Mastering Postoperative Rehabilitation and Complication Management in Orthopaedic Trauma
Key Takeaway
Postoperative rehabilitation in orthopaedic trauma requires a delicate balance between early joint mobilization and the preservation of soft-tissue envelopes. Weight-bearing protocols must be tailored to the biomechanical stability of the fixation construct. Concurrently, surgeons must remain vigilant for devastating complications such as deep surgical site infections, clostridial myonecrosis, and fracture blisters, employing aggressive surgical debridement and targeted antimicrobial therapies to salvage both the limb and the patient's life.
POSTOPERATIVE REHABILITATION IN ORTHOPAEDIC TRAUMA
The rehabilitation of the orthopaedic trauma patient is a highly dynamic process that must begin immediately following surgical stabilization. The overarching goal is the restoration of maximal functional capacity while respecting the biological and biomechanical constraints of the healing fracture and its surrounding soft-tissue envelope.
Early Mobilization and Soft-Tissue Considerations
The paradigm of modern osteosynthesis dictates that adjacent joints should be mobilized as expeditiously as possible to prevent arthrofibrosis, capsular contracture, and cartilage degradation. However, this principle must be carefully weighed against the stability of the soft tissues, particularly in the setting of open fractures or severe degloving injuries (e.g., Morel-Lavallée lesions). In open fractures, the premature or excessive motion of musculotendinous units gliding over irregular fracture surfaces can mechanically irritate the compromised soft tissues, thereby exacerbating local inflammation, delaying angiogenesis, and significantly decreasing the local resistance to bacterial inoculation.
To mitigate these risks while preventing contractures, the strategic incorporation of immobilization devices is paramount. Adjacent joints should be supported with custom-molded splints, dynamic braces, or specialized foot attachments integrated directly into external fixation systems.
Clinical Pearl: When neurological deficits result in the loss of active motor function (e.g., peroneal nerve palsy following a complex tibial plateau fracture), the affected joints must be rigorously splinted in a functional position (neutral dorsiflexion) to prevent rigid equinus contractures that will severely compromise future ambulation.
Physical therapy must be initiated with active and active-assisted range-of-motion (ROM) exercises as soon as the soft-tissue healing trajectory permits. The rehabilitation protocol must be strictly physician-directed but heavily reliant on patient compliance and education.
Biomechanics of Weight-Bearing Progression
Weight-bearing protocols are not arbitrary; they are dictated by the mechanical stability of the fixation construct, the inherent fatigue life of the chosen implant, the fracture pattern, and the systemic physiological condition of the patient. Progression must be meticulously monitored via serial radiographic evaluations to assess callus formation, cortical bridging, and the absence of implant failure.
- Extra-articular Fractures with Intramedullary Fixation: For most diaphyseal fractures stabilized with statically locked intramedullary nails, touch-down weight bearing (TDWB) or flat-foot weight bearing (up to 10-15% of body weight) is permitted immediately. This allows for physiological mechanotransduction and axial micromotion, which stimulates secondary bone healing via enchondral ossification.
- Intra-articular Fractures: Fractures with intra-articular extension (e.g., tibial plateau, pilon, or distal femur fractures) require a vastly different approach. Weight bearing is strictly prohibited for a minimum of 10 to 12 weeks to prevent articular subsidence and catastrophic hardware failure. However, early continuous passive motion (CPM) or active ROM is aggressively encouraged to facilitate cartilage nutrition via synovial fluid diffusion.
Vocational rehabilitation and psychosocial counseling must be initiated early in the postoperative period. Polytrauma patients frequently face profound psychological barriers to recovery; early intervention ensures a more productive and holistic return to society.
MANAGEMENT OF SURGICAL COMPLICATIONS
Despite meticulous surgical technique and adherence to sterile protocols, complications following the surgical treatment of fractures remain a formidable challenge. The surgeon must be prepared to diagnose and aggressively manage these limb- and life-threatening scenarios.
