

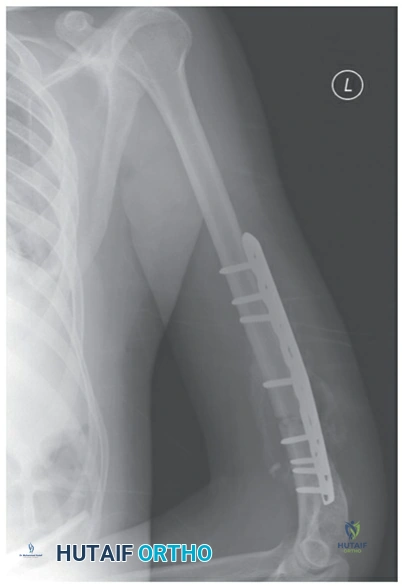
Good morning, candidate. You are presented with a 35-year-old male patient who reports left arm pain after slipping and falling on a flexed elbow at work. Please interpret the provided X-ray image. Describe your findings and classify the type of fracture shown.

Candidate: "The radiograph shows a displaced, comminuted mid-shaft fracture of the left humerus. There is no evidence of articular involvement at the shoulder or elbow. I would classify this as a mid-diaphyseal humeral shaft fracture."
Jumping immediately to treatment plans ("I'd put him in a brace") before describing the injury. Failing to comment on the joints above and below (shoulder/elbow) is a critical omission in an FRCS-level examination.
Systematically address the: (1) View (AP/Lateral), (2) Bone (Humerus), (3) Location (Mid-diaphyseal), (4) Fracture pattern (Transverse/Oblique/Comminuted), (5) Displacement/Angulation, and (6) Joint integrity. Mention that "I have excluded articular extension at the shoulder and elbow joints."
This patient has an associated radial nerve palsy at initial presentation. What is the incidence of this complication in closed fractures, and what is your immediate management strategy?
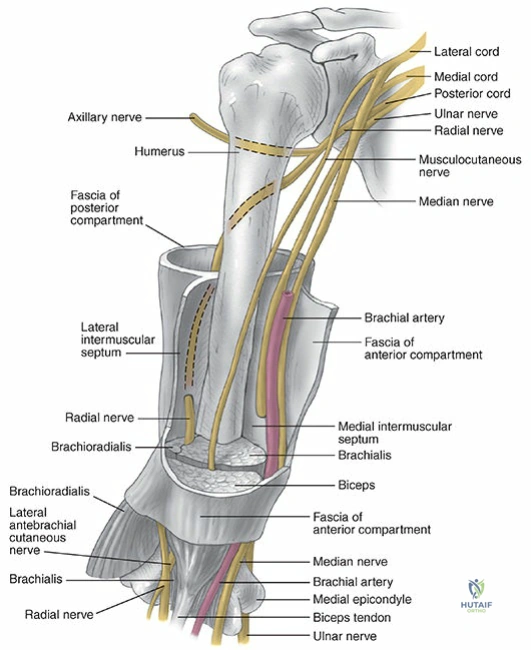
Candidate: "The incidence of radial nerve palsy in closed humeral shaft fractures is 8-15%. Since this is a closed injury, the vast majority are neurapraxias. I would manage this nonoperatively with a functional brace, monitor serial neuro exams, and consider EMG studies at 6-8 weeks if no recovery is seen."
Suggesting immediate surgical exploration. At the FRCS level, examiners expect you to know that primary radial nerve palsy in a closed fracture has a very high rate of spontaneous recovery and is not an indication for immediate surgery.
State the 8-15% incidence, acknowledge the high recovery rate (90%+), and define the 'observation' strategy. Correctly note that surgical exploration is only required for: 1) Open fractures, 2) Vascular injury, or 3) No clinical/EMG recovery after 3-6 months.
Suppose you opt for operative management. Compare the indications for plate fixation versus intramedullary nailing in these fractures.
Candidate: "Plating is generally considered the gold standard for most humeral shaft fractures as it allows for rigid fixation and avoids shoulder morbidity associated with nailing. Nailing is reserved for specific cases such as pathologic fractures, segmental fractures, or patients with poor bone quality where plate screws might not hold."
Failing to mention the shoulder pain associated with antegrade nailing (rotator cuff injury) or failing to recognize that nailing is superior in specific 'host' conditions like osteoporotic bone or bone tumors.
Structure the answer by: (1) Plating as the standard for anatomical reduction/compression, (2) Nailing as a load-sharing device for specific indications (pathologic, segmental, osteoporotic), and (3) Acknowledge the 'Nailing vs. Plating' literature regarding shoulder morbidity.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-md-oral-examination-diagnosis-and-management-of-humeral-shaft-fractures