Congenital Hand Reconstruction: Index Finger Recession and Clasped Thumb Management
Key Takeaway
Congenital clasped thumb and thumb hypoplasia present complex reconstructive challenges. Management ranges from serial splinting for isolated extensor deficiencies to comprehensive surgical reconstruction, including index finger recession or pollicization. This guide details the Flatt technique for index metacarpal recession and the Neviaser protocol for clasped thumb, providing step-by-step surgical approaches, biomechanical principles, and evidence-based postoperative rehabilitation protocols for optimal functional outcomes.
INTRODUCTION TO CONGENITAL THUMB ANOMALIES
Congenital anomalies of the thumb, ranging from isolated extensor deficiencies to severe hypoplasia, profoundly impact the functional capacity of the developing hand. The thumb contributes approximately 40% to 50% of overall hand function, primarily through its unique ability to perform opposition, power grasp, and precision pinch. When congenital hypoplasia or a clasped thumb deformity is present, early and precise intervention is paramount to harness neuroplasticity and integrate the reconstructed digit into the child's functional motor patterns.
This comprehensive guide details two critical reconstructive paradigms: the recession of the index finger (Flatt technique) for severe thumb hypoplasia, and the systematic management of the congenital clasped thumb, including tendon transfer techniques and complex soft-tissue reconstructions.
RECESSION OF THE INDEX FINGER (FLATT TECHNIQUE)
In cases of severe thumb hypoplasia or aplasia where the basal joint is absent or non-functional, pollicization of the index finger remains the gold standard. However, in specific anatomical variants where a rudimentary thumb ray exists but lacks adequate length or mobility, or as a modified approach to index transposition, the recession of the index finger (as described by Flatt) provides a biomechanically sound alternative. The goal is to reposition the index metacarpal into a spatial orientation that mimics the native trapeziometacarpal joint, allowing for effective opposition against the ulnar digits.
Biomechanical Principles of Index Recession
To function as a thumb, the index finger must be shortened, rotated, and abducted. The native thumb operates in a plane distinct from the other digits. Therefore, the index metacarpal must undergo a complex three-dimensional spatial realignment:
1. Shortening (Recession): Removing 1.5 to 2.0 cm of the metacarpal shaft equates the length of the new "thumb" to the normal thumb, ensuring the tip aligns appropriately with the proximal interphalangeal joints of the remaining fingers during pinch.
2. Axial Rotation: Pronating the digit 100 to 110 degrees is critical. This rotation positions the volar tactile pads of the index finger directly facing the pads of the middle and ring fingers.
3. Palmar and Radial Abduction: Positioning the digit in 35 degrees of palmar abduction and 20 degrees of radial abduction clears the first web space, allowing for grasping of large objects.
💡 Clinical Pearl: Metacarpal Positioning
The most common error in index recession or pollicization is under-rotation. Ensure a full 100 to 110 degrees of axial rotation. The nail plate of the recessed index finger should sit at a 90-degree angle to the nail plates of the remaining digits when the hand is resting flat.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia is required, supplemented by a regional brachial plexus block for postoperative pain control and vasodilation.
- Positioning: The patient is positioned supine with the operative extremity extended on a radiolucent hand table.
- Equipment: A well-padded pneumatic tourniquet is applied to the upper arm. Loupe magnification (3.5x to 4.5x) and bipolar electrocautery are essential for meticulous neurovascular dissection. Mini-C-arm fluoroscopy must be available.
Surgical Technique: Step-by-Step Approach
-
First Web Space Incision and Dissection:
- Under strict tourniquet control, design a dorsal longitudinal 1-cm incision within the first web space.
- Deepen the incision through the subcutaneous tissues. Meticulously identify and protect the radial digital nerve to the index finger and the proper digital artery.
- Divide the deep transverse metacarpal ligament, the palmar and dorsal fascial bands, and the intertendinous connections (juncturae tendinum) between the index and middle finger metacarpals. This release must be absolute to allow independent mobilization of the index ray.
- Surgical Warning: Avoid excessive traction on the neurovascular bundles during this release, as pediatric vessels are highly prone to vasospasm.
-
Basal Metacarpal Exposure:
- Make a second short, curved dorsoradial incision at the base of the index metacarpal.
- Elevate full-thickness flaps to expose the periosteum of the proximal metacarpal shaft and base. Subperiosteal dissection should be minimized to preserve the diaphyseal blood supply.
-
Osteotomy and Recession:
- Perform a transverse osteotomy at the base of the index metacarpal using an oscillating microsaw. Once osteotomized, the metacarpal shaft can be easily grasped with a bone clamp and maneuvered.