Implant-Related and Deep Space Infections
Postoperative infections occur in approximately 4% to 7% of open femoral and tibial fractures treated with intramedullary nailing. In the realm of external fixation, pin track infections are notoriously common, with reported incidences ranging widely from 0.5% to 42%.
The management of an infected fracture in the presence of orthopaedic hardware represents a complex biomechanical and biological trade-off. The fundamental conflict lies between the necessity of bony stability for fracture healing and the foreign body response elicited by the implant. Bacterial organisms, particularly Staphylococcus aureus and Staphylococcus epidermidis, rapidly adhere to metallic implants, producing a protective glycocalyx biofilm that renders them highly recalcitrant to systemic antibiotic therapy and host immune responses.
Surgical Decision-Making Algorithm for Infected Hardware:
1. Unstable Fixation: If the implant is loose or failing to provide absolute or relative stability, it must be removed. An unstable, infected fracture will not heal. The hardware should be extracted, the medullary canal or fracture site radically debrided, and stability restored via an alternative method, most commonly a definitive external fixator.
2. Stable Fixation: If the implant is providing rigid stability and the fracture is not yet united, the implant should generally be retained. Stability is a prerequisite for infection eradication. The patient is subjected to aggressive, serial surgical debridements and targeted intravenous antibiotic therapy (often suppressive) until clinical and radiographic union is achieved.
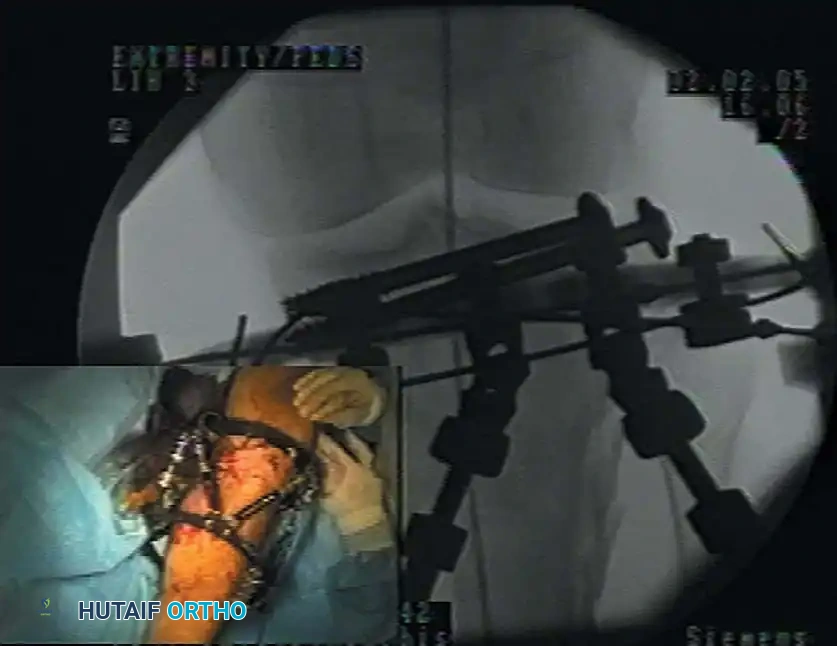
Fig. 50-43 Application of spatial-frame external fixator with use of image intensification. This modality is frequently utilized for the management of infected nonunions following hardware removal.
For infections following the intramedullary nailing of tibial fractures, the contemporary consensus strongly favors leaving the nail in situ until fracture union occurs. Once united, the nail is extracted, and the medullary canal is aggressively reamed and irrigated (often utilizing a Reamer-Irrigator-Aspirator system) to clear the residual nidus of infection.
If a sequestrectomy is required prior to union, exchange nailing is usually necessary. Clinical data from major trauma centers demonstrates that debridement, irrigation, and nail retention until union—followed by subsequent removal and canal brushing—yields exceptionally high rates of both fracture union and infection eradication.

Radiographic evaluation of an intramedullary nail in situ. In the setting of deep infection, stable nails are retained until union, whereas loose nails require immediate exchange or conversion to external fixation.
