Surgical Restoration of Pinch and Thumb Opposition
Key Takeaway
Restoration of thumb opposition is critical for functional pinch, often compromised by median nerve palsy or poliomyelitis. Successful opponensplasty requires a supple carpometacarpal joint, meticulous selection of an expendable donor motor such as the flexor digitorum superficialis, and precise biomechanical routing. This guide details the fundamental principles of tendon excursion, pulley construction, and step-by-step surgical techniques to restore dynamic thumb opposition and maximize hand function.
RESTORATION OF PINCH AND THUMB OPPOSITION
The evolutionary hallmark of the human hand is the opposable thumb, a biomechanical marvel that enables both powerful grasp and precise pinch. The loss of thumb opposition—frequently secondary to median nerve palsy, poliomyelitis, severe brachial plexus trauma, or advanced peripheral neuropathies (such as Charcot-Marie-Tooth disease)—devastates global hand function. Without opposition, the hand is relegated to a primitive, non-prehensile state, severely limiting the patient's independence and occupational capacity.
The surgical restoration of pinch, commonly referred to as opponensplasty, is a highly nuanced procedure. It demands a profound understanding of hand biomechanics, precise preoperative evaluation, and meticulous surgical execution. This comprehensive guide details the foundational principles, donor muscle selection, and operative techniques required to successfully restore thumb opposition.
BIOMECHANICS OF THUMB OPPOSITION
Opposition is not a simple, single-plane movement; rather, it is a complex, triplanar motion that positions the thumb pad directly opposite the pads of the other digits.
The Triplanar Motion
Opposition is achieved through the coordinated execution of three distinct movements:
1. Abduction: Elevating the thumb away from the palmar surface of the index finger.
2. Flexion: Sweeping the thumb across the palm toward the ulnar digits.
3. Pronation: Rotating the first metacarpal and proximal phalanx along their longitudinal axes to face the fingers.
Muscular Contributions
Normal opposition depends primarily on the function of the thenar intrinsic muscles innervated by the recurrent motor branch of the median nerve:
* Abductor Pollicis Brevis (APB): The primary driver of palmar abduction and pronation.
* Opponens Pollicis (OP): Acts on the first metacarpal to flex and pronate the carpometacarpal (CMC) joint.
* Flexor Pollicis Brevis (FPB): Contributes to flexion and pronation (superficial head via median nerve, deep head via ulnar nerve).
Clinical Pearl: The abductor pollicis brevis is the most critical intrinsic muscle for opposition. Any tendon transfer designed to restore pinch must replicate the vector and function of the APB.
Furthermore, extrinsic muscles are absolutely necessary to dynamically stabilize the thumb metacarpophalangeal (MCP) and interphalangeal (IP) joints during pinch. If these joints lack dynamic stability due to concurrent paralysis, they must be stabilized surgically via arthrodesis or tenodesis to prevent collapse under the load of the transferred tendon.
PREOPERATIVE PREREQUISITES
Before any tendon transfer is considered, the surgeon must ensure that the hand meets strict biomechanical prerequisites. Failure to address these will result in a failed opponensplasty.
- A Supple Carpometacarpal (CMC) Joint: The thumb CMC joint must be freely movable. A tendon transfer cannot overcome a stiff joint or a contracted first web space. If a fixed adduction contracture exists, it must be released preoperatively or concomitantly via a Z-plasty of the web space, release of the adductor pollicis origin, or capsulotomy.
- Joint Stability: The MCP and IP joints must be stable. If a fixed flexion contracture or severe instability is present, arthrodesis (typically in 15 to 20 degrees of flexion for the MCP joint) is indicated.
- Adequate Donor Motor: The selected donor muscle must be expendable, healthy, and possess a Medical Research Council (MRC) grade of 5/5. A transferred muscle typically loses one full grade of strength postoperatively.
PRINCIPLES OF TENDON TRANSFER FOR OPPOSITION
The success of an opponensplasty relies on matching the biomechanical properties of the donor muscle to the requirements of the paralyzed thumb intrinsics. The pioneering work of Curtis (1974) established the fundamental principles of tendon amplitude, excursion, and muscle power.
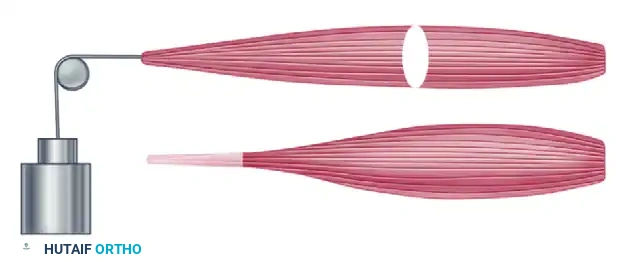
Amplitude and Excursion
The amplitude (excursion) of the donor tendon must closely match the physiological requirements of thumb opposition.
