Advanced ABOS Part I Orthopaedic Review: Tibia & Osteoporotic Fracture Fixation | Part 21584
Key Takeaway
This module offers 21 advanced multiple-choice questions mirroring the ABOS Part I and AAOS OITE exams. It covers critical topics like proximal tibia intramedullary nailing, osteoporotic fracture fixation for hip, humerus, and distal radius, along with secondary fracture prevention via Fracture Liaison Services. Ideal for comprehensive orthopaedic board preparation.
Advanced ABOS Part I Orthopaedic Review: Tibia & Osteoporotic Fracture Fixation | Part 21584
A 35-year-old male sustains a high-energy injury resulting in a proximal tibia fracture. Clinical exam reveals an intact neurovascular status and no signs of compartment syndrome. What is the most appropriate initial imaging study to fully characterize the fracture pattern and guide surgical planning, especially considering potential articular involvement?
Correct Answer: C
The case emphasizes that CT scans are essential for all suspected intra-articular involvement and for complex meta-diaphyseal fractures. CT provides detailed information on fracture morphology, fragment size, comminution, and helps in planning reduction strategies (e.g., identifying blocking screw trajectories, assessing articular step-off). Sagittal and coronal reconstructions are particularly useful. While plain radiographs (Option B) are crucial for initial assessment, they often underestimate the extent of articular involvement and comminution in proximal tibia fractures. MRI (Option D) is excellent for soft tissue injuries (ligaments, menisci) but is not the primary imaging modality for detailed bone fracture morphology in the acute setting. Long-leg alignment films (Option E) are helpful for overall limb alignment but are not typically performed acutely for fracture characterization. Standard AP and lateral radiographs of the knee only (Option A) are insufficient as they do not show the entire tibia or ankle, which is necessary for assessing overall alignment and planning nail length.
A 48-year-old male presents with an AO/OTA 41-A3 fracture of the proximal tibia. The fracture is extra-articular, comminuted in the metaphysis, but the articular surface is intact. Soft tissues are amenable to surgery. Which of the following is the most appropriate primary surgical fixation method for this fracture pattern?
Correct Answer: C
The case explicitly states that intramedullary nailing (IMN) is primarily indicated for extra-articular or meta-diaphyseal proximal tibia fractures (AO/OTA 41-A, or 42-A extending proximally) where the fracture line does not significantly compromise the articular surface or metaphyseal cortical support. An AO/OTA 41-A3 fracture is an extra-articular, multifragmentary metaphyseal fracture. The advantages of IMN include load-sharing fixation, smaller incisions, less soft tissue stripping, and improved healing rates compared to plating for certain patterns. ORIF with plates (Options A and E) is typically reserved for significant articular involvement (e.g., Schatzker Type IV-VI, or AO/OTA 41-B/C) requiring anatomical reduction and absolute stability. External fixation (Option B) is usually a temporizing measure for severe soft tissue compromise or in polytrauma, not a definitive primary fixation for this pattern. Non-operative management (Option D) is generally for minimally displaced, stable fractures, which is not the case for a comminuted 41-A3 fracture.
During intramedullary nailing of a proximal tibia fracture, the most common and challenging malalignment to prevent is procurvatum (apex anterior angulation). Which of the following biomechanical factors is the primary contributor to this specific deformity?
Correct Answer: C
The case explicitly identifies the deforming forces contributing to malreduction. For procurvatum (apex anterior angulation), it states: 'The nail's straight trajectory attempts to straighten the natural anterior bow of the tibia, pushing the proximal fragment into procurvatum (apex anterior angulation). This is the most common malalignment.' It also mentions that patellar tendon tension can contribute if an infrapatellar entry point is used. Option A (proximal flare) primarily contributes to valgus malalignment. Option B (natural valgus alignment) is a normal anatomical feature, and failure to account for it can lead to valgus malalignment, not procurvatum. Option D (muscle pull) influences overall fragment position but is not the primary biomechanical reason for the nail-induced procurvatum. Option E describes a neurovascular risk, not a biomechanical deforming force.
A surgeon is preparing for intramedullary nailing of a proximal tibia fracture. The image shows an intraoperative fluoroscopic view during guidewire placement. To minimize the risk of procurvatum and anterior knee pain, which entry point and approach is generally preferred for proximal tibia fractures?
Correct Answer: C
The case highlights the evolution of techniques, stating: 'The development of anatomically pre-bent nails and, crucially, the widespread adoption of the semi-extended (suprapatellar) approach, have significantly improved outcomes by allowing a more central and posterior entry point, thereby reducing the incidence of procurvatum and anterior knee pain.' The suprapatellar approach, with the knee flexed approximately 15-20 degrees, allows for a more anatomical and central entry point through the suprapatellar region, which better controls procurvatum and reduces anterior knee pain. The traditional infrapatellar approaches (Options A, B, D) are more prone to creating an apex anterior (procurvatum) deformity due to the acute angle of nail entry relative to the proximal fragment, and are associated with higher rates of anterior knee pain. A lateral parapatellar approach (Option E) is not a standard entry point for tibial IMN.
During IMN for a proximal tibia fracture, the surgeon notes persistent procurvatum (apex anterior angulation) on the lateral fluoroscopic view, similar to the malalignment seen in the provided image (lateral view). The guidewire is already in place. Which of the following is the most effective intraoperative maneuver to correct this procurvatum before reaming?