- Recess the metacarpal by resecting exactly 1.5 to 2.0 cm of the proximal metacarpal shaft. The exact amount depends on the age and size of the child, aiming to align the new thumb tip with the proximal interphalangeal joint of the middle finger.
-
Three-Dimensional Repositioning:
- Reposition the distal metacarpal segment into the functional thumb position: 20 degrees of radial abduction, 35 degrees of palmar abduction, and 100 to 110 degrees of axial rotation (pronation).
-
Skeletal Fixation:
- Once the desired spatial orientation and recession length are achieved, maintain the reduction manually.
- Pass two smooth Kirschner wires (0.035 or 0.045 inch, depending on patient size) percutaneously through the recessed index metacarpal into the adjacent middle metacarpal (and carpus if necessary) to secure the construct.
- Confirm the position, rotation, and hardware placement under fluoroscopy.
-
Closure and Immobilization:
- Deflate the tourniquet and achieve meticulous hemostasis.
- Close the incisions routinely with absorbable sutures (e.g., 5-0 chromic gut or fast-absorbing plain gut).
- Apply a sterile, non-adherent dressing followed by a well-padded, long-arm cast that rigidly holds the repositioned index finger in its new abducted and rotated position.
CONGENITAL CLASPED THUMB
Congenital clasped thumb is a complex and unusual condition characterized by a fixed posture of the thumb in adduction and extreme flexion at the metacarpophalangeal (MCP) joint. Unlike a simple trigger thumb, which involves flexion at the interphalangeal (IP) joint due to a flexor tendon nodule, the clasped thumb represents a fundamental imbalance between the extrinsic flexors and the deficient extensors of the thumb.
Pathoanatomy and Etiology
The primary pathoanatomic feature is the underlying hypoplasia or complete absence of the extensor pollicis brevis (EPB) muscle. In more severe variants, the extensor pollicis longus (EPL) may also be absent or severely attenuated. This lack of extensor tone allows the normal flexor pollicis longus (FPL) and intrinsic thenar muscles to pull the thumb into a tightly clasped position within the palm.

Clinical appearance of a pediatric hand demonstrating severe thumb hypoplasia and a clasped posture, requiring complex metacarpal transfer and soft tissue reconstruction.

Preoperative radiograph of a child with thumb hypoplasia, illustrating the skeletal deficiencies that often accompany the soft-tissue imbalances seen in clasped thumb deformities.
This deformity may present as an isolated anomaly, or it may be syndromic, frequently associated with clubfoot deformities, arthrogryposis, or Freeman-Sheldon syndrome.
Classification System (Weckesser, Reed, and Heiple)
Weckesser, Reed, and Heiple classified the congenital clasped thumb syndrome into four distinct etiological categories to guide treatment:
- Group 1 (Deficient Extension Only): The most common variant. It is characterized by isolated absence or hypoplasia of the EPB/EPL without severe soft tissue contractures. It appears to be transmitted via a sex-linked recessive gene, as it is predominantly seen in boys and is frequently bilateral.
- Group 2 (Flexion Contracture Combined with Deficient Extension): Involves extensor deficiency compounded by secondary contractures of the volar skin, first web space, and flexor musculature.
- Group 3 (Hypoplasia of the Thumb): A severe form involving global hypoplasia of the thumb ray, including profound tendon and thenar muscle deficiencies, often with MCP joint instability.
- Group 4 (Unclassified): Deformities that do not easily fit into the first three categories, often associated with severe syndromic conditions like arthrogryposis multiplex congenita.
Clinical Evaluation and Diagnosis
At birth, it is physiological for an infant to clutch the thumb within the palm (cortical thumbing). However, a normal infant will intermittently release the thumb and actively extend it.
🚨 Diagnostic Pitfall: Trigger Thumb vs. Clasped Thumb
Do not confuse a congenital clasped thumb with a pediatric trigger thumb. A trigger thumb presents with a fixed flexion deformity at the interphalangeal (IP) joint with a palpable Notta's node at the A1 pulley. A clasped thumb presents with flexion and adduction primarily at the metacarpophalangeal (MCP) joint.
If prolonged observation reveals an absolute lack of active extension at the MCP joint, and particularly if this persists beyond 3 months of age, the definitive diagnosis of congenital clasped thumb is established.
Nonoperative Management
Most clasped thumb deformities fall into Group 1 (deficiencies of extension only) and exhibit an excellent response to early, conservative management.