Surgical Warning: When revising fixation to achieve stability in an infected field, exchange nailing (if the canal permits and soft tissues are adequate) is often preferable to external fixation, as it significantly accelerates the timeline to fracture union and avoids the high morbidity associated with prolonged external fixator wear.
Clostridial Myonecrosis (Gas Gangrene)
Gas gangrene is a catastrophic, rapidly progressive necrotizing soft-tissue infection primarily caused by the Clostridium species of anaerobic, spore-forming, gram-positive bacilli. While historically associated with contaminated battlefield wounds, it remains a critical threat in civilian trauma, particularly in severe open fractures, crush injuries, and agricultural accidents.
Clostridium perfringens is responsible for approximately 90% of gas gangrene cases. The pathogenesis is driven by the production of potent exotoxins, most notably the alpha toxin (lecithinase C). This toxin is profoundly hemolytic, destroying platelets and polymorphonuclear leukocytes, and causing widespread capillary endothelial damage. This results in a vicious cycle of microvascular thrombosis, profound tissue ischemia, and an expanding anaerobic environment that facilitates further bacterial proliferation.
Clinical Presentation and Diagnosis:
The hallmark of clostridial myonecrosis is the sudden onset of excruciating pain that is entirely out of proportion to the visible physical findings. Unlike spreading cellulitis, the pain is initially localized to the infected region but advances rapidly as the myonecrosis spreads—sometimes at an astonishing rate of 10 cm per hour.
Systemic toxicity develops precipitously. The patient will exhibit unexplained tachycardia, diaphoresis, anxiety, and impending delirium. Interestingly, high fever is often absent early in the course. The overlying skin is initially tense, white, and cooler than normal due to underlying ischemia, rapidly progressing to a dark red, purple, or bronze discoloration with the formation of hemorrhagic bullae. Crepitus (gas in the soft tissues) may be palpable but is a late and inconsistent finding.

Fig. 50-44 Gas gangrene presenting with severe soft-tissue necrosis, requiring emergent radical debridement and fasciotomy.
Pitfall: Do not delay surgical intervention to obtain advanced imaging (CT or MRI) if gas gangrene is clinically suspected. The diagnosis is clinical, and any delay in surgical extirpation dramatically increases mortality.
Surgical and Medical Management:
1. Emergent Radical Debridement: The cornerstone of survival is the immediate, aggressive surgical excision of all necrotic, damaged, and infected tissue. Muscle viability must be assessed using the "4 C's": Color, Consistency, Contractility, and Capacity to bleed.
2. Fasciotomy and Amputation: Therapeutic fasciotomies are routinely required to decompress secondary compartment syndromes. In rapidly advancing cases, guillotine amputation of the affected extremity is a life-saving necessity to halt the systemic release of lethal toxins.
3. Antimicrobial Therapy: High-dose intravenous Penicillin G remains highly effective against Clostridium species. However, because these are frequently polymicrobial infections, empiric broad-spectrum coverage must be initiated immediately (e.g., Penicillin G combined with Clindamycin, which halts bacterial toxin synthesis, plus a broad-spectrum agent like Piperacillin-Tazobactam or Vancomycin).
4. Hyperbaric Oxygen (HBO) Therapy: HBO is a controversial but potentially valuable adjunct. By elevating tissue oxygen tension to 3 atmospheres (atm), alpha toxin production is halted, and the demarcation of viable versus necrotic tissue may be improved, potentially allowing for more conservative debridement. However, HBO must never delay the primary surgical debridement.
Tetanus Prophylaxis
Due to robust global vaccination initiatives, Clostridium tetani infections are rare in developed nations. However, when clinical tetanus occurs, the mortality rate approaches 60%. The disease is mediated by tetanospasmin, a neurotoxin that blocks the release of inhibitory neurotransmitters (GABA and glycine) in the central nervous system, leading to severe, uncontrolled muscle spasms and autonomic instability.
The American College of Surgeons (ATLS guidelines) strictly defines tetanus-prone wounds as those exhibiting any of the following characteristics:
* Wounds older than 6 hours prior to medical evaluation.
