
Step-by-Step Surgical Technique:
1. Positioning: The patient is placed supine with the arm extended on a radiolucent hand table. Fluoroscopy is positioned perpendicular to the arm.
2. Ulnar Nailing:
* An incision is made over the lateral aspect of the proximal ulna, 1-2 cm distal to the olecranon apophysis.
* The cortex is breached with an awl or drill.
* The pre-bent nail (contoured to create a bow that will tension against the inner cortices) is advanced antegrade down the ulnar shaft to the fracture site.
3. Radial Nailing:
* An incision is made laterally over the distal radius metaphysis, carefully avoiding the superficial branch of the radial nerve and the physis.
* The entry point is created, and the pre-bent nail is advanced retrograde.
4. Fracture Reduction and Nail Passage:
* Closed reduction is performed. The nails are advanced across the fracture sites under fluoroscopic guidance.
* If closed reduction is impossible due to interposition (often seen when initial translation exceeds 100%), a mini-open incision (1-2 cm) is made directly over the fracture to clear the soft tissue.
5. Final Seating: The nails are advanced to the opposite metaphyses. The trailing ends are cut, leaving 1-2 cm outside the bone but buried beneath the skin to facilitate future removal.
Single vs. Double Bone Fixation:
Myers et al. recommended percutaneously fixing the most displaced bone first. If clinical and fluoroscopic examination through a full range of pronosupination demonstrates stability, the second bone may be managed in a cast without internal fixation. However, most surgeons prefer fixing both bones to prevent late displacement.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Postoperative Care
Following ESIN or plating, the arm is typically placed in a well-padded long-arm splint or bivalved cast to accommodate swelling.
* Plating: Early active range of motion can begin once soft tissues heal (1-2 weeks), though a removable splint is often used for protection for 4-6 weeks.
* ESIN: A long-arm cast is usually maintained for 4 to 6 weeks until radiographic bridging callus is visible. Hardware removal for ESIN is routinely performed at 6 to 9 months post-operatively to prevent tendon irritation or skin ulceration over the buried nail ends.

Complications
While outcomes are generally excellent, complications can occur:
1. Compartment Syndrome: Yuan et al. evaluated the incidence of compartment syndrome in pediatric forearm fractures. High-energy crush injuries, open fractures, and prolonged surgical times increase the risk. A high index of suspicion and low threshold for fasciotomy are required.
2. Hardware Complications (ESIN): Shoemaker et al. reported complications including skin ulceration over buried wires, pin-site infections, and loss of reduction after premature wire removal. Nails must be cut short enough to avoid skin tenting but long enough to allow easy retrieval.
3. Neurologic Injury: Transient anterior interosseous nerve (AIN) palsy or superficial radial nerve irritation can occur, particularly during the distal radial approach for ESIN. Meticulous blunt dissection is mandatory.
4. Refracture: Occurs in up to 5% of cases, often after premature hardware removal or inadequate initial immobilization.
5. Radioulnar Synostosis: A rare but devastating complication, more common when both bones are fractured at the same level, or when a single incision is used to approach both bones (which should be strictly avoided).
CONCLUSION
The management of pediatric forearm fractures requires a nuanced approach balancing the incredible remodeling potential of the growing skeleton with the biomechanical demands of the forearm axis. While closed reduction and casting remain the cornerstone of treatment, the strategic application of operative techniques—particularly Elastic Stable Intramedullary Nailing (ESIN)—provides a safe, effective, and minimally invasive solution for unstable or irreducible fractures. By adhering to strict biomechanical principles and respecting the soft-tissue envelope, orthopedic surgeons can consistently achieve excellent functional outcomes and minimize the risk of long-term deformity.
📚 Medical References
- pediatric forearm fractures, J Pediatr Orthop 25:51, 2005.
- Aminian A, Schoenecker PL: Premature closure of the distal radial physis after fracture of the distal radial metaphysis, J Pediatr Orthop 15:395, 1995.
- Bado JL: The Monteggia lesion, Springfi eld, Ill, 1962, Charles C Thomas. Bado JL: The Monteggia lesion, Clin Orthop Relat Res 50:71, 1967.
- Barquet A, Caresani J: Fracture of the shaft of ulna and radius with associated dislocation of the radial head, Injury 12:471, 1980.
- Bell Tawse AJ: The treatment of malunited anterior
You Might Also Like