Table 71-1: Amplitude of Excursion (Adapted from Curtis RM, 1974)
* Wrist tendons: 33 mm
* Flexor digitorum profundus (FDP): 70 mm
* Flexor digitorum sublimis/superficialis (FDS): 64 mm
* Extensor digitorum communis (EDC): 50 mm
* Flexor pollicis longus (FPL): 52 mm
* Extensor pollicis longus (EPL): 58 mm
* Extensor pollicis brevis (EPB): 28 mm
* Abductor pollicis longus (APL): 28 mm
Muscle Power and Work Capacity
The working capacity of a muscle is defined by the equation:
W = F × d
Where:
* W = Working capacity (meter-kilograms)
* F = Absolute muscle power (Force), calculated as 3.65 × cm² of the physiological cross-section.
* d = Distance (amplitude or displacement).
When selecting a motor, the surgeon must evaluate the strength of available units. The donor must have sufficient cross-sectional area to generate the force required for a strong pinch against the index and middle fingers.
Direction of Pull and Pulley Systems
To replicate the function of the APB, the transferred tendon must approach the thumb from the ulnar side of the wrist or palm. Specifically, the ideal vector originates near the pisiform bone. Because most donor tendons do not naturally follow this path, a pulley system is often required.
- Static Pulley: Created by making a loop at the distal end of the flexor carpi ulnaris (FCU) tendon or utilizing the transverse carpal ligament.
- Dynamic Pulley: Formed by looping the transfer around the intact, functioning FCU tendon.
Surgical Warning: The pulley must be robust. If the pulley fails or stretches postoperatively, the vector of pull will migrate radially, resulting in palmar abduction without the critical pronation required for true opposition.
SELECTION OF DONOR MOTORS
The selection of an appropriate motor is dictated by the pattern of paralysis and the availability of healthy, expendable muscles.
1. Flexor Digitorum Superficialis (FDS)
The FDS of the ring finger is the gold standard and muscle of choice for restoring opposition (the Riordan or Royle-Thompson transfer). It possesses excellent excursion (64 mm), adequate power, and an in-phase firing pattern for grasp and pinch.

Prerequisite: The associated flexor digitorum profundus (FDP) of the ring finger must be strong enough to flex the digit independently. If the ring FDS is unsuitable, the FDS of the middle finger is the second choice.
2. Extensor Indicis Proprius (EIP)
If the flexor tendons are unsuitable (e.g., in high median nerve palsy where FDS is paralyzed), the EIP is an excellent alternative (the Burkhalter transfer). It does not require a tendon graft, as it is long enough to reach the thumb when routed through the interosseous membrane or around the ulnar border of the wrist.
3. Alternative Motors Requiring Tendon Grafts
If neither the FDS nor the EIP is available, other muscles can be utilized, though they universally require a free tendon graft (e.g., palmaris longus or plantaris) to reach the thumb insertion:
* Extensor Carpi Ulnaris (ECU)
* Extensor Carpi Radialis Longus (ECRL): A wrist extensor should only be transferred if the other wrist extensors (ECRB) are strong and have not been transferred elsewhere.
* Palmaris Longus (PL): Often used in the Camitz transfer for severe carpal tunnel syndrome, though it primarily restores abduction rather than true opposition due to its radial vector.
SURGICAL TECHNIQUE: THE RIORDAN TRANSFER
The Riordan transfer utilizes the FDS of the ring finger, routed around an FCU pulley, to restore opposition. It is highly reliable for isolated median nerve palsy.
Step 1: Harvest of the FDS Tendon
- Make a transverse incision at the proximal flexion crease of the ring finger.
- Identify the FDS tendon. To maximize length, divide the two slips of the FDS just proximal to their insertion on the middle phalanx, taking care not to damage the underlying FDP tendon or the vincula.
- Make a second incision in the distal volar forearm, proximal to the wrist crease.
- Identify the FDS to the ring finger in the forearm and withdraw it from the carpal tunnel into the forearm wound.
Step 2: Construction of the Pulley
To achieve the correct vector (pulling toward the pisiform), a pulley is constructed using the FCU.

- Identify the FCU tendon near its insertion into the pisiform.
- Split the radial half of the FCU tendon longitudinally for approximately 3 to 4 cm.
- Detach this radial half proximally, leaving it attached distally at the pisiform.
- Loop the detached slip back upon itself to create a ring, and suture it securely to the intact ulnar half of the FCU. This creates a static, unyielding pulley directly over the pisiform.
Step 3: Tendon Routing
- Make a longitudinal or curved incision over the radial aspect of the thumb MCP joint, exposing the insertion of the APB and the EPL tendon over the proximal phalanx.
- Create a subcutaneous tunnel from the thumb MCP joint incision, across the palm, to the forearm incision.
- Pass the harvested FDS tendon through the constructed FCU pulley.
- Route the FDS tendon through the subcutaneous tunnel to the thumb. The tunnel must be superficial to the palmar fascia to prevent bowstringing and ensure a straight line of pull.
