Surgical Management of Central Slip Ruptures and Boutonnière Deformity
Key Takeaway
The surgical management of central slip ruptures requires a profound understanding of extensor mechanism biomechanics. This comprehensive guide details the operative techniques for both acute injuries and chronic Boutonnière deformities. Key procedures include primary anatomic repair, Fowler/Dolphin tenotomy for supple deformities, and the Littler dorsal shift reconstruction. Precise surgical execution, combined with meticulous postoperative rehabilitation such as the Evans short-arc motion protocol, is essential for restoring proximal interphalangeal joint kinematics and preventing long-term functional impairment.
INTRODUCTION AND PATHOANATOMY
The extensor mechanism of the digit is a highly complex, finely balanced kinematic chain. Disruption of the central slip of the extensor expansion over the proximal interphalangeal (PIP) joint initiates a predictable and debilitating cascade of biomechanical failures, clinically recognized as the Boutonnière (or buttonhole) deformity.
Initially, the loss of central slip continuity results in an extensor lag at the PIP joint. If left untreated, the triangular ligament over the dorsum of the middle phalanx attenuates, allowing the lateral bands to subluxate volar to the axis of rotation of the PIP joint. Once the lateral bands migrate volarward, they transition from being extensors of the PIP joint to paradoxical flexors. Concurrently, the transverse retinacular ligaments contract, tethering the lateral bands in this abnormal volar position. The unopposed pull of the extensor mechanism is then concentrated entirely on the distal interphalangeal (DIP) joint via the terminal tendon, leading to the classic clinical presentation: a fixed flexion contracture of the PIP joint combined with hyperextension of the DIP joint.
Clinical Pearl: The true Boutonnière deformity is rarely present immediately following an acute central slip rupture. It is a progressive deformity that develops over weeks as the secondary stabilizing structures (triangular ligament and transverse retinacular ligaments) fail and contract. Early diagnosis of a central slip injury via the Elson test is paramount to prevent chronic deformity.
PREOPERATIVE EVALUATION AND PREPARATION
Clinical Assessment
Surgical decision-making is dictated by the chronicity of the injury and the suppleness of the joints. In chronic cases, the surgeon must differentiate between a supple deformity (where the PIP joint can be passively extended) and a fixed deformity (where volar capsular contractures and collateral ligament shortening prevent passive extension).
Preoperative Rehabilitation
Before any surgical reconstruction of a chronic Boutonnière deformity is attempted, aggressive hand therapy is mandatory.
- Serial Splinting: Dynamic or static progressive splinting (e.g., Capener splints, serial cylinder casts) must be utilized to stretch the contracted volar structures and restore passive PIP joint extension.
- DIP Joint Flexion Exercises: Active and passive DIP joint flexion exercises are prescribed to stretch the contracted oblique retinacular ligaments (ORL) and lateral bands.
Surgical Warning: Attempting soft-tissue reconstruction on a digit with a fixed PIP flexion contracture is destined for failure. If preoperative splinting fails to achieve full passive PIP extension, a surgical release of the volar plate and collateral ligaments must precede or accompany the extensor mechanism reconstruction.
ACUTE PRIMARY REPAIR OF THE CENTRAL SLIP
Acute lacerations or avulsions of the central slip should be treated with primary anatomic repair.
Surgical Approach and Joint Stabilization
- Incision: Expose the extensor mechanism dorsally utilizing a lazy-S or bayonet incision. Straight dorsal incisions must be strictly avoided to prevent longitudinal scar contracture over the joint.
- Joint Positioning: Place the PIP joint in full, absolute extension.
- Transarticular Fixation: Hold the joint in this extended position by inserting a 0.045-inch Kirschner wire (K-wire) obliquely across the PIP joint. This neutralizes tension on the repair site.
Tendon Repair Techniques
- Mid-substance Lacerations: Repair the disruption of the central slip using a roll stitch of 4-0 monofilament nylon or stainless steel wire. If there is sufficient tendon bulk, utilize a core suture technique, supplemented with a Silfverskiöld cross-stitch to optimize the biomechanical strength of the repair.
- Avulsion Injuries: If there is an insufficient distal tendon stump at the insertion site on the dorsal base of the middle phalanx, utilize a micro-suture anchor. This provides a robust, anatomically precise reattachment of the central slip to the bone.
Postoperative Care for Acute Repairs
- Immobilization: Close the wound and apply a volar splint over a gently compressing dressing. Sutures are removed at 10 to 14 days.
- K-wire Removal: The transarticular K-wire is typically removed at 3 to 4 weeks, followed by gradual, protected flexion. A volar splint is worn to protect the repair for an additional 4 weeks between exercise sessions.