- Splinting Protocol: Early splinting in extension and abduction is initiated. A custom-molded thermoplastic or plaster splint is applied to hold the thumb out of the palm.
- Duration: The splint is worn continuously and changed every 6 weeks to accommodate growth. This protocol is maintained for 3 to 6 months.
- Prognosis: If the initial response to splinting is favorable, long-term functional results are generally satisfactory. However, if there is no evidence of active MCP joint extension after 3 to 6 months of rigid splinting, further conservative management is futile. This lack of response confirms that the extrinsic extensors are extremely deficient or totally absent, necessitating surgical tendon transfer.
Operative Treatment and Tendon Transfers
When surgery is indicated (typically after 1 year of age but before school age), the goal is to restore active extension and clear the thumb from the palm.
Donor Tendon Selection:
For an inadequate or absent EPL, several donor tendons are viable:
1. Extensor Indicis Proprius (EIP): The most common and reliable transfer for EPL reconstruction. It has appropriate excursion and its harvest leaves minimal donor site morbidity.
2. Palmaris Longus (PL): Useful if the EIP is unavailable or if multiple transfers are needed.
3. Brachioradialis (BR): Provides excellent power but requires a tendon graft (e.g., plantaris or toe extensor) to reach the thumb.
4. Flexor Digitorum Superficialis (FDS): Typically the ring finger FDS is used in severe cases requiring robust power.
If the EPB is the sole deficient muscle, it can be effectively replaced by transferring the EIP to the EPB insertion at the base of the proximal phalanx.
Management of Group 3 Deformities (The Neviaser Protocol)
Group 3 deformities present a formidable challenge due to significant hypoplasia of the thenar muscles, absence of the abductor pollicis longus (APL), and gross instability of the MCP joint. Neviaser recommended a comprehensive, single-stage reconstructive operation:
- Chondrodesis of the MCP Joint: To provide a stable post for pinch, the unstable MCP joint is fused (chondrodesis preserves the physis for future longitudinal growth).
- Extensor Reconstruction: The absent EPL is replaced with the EIP.
- Abductor Reconstruction: The absent APL is replaced with the Palmaris Longus.
- Huber Opponensplasty: To restore thenar bulk and opposition, the abductor digiti minimi (ADM) is transferred to the thumb (Huber procedure).
- Web Space Deepening: Z-plasties or dorsal rotational flaps are utilized to release the adduction contracture of the first web space.
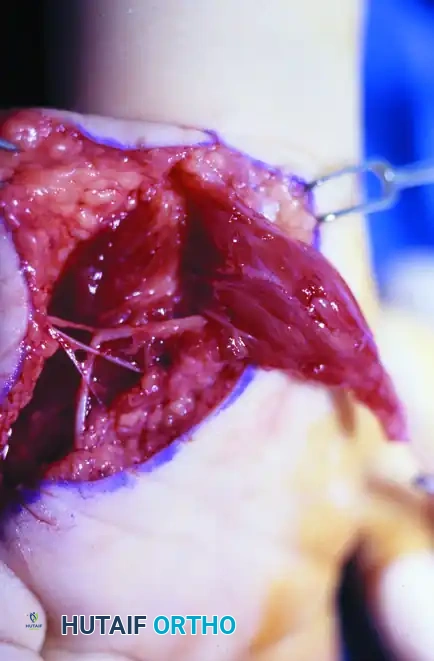
Intraoperative photograph demonstrating the Huber opponensplasty. The abductor digiti minimi muscle belly has been mobilized on its neurovascular pedicle and is being routed subcutaneously across the palm to reconstruct the deficient thenar eminence.

Postoperative clinical appearance of the hand following a comprehensive single-stage reconstruction (Neviaser protocol). Note the restored first web space, improved thenar bulk from the Huber transfer, and the functional resting posture of the thumb.
Despite the magnitude of this multi-tissue reconstruction, Neviaser reported obtaining useful grasp and pinch with minimal complications when performed meticulously in the preschool-aged child.
Surgical Technique: Extensor Reconstruction (Littler Technique)
When performing a tendon transfer for congenital clasped thumb, the routing and tensioning of the transfer are critical for success. The Littler technique provides a reliable method for securing the transferred tendon.
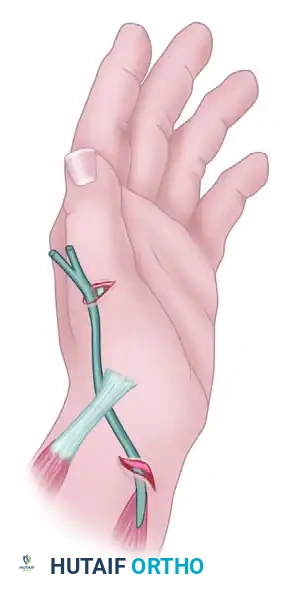
Diagram A: Path of the transferred tendon. The donor tendon (e.g., EIP) is routed subcutaneously to align with the anatomical axis of the deficient extensor pollicis longus.