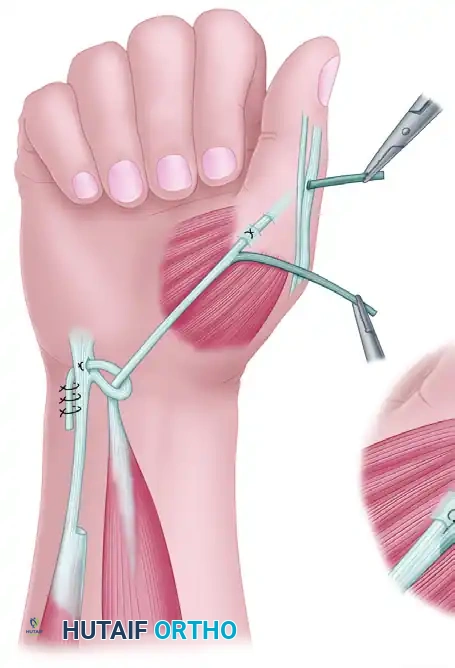
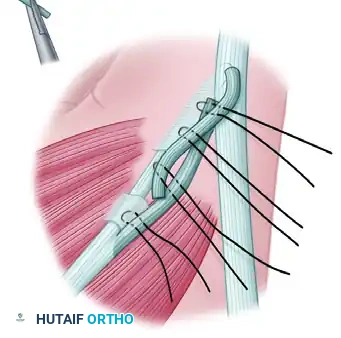
Step 4: Insertion and Fixation
The insertion technique is critical for restoring both abduction and pronation. Riordan advocated a dual insertion to maximize the pronation effect.
- Pass the FDS tendon through the substance of the paralyzed APB tendon/muscle belly.
- Route the distal end of the FDS tendon dorsally over the proximal phalanx to interweave with the Extensor Pollicis Longus (EPL) tendon.
- Tensioning: Position the wrist in neutral, the thumb in maximum palmar abduction, and full opposition (touching the ring finger).
- Suture the transfer to the APB insertion and the EPL tendon under appropriate tension using non-absorbable braided sutures (e.g., 3-0 or 4-0 polyester).
Pitfall: Over-tensioning is a common error. While the transfer should be snug, excessive tension can lead to a fixed flexion contracture of the thumb MCP joint or limit the ability to flatten the hand. Conversely, under-tensioning will fail to provide adequate pinch strength.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of an opponensplasty is heavily dependent on meticulous postoperative care and specialized hand therapy.
Phase 1: Immobilization (Weeks 0-3)
- Immediately postoperatively, the hand is immobilized in a custom thermoplastic splint or a well-padded fiberglass thumb spica cast.
- Positioning: The wrist is placed in 10 to 15 degrees of flexion. The thumb is immobilized in maximum palmar abduction and opposition. The IP joint of the thumb is left free if it was not part of the transfer fixation, though many surgeons prefer to immobilize it in slight flexion to protect the EPL insertion.
- Strict elevation is maintained to minimize edema.
Phase 2: Early Active Motion (Weeks 3-6)
- The cast is removed at 3 to 4 weeks.
- A removable thumb spica splint is fabricated, holding the thumb in opposition.
- Active Range of Motion (AROM): The patient begins active, gravity-eliminated motion. The focus is on activating the transferred muscle (e.g., asking the patient to "flex the ring finger" to initiate thumb opposition if the FDS was used).
- Cortical re-education is critical during this phase. Biofeedback and mirror therapy can be highly effective.
- Passive stretching of the transfer is strictly prohibited.
Phase 3: Strengthening and Weaning (Weeks 6-12)
- At 6 weeks, gentle passive range of motion (PROM) is initiated to resolve any residual stiffness.
- The splint is gradually weaned during the day but maintained at night until 8 weeks.
- Progressive strengthening begins, utilizing putty and pinch gauges.
- Full, unrestricted activity is typically permitted by 10 to 12 weeks, provided that dynamic stability and strength have been achieved.
COMPLICATIONS AND MANAGEMENT
Even in experienced hands, opponensplasty carries potential complications that must be anticipated and managed promptly.
- Pulley Failure: If the FCU pulley stretches or ruptures, the vector of pull shifts radially. The thumb will abduct but fail to pronate, resulting in a weak, side-to-side pinch rather than true opposition. Revision surgery to reconstruct the pulley is required.
- Adduction Contracture: Failure to maintain the first web space during the postoperative phase can lead to a recurrent adduction contracture, negating the mechanical advantage of the transfer. Aggressive splinting and therapy are required; severe cases may necessitate surgical release.
- Swan-Neck Deformity of the Donor Digit: Harvesting the FDS can occasionally lead to a swan-neck deformity in the donor ring finger, particularly in patients with inherent ligamentous laxity. This can be mitigated by leaving a sufficient distal stump of the FDS to prevent PIP joint hyperextension, or by performing a concurrent tenodesis.
- Tendon Rupture or Adhesion: Adhesions along the subcutaneous tunnel can restrict excursion. Meticulous hemostasis, gentle tissue handling, and early active motion (within the constraints of the protocol) minimize this risk. Rupture at the insertion site requires immediate surgical exploration and repair.
CONCLUSION
The restoration of pinch through thumb opponensplasty is a transformative procedure for patients suffering from median nerve palsy or other paralytic conditions. By strictly adhering to the biomechanical principles of tendon excursion, selecting an appropriate donor motor, constructing a rigid ulnar-based pulley, and executing a precise insertion, the orthopedic surgeon can reliably restore dynamic, powerful, and functional thumb opposition.
You Might Also Like