- The Evans Protocol: Evans reported superior functional outcomes in highly compliant patients utilizing an early "short arc" motion protocol. In this regimen, controlled, limited-arc exercises begin 2 to 11 days postoperatively, bypassing the need for transarticular K-wire fixation. This protocol requires meticulous hand therapy supervision and is contraindicated in non-compliant patients or tenuous repairs.
MANAGEMENT OF CHRONIC BUTTONHOLE DEFORMITY
In neglected or chronic cases, the central slip has retracted, the lateral bands have subluxated volarward, and the dorsal transverse retaining fibers have stretched beyond competence. Reconstruction is technically demanding and requires precise rebalancing of the extensor forces.
Supple Deformity: The Fowler/Dolphin Tenotomy
For a chronic Boutonnière deformity where the PIP joint remains fully flexible, a Fowler/Dolphin tenotomy may be indicated.
This procedure involves the targeted release of the lateral bands distal to the central slip insertion. By transecting the extensor mechanism distally, the entire extensor apparatus migrates proximally. This proximal shift reduces the pathological hyperextension tension at the DIP joint and simultaneously increases the extensor tension at the PIP joint, effectively rebalancing the digit.
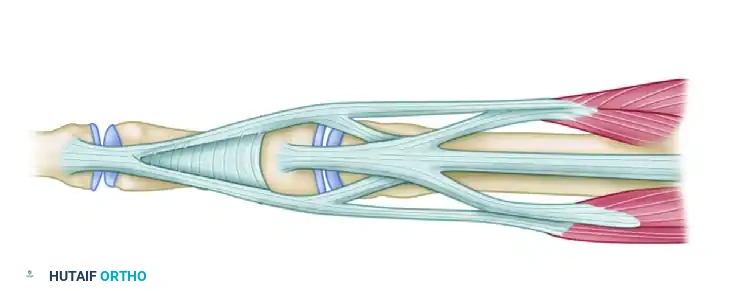
Figure 66-73A: Preoperative biomechanics of the supple buttonhole deformity. The lateral bands are subluxated, causing PIP flexion and DIP hyperextension.
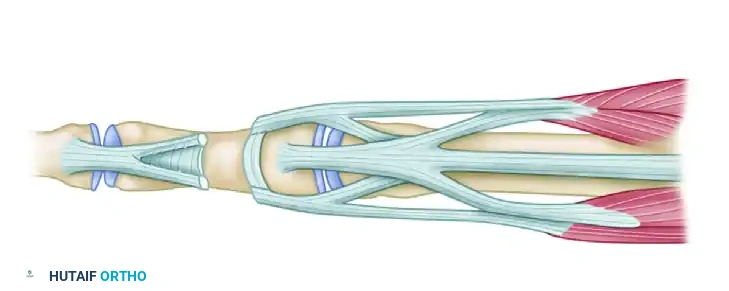
Figure 66-73B: Post-tenotomy biomechanics. The lateral bands are released distal to the insertion of the central slips. The resulting proximal migration of the extensor mechanism reduces tension at the DIP joint and increases extensor tension at the PIP joint.
The Littler Technique (Dorsal Shift of Lateral Bands)
When the central slip is irreparably attenuated, the Littler technique provides an elegant biomechanical reconstruction by recruiting the subluxated lateral bands to recreate the central slip.
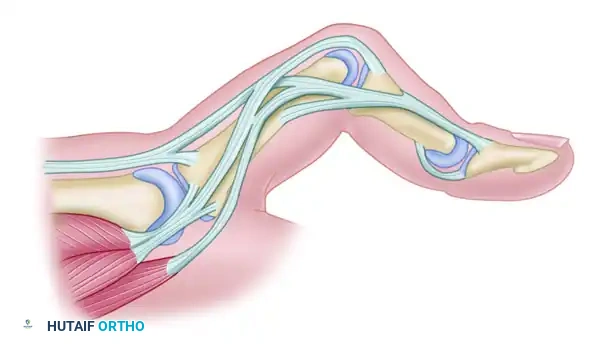
Figure 66-72A: Typical chronic Boutonnière deformity with fixed flexion of the PIP joint and hyperextension of the DIP joint. The lateral bands have subluxated volarward.