* Stellate, avulsion, or severe abrasion configurations.
* Depth greater than 1 cm.
* Mechanism involving high-velocity missiles, crush injuries, burns, or frostbite.
* Presence of devitalized, denervated, or ischemic tissue.
* Gross contamination with soil, feces, dirt, or saliva.
Prophylaxis Protocol:
* Previously Immunized Patients: Require only a tetanus toxoid booster if it has been more than 5 years since their last dose (for tetanus-prone wounds) or 10 years (for clean wounds).
* Unimmunized or Unknown Status: Require immediate passive immunization with Human Tetanus Immune Globulin (TIG) at a dose of 250 Units, administered intramuscularly. Concurrently, an active immunization series with tetanus toxoid must be initiated.
* Crucial Technique: TIG and the tetanus toxoid must be administered using separate syringes and injected into separate anatomical sites to prevent the neutralization of the toxoid by the immune globulin.
Soft-Tissue Complications: Fracture Blisters
Fracture blisters are a frequent complication of high-energy trauma, particularly in regions with minimal subcutaneous fat and restricted skin mobility, such as the ankle, calcaneus, tibial plafond, and elbow. They represent a localized separation at the dermo-epidermal junction secondary to profound post-traumatic edema and elevated interstitial pressures.

Fracture blisters presenting on the medial aspect of the ankle following high-energy trauma. Note the distinction between clear fluid-filled and hemorrhagic variants.
Fracture blisters are clinically categorized into two distinct types:
1. Clear Blisters: These contain a transudate fluid. The underlying dermis remains intact and viable. While they indicate severe soft-tissue compromise, they are less prone to deep infection and may tolerate carefully planned surgical incisions once the swelling subsides.
2. Bloody (Hemorrhagic) Blisters: These represent a deeper injury, signifying complete disruption of the dermal vascular plexus. They are essentially equivalent to deep second-degree burns. Surgical incisions directly through bloody blisters carry an unacceptably high risk of wound dehiscence and deep infection and must be strictly avoided.
Management Protocol:
The definitive surgical fixation of the underlying fracture must be delayed until the soft-tissue envelope recovers. The limb should be strictly elevated and immobilized (often via a spanning external fixator).
We advocate treating ruptured or unroofed fracture blisters with a burn-care protocol. This involves sterile surgical excision of the necrotic epidermal roof, followed by the daily application of Silver Sulfadiazine (Silvadene) ointment and non-adherent dressings. This promotes rapid re-epithelialization (typically within 5 to 10 days) and minimizes superficial bacterial colonization.
The "Wrinkle Test": The optimal timing for definitive internal fixation is determined by the return of skin pliability. Surgery should be delayed until the skin over the surgical site exhibits fine wrinkling upon manual compression or dependency, indicating that the interstitial edema has sufficiently resolved to allow for tension-free wound closure.
Thromboembolic Complications
Polytrauma patients are at an exceptionally high risk for deep vein thrombosis (DVT) and subsequent pulmonary embolism (PE). The physiological stress of trauma perfectly fulfills Virchow's Triad: endothelial injury (from the fracture and surgery), venous stasis (from immobilization), and hypercoagulability (the systemic acute phase response to trauma).
Research indicates that polytrauma patients with major lower extremity or pelvic fractures who are immobilized for 10 days or more face a DVT incidence approaching 67% if left unprophylaxed. While fatal PE is relatively rare, non-fatal embolic events severely complicate the patient's cardiopulmonary recovery.
The challenge in orthopaedic trauma is balancing the necessity of chemical thromboprophylaxis (e.g., Low Molecular Weight Heparin) against the risk of catastrophic postoperative hemorrhage, particularly in the setting of pelvic ring injuries, spinal trauma, or evolving compartment syndromes. Mechanical prophylaxis (sequential compression devices) should be instituted immediately, with chemical prophylaxis initiated as soon as the hemorrhagic risk is deemed acceptable by the surgical team.
You Might Also Like


