Midshaft Humerus Fractures: Epidemiology, Surgical Anatomy, Biomechanics & Management
Key Takeaway
Midshaft humerus fractures are managed based on fracture characteristics and patient factors. Non-operative care with functional bracing is common for stable fractures. Operative fixation (plates or nails) is reserved for open fractures, vascular injury, specific nerve compromise, or failure of conservative treatment, aiming to restore alignment and function.
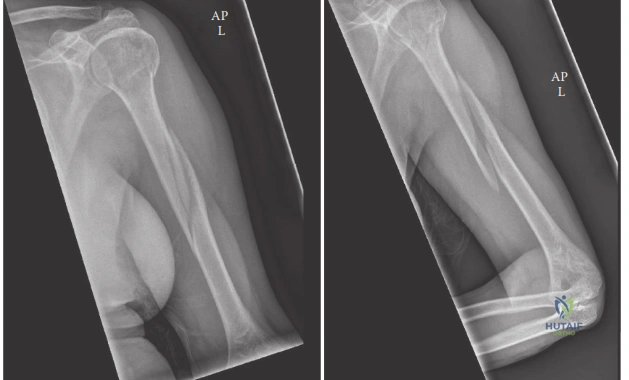
A 35-year-old male presents to the Emergency Department following a high-energy motorcycle collision. He has an obvious deformity of the right mid-humerus. On examination, he has a complete wrist drop and absent sensation over the first dorsal web space. Radiographs confirm a displaced, comminuted midshaft humerus fracture. How do you approach the management of this specific radial nerve injury?
Candidate: I would document the neurological deficit thoroughly and inform the patient that most radial nerve palsies associated with closed humerus fractures are neuropraxic. I would manage the fracture according to standard indications—likely ORIF given the comminution—and observe the nerve post-operatively. If it doesn't recover by 3 months, I would consider an EMG/NCS and potentially exploration.
Failing to distinguish between "primary" (pre-operative) and "secondary" (post-operative/iatrogenic) palsy. A failing candidate often treats all radial nerve palsies the same, forgetting that a newly developed palsy following surgery warrants immediate exploration to rule out entrapment or transection, whereas a primary closed palsy is managed expectantly.
Structure the answer by injury status: 1. Primary (Pre-op) Palsy: In a closed fracture, this is usually a neuropraxia. Manage the fracture based on orthopaedic indications (likely ORIF here due to comminution). Explore the nerve only at the time of planned internal fixation. 2. Expectant Management: Follow clinically; if no recovery by 3-6 months, perform nerve conduction studies/EMG. 3. Secondary (Post-op) Palsy: This is a surgical emergency; immediate exploration is required to rule out iatrogenic injury (entrapment or laceration). 4. Open Fracture: If the fracture is open with nerve palsy, early exploration and nerve repair/grafting may be indicated.
You have decided to proceed with open reduction and internal fixation (ORIF) for the comminuted midshaft humerus fracture. Please describe your approach to the radial nerve and the logic behind your plate placement.
Candidate: I would perform a posterior approach. I'd split the triceps, identify the radial nerve in the spiral groove, and protect it. I would then place the plate on the posterior aspect of the humerus, using a bridging construct with locking screws to account for the comminution.
Neglecting the "Working Length" concept and failing to mention lateral intermuscular septum proximity. Candidates often forget that the radial nerve is at the highest risk when it pierces the lateral intermuscular septum, which is critical during the distal portion of the posterior approach.
Detail the Posterior Approach (Henry/Triceps splitting): 1. Nerve ID: Systematically identify the nerve between the lateral and long heads of the triceps; isolate it early with a vessel loop. 2. Plate Position: While posterior is common, a posterolateral plate placement is often preferred; it provides better biomechanical purchase and keeps the hardware slightly away from the nerve path as it spirals anteriorly. 3. Bridging Principles: Use a long plate to increase "working length" (the number of empty screw holes over the comminution zone), which decreases strain and promotes secondary healing via callus formation, critical in comminuted patterns.