Step-by-Step Surgical Technique:
1. Incision: Make a dorsal curved longitudinal incision over the PIP joint to expose the entire extensor apparatus.
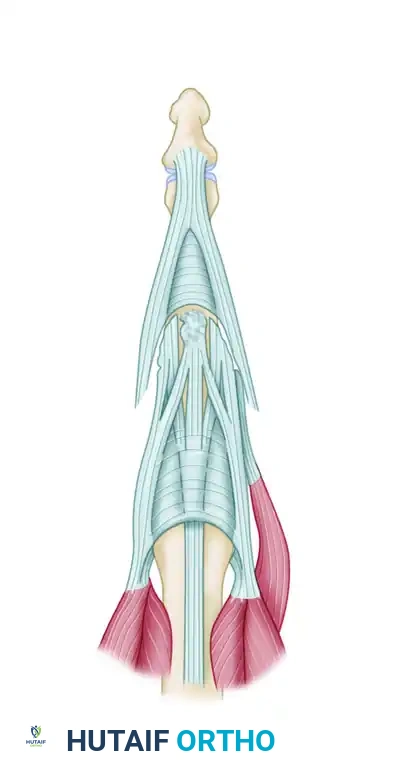
Figure 66-72B: Dorsal curved longitudinal incision.
-
Mobilization of Lateral Bands: Identify the volar-subluxated lateral bands. Carefully free their insertions completely, preserving only the radialmost fibers of the radial lateral band to maintain some active DIP joint extension via the lumbrical contribution.

Figure 66-72C: The insertions of the lateral bands are completely freed except for the radialmost fibers of the radial lateral band. -
Dorsal Relocation: Shift the mobilized lateral bands dorsally and proximally toward the dorsal midline of the PIP joint.
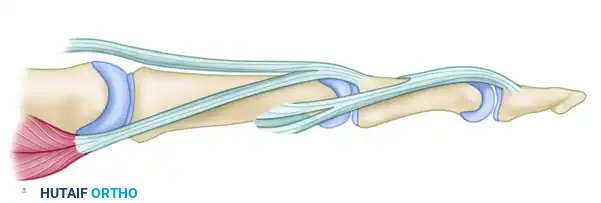
Figure 66-72D: The lateral bands are shifted dorsally and proximally. -
Suture Reconstruction: Suture the relocated lateral bands to each other in the midline. Secure them to the soft tissues over the proximal third of the middle phalanx and to the remnant of the central tendon to recreate a robust central extensor force.
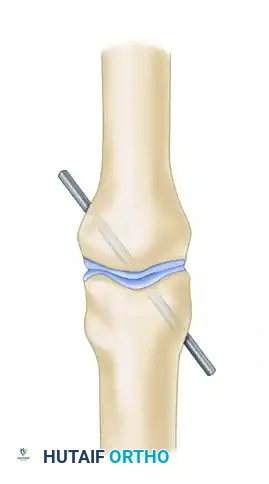
Figure 66-72E: The lateral bands are sutured together and to the central tendon. -
Joint Fixation: Fix the PIP joint in absolute full extension using a transarticular K-wire to protect the reconstruction during the initial healing phase.
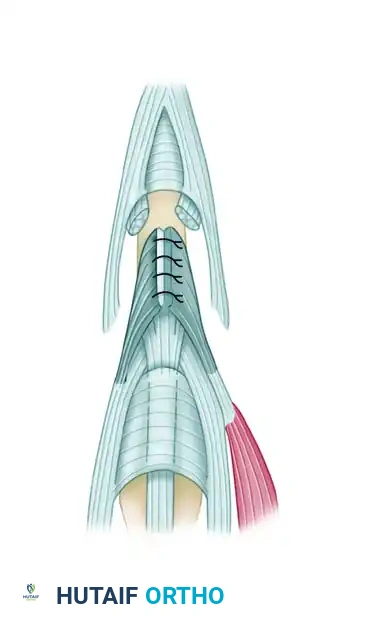
Figure 66-72F: The PIP joint is fixed in full extension by a Kirschner wire. -
Biomechanical Restoration: Following this repair, the PIP joint is extended by the newly reconstructed extensor hood. The DIP joint extension is maintained by the preserved lumbrical muscle and the oblique retinacular ligament.

Figure 66-72G: Cross-sectional biomechanics after repair. The lateral bands are restored dorsal to the PIP axis of rotation.
Alternative Reconstructive Techniques
Depending on the specific pattern of tissue loss and surgeon preference, several other reconstructive options exist for chronic central slip deficiency.
The Snow Technique (Central Slip Flap)
In cases where the central slip is severed but a robust proximal stump remains, a retrograde flap can be utilized.
* A retrograde flap of the proximal central slip is elevated.
* After suturing the severed central slip and lateral bands to restore continuity, the retrograde flap is folded distally over the juncture as a reinforcing batten.