Diagram B: Suture of the transferred tendon. The Littler technique utilizes a woven, interlacing suture method (Pulvertaft weave) to ensure a biomechanically robust repair that can withstand early postoperative rehabilitation.
Key Steps in Tendon Transfer:
1. Harvest: The EIP is identified over the index metacarpal (it lies ulnar to the Extensor Digitorum Communis tendon). It is transected just proximal to the extensor hood.
2. Routing: The tendon is withdrawn to the wrist level and routed subcutaneously in a straight line toward the thumb MCP joint.
3. Tensioning and Weave: The thumb is held in full extension and slight radial abduction. The EIP is woven through the remnant of the EPL or directly into the periosteum/extensor expansion using a Pulvertaft weave (as shown in Diagram B). Tension is set slightly tighter than physiological resting tension to account for postoperative stretching.
POSTOPERATIVE CARE AND REHABILITATION
The success of both index finger recession and clasped thumb reconstruction relies heavily on strict adherence to postoperative immobilization and subsequent rehabilitation.
Phase 1: Strict Immobilization (Weeks 0-4)
* Immediately postoperatively, the limb is immobilized in a well-padded, long-arm cast. For index recession, the cast must meticulously support the pollicized/recessed digit in its new abducted and rotated position. For clasped thumb transfers, the thumb is immobilized in maximum extension and abduction.
* At 2 weeks postoperative, the cast is bivalved or changed in the clinic. Skin sutures are removed. A new, snug long-arm cast is applied to continue supporting the reconstruction for an additional 2 to 4 weeks.
Phase 2: Hardware Removal and Transition (Weeks 4-6)
* If Kirschner wires were utilized (e.g., for index recession or MCP chondrodesis), they are removed in the clinic once radiographic evidence of early bone healing is confirmed, typically between 4 to 6 weeks after the operation.
* The patient is transitioned from a rigid cast to a custom thermoplastic splint. The thumb is splinted in a functional resting position.
Phase 3: Rehabilitation and Motor Re-education (Weeks 6-12)
* Progressively increasing activities are allowed.
* The custom splint is worn continuously between exercise sessions and at night for another 4 to 6 weeks.
* Pediatric occupational therapy is initiated. Therapy focuses on play-based motor re-education, encouraging the child to incorporate the newly reconstructed thumb or recessed index finger into large object grasping, and eventually, fine motor pincer grips.
* Because cortical plasticity is highest in the preschool years, children typically adapt to the altered biomechanics rapidly, integrating the reconstructed digit into spontaneous daily activities.
📚 Medical References
- congenital clasped thumb, Plast Reconstr Surg 34:612, 1964.
- Cheng JCY, Chan KM, Ma GFY, et al: Polydactyly of the thumb: a surgical plan based on 95 cases, J Hand Surg 9A:155, 1984.
- DeHaan MR, Wong LB, Peterson DP: Congenital anomaly of the thumb: aplasia of the fl exor pollicis longus, J Hand Surg 12A:108, 1987.
- Egloff DV, Verdan CL: Pollicization of the index fi nger for reconstruction of the congenitally hypoplastic or absent thumb, J Hand Surg 8A:839, 1983.
- Fitch RD, Urbaniak JR, Ruderman RJ: Conjoined fl exor and extensor pollicis longus tendons in hypoplastic thumb, J Hand Surg 9A:417, 1984.
- Flatt AE: The care of congenital hand anomalies, St Louis, 1977, Mosby. Gilbert A: Congenital absence of the thumb and digits, J Hand Surg 14B:6, 1989.
- Huber E: Hilfsoperation bei Medianuslahmung, Dtsch Z Chir 162:271, 1921.
- Lipskeir E, Weizenbluth M: Surgical treatment of the clasped thumb, J Hand Surg 14B:72, 1989.
- Littler JW: The prevention and the correction of adduction contracture of the thumb, Clin Orthop 13:182, 1959.
- Littler JW, Cooley SGE: Opposition of the thumb and its restoration by abductor digiti quinti transfer, J Bone Joint Surg 45A:1389, 1963.
- Manske PR: Redirection of the extensor pollicis longus in the treatment of spastic
You Might Also Like