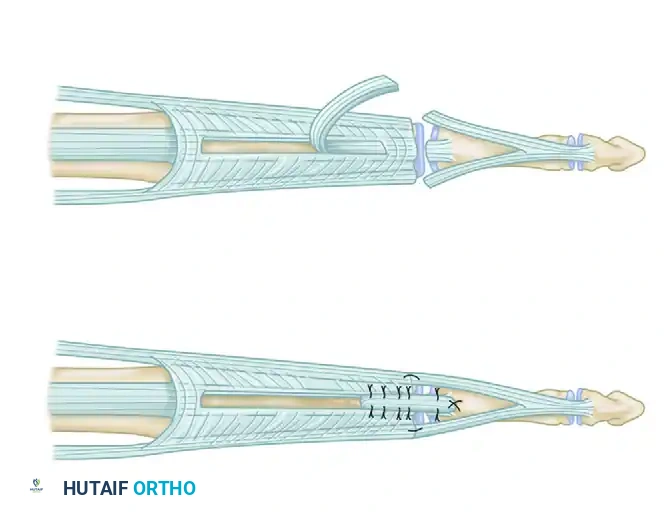
Figure 66-74: Severed extensor mechanism over the PIP joint. A retrograde flap of the central slip has been elevated and brought over the juncture as a batten.
The Aiache Technique (Lateral Band Flaps)
This technique utilizes split portions of the lateral bands to reconstruct the central slip without completely sacrificing their distal insertions.
1. The lateral bands are freed, and the oblique and transverse retinacular ligaments are elevated from the middle phalanx.
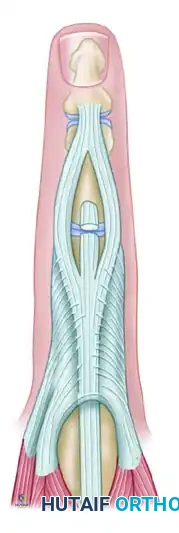
Figure 66-75 (Left): Injury to the middle slip. Lateral bands are freed.
-
Each lateral band is slit longitudinally into two equal parts.
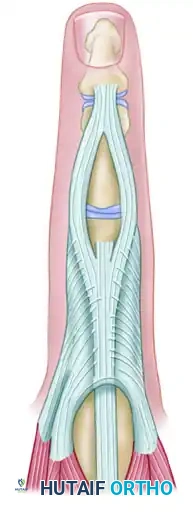
Figure 66-75 (Center): Each lateral band is slit longitudinally. -
The medial halves of the split lateral bands are mobilized dorsally, sutured together in the midline, and secured to the capsule to recreate the central slip insertion.
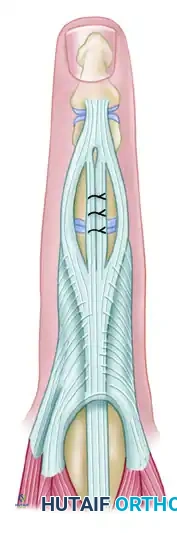
Figure 66-75 (Right): Medial halves of the lateral bands are sutured together and to the capsule in the midline.
Tendon Grafting and Salvage Procedures
- Tendon Grafts: If there is a significant segmental defect in the extensor mechanism that cannot be bridged by local tissue rearrangement, free tendon grafts (e.g., palmaris longus) may be necessary to span the defect.
- Salvage Procedures: In cases of severe, long-standing deformity where the PIP joint has developed significant secondary arthrosis, soft-tissue reconstruction will fail to provide a painless, functional digit. In these scenarios, PIP joint arthrodesis (typically positioned in 30 to 40 degrees of flexion, depending on the digit) or PIP joint arthroplasty (silicone or surface replacement) must be considered as the definitive salvage procedure.
POSTOPERATIVE REHABILITATION AND COMPLICATIONS
The success of extensor mechanism reconstruction is inextricably linked to postoperative rehabilitation. The delicate balance between protecting the repair and preventing joint stiffness requires constant vigilance.
- Immobilization Phase: For complex reconstructions (Littler, Aiache, Snow), the transarticular K-wire is maintained for 3 to 4 weeks.
- Mobilization Phase: Upon pin removal, an active, short-arc motion protocol is initiated. A dynamic extension splint (e.g., Capener) is often utilized between exercise sessions to prevent recurrent extensor lag.
- Complications: The most common complication is a recurrent extensor lag, often due to stretching of the repair or inadequate preoperative correction of volar contractures. Conversely, overly aggressive dorsal tethering can result in a loss of PIP joint flexion. Pin tract infections from the transarticular K-wire must be monitored and treated promptly with oral antibiotics and local pin care.
> Clinical Pearl: Always counsel the patient preoperatively that a "normal" finger is rarely achieved after a chronic Boutonnière reconstruction. The goal is a functional arc of motion, typically accepting a mild residual extensor lag in exchange for functional PIP flexion.
You Might Also Like