Correct Answer: D
The case specifically addresses the correction of procurvatum (apex anterior angulation). It states: 'Blocking Screws: An anterior-to-posterior blocking screw placed in the proximal fragment just anterior to the nail trajectory forces the nail posteriorly.' This acts as a bumper, guiding the nail posteriorly and correcting the apex anterior angulation. Option B describes a blocking screw placement that would exacerbate procurvatum or cause recurvatum. Option C is a preventive measure during nail insertion, not a corrective maneuver for existing malreduction with the guidewire in place. Option A and E are maneuvers for correcting valgus/varus malalignment, not procurvatum.
A 62-year-old patient undergoes IMN for a proximal tibia fracture. Intraoperatively, despite traction and manual reduction, the AP fluoroscopic view reveals persistent valgus malalignment of the proximal fragment, similar to the malalignment seen in the provided image (AP view). The guidewire is centrally placed in the distal fragment. Which of the following is the most appropriate next step to correct this valgus deformity?
Correct Answer: C
The case describes the use of blocking screws for valgus correction: 'Valgus Correction: Place a blocking screw on the lateral side of the proximal fragment, just lateral to the intended nail path, forcing the nail medially and correcting valgus.' This eccentric placement of the blocking screw acts as a fulcrum, pushing the nail towards the desired central axis and correcting the valgus. Option A describes a blocking screw placement that would exacerbate valgus or cause varus. Option B (direct medial force) is a manual reduction maneuver, which the question states has already been attempted and failed to fully correct the deformity. Option D is incorrect as rapid nail advancement without proper reduction can lead to iatrogenic fracture or worsen malalignment. Option E is a maneuver for correcting procurvatum, not valgus.
A 55-year-old male sustains a comminuted extra-articular proximal tibia fracture (AO/OTA 41-A3) with a significant medial metaphyseal wall defect. After achieving provisional reduction and inserting an intramedullary nail, the surgeon is concerned about potential valgus collapse and instability. Which adjunctive fixation technique would be most appropriate to enhance stability in this scenario?
Correct Answer: C
The case discusses adjunctive fixation, stating: 'Supplemental Plating: In cases of severe metaphyseal comminution or large medial/lateral wall defects, a small anti-glide plate or buttress plate (e.g., a 1/3 tubular plate or specific metaphyseal plate) can be applied percutaneously or through a small incision to provide additional stability and prevent collapse, especially on the medial side for valgus stability.' A medial wall defect specifically predisposes to valgus collapse, making a medial buttress plate ideal. Cerclage wires (Option A) are rarely used in the metaphysis and are more for long oblique or spiral diaphyseal fractures. Additional distal locking screws (Option B) would not address proximal metaphyseal instability. Exchange nailing (Option D) is typically for nonunion or delayed union, not for acute instability with a defect. Converting to external fixation (Option E) would be a step down in stability and is usually reserved for severe soft tissue issues or infection.
A 30-year-old patient undergoes IMN for a proximal tibia fracture. Eighteen months post-surgery, the fracture is fully united, but the patient complains of persistent, debilitating anterior knee pain, especially with kneeling and squatting. Clinical examination reveals tenderness over the superior pole of the patella. Which of the following is the most common reason for secondary surgical intervention in this patient's situation?
Correct Answer: C
The case identifies anterior knee pain as a very common complication: 'Anterior Knee Pain: Very common, up to 50-60% with infrapatellar approach. Less with suprapatellar.' It further states under management: 'Hardware removal (nail/proximal locking screws) after fracture union for persistent symptomatic pain. This is the most common reason for secondary surgery.' The patient's symptoms (persistent anterior knee pain, tenderness over the superior pole of the patella, especially with kneeling/squatting) are classic for hardware-related anterior knee pain. Nonunion (Option A) is ruled out as the fracture is fully united. Deep infection (Option B) would present with different symptoms (fever, drainage, severe pain, elevated inflammatory markers). Rotational malunion (Option D) would cause gait disturbance and patellofemoral pain but is not described as the *most common* reason for secondary surgery, and the primary complaint is localized anterior knee pain. Compartment syndrome (Option E) is an acute emergency, not a chronic post-operative complication 18 months later.
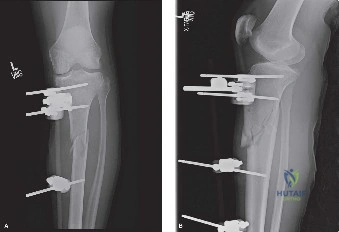
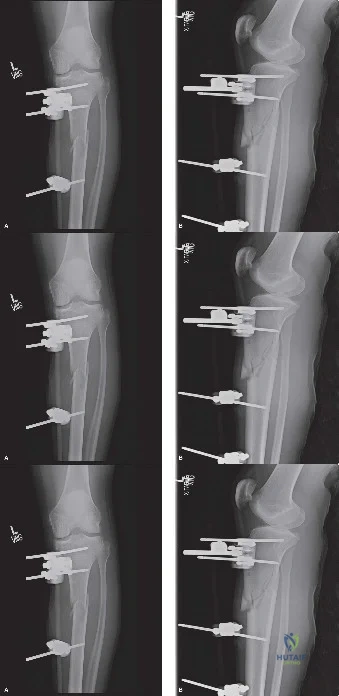
A 70-year-old female presents for follow-up 6 months after intramedullary nailing of a proximal tibia fracture. She complains of persistent knee pain and an altered gait. The provided radiographs show the post-operative result. Based on these images, what is the most significant malunion present?
Correct Answer: D
The provided image clearly demonstrates both procurvatum and valgus malalignment. On the lateral view, the proximal fragment is angled anteriorly relative to the distal fragment, indicating procurvatum (apex anterior angulation). On the AP view, the proximal fragment is angled laterally, indicating valgus malunion. The case identifies both procurvatum and valgus as common malunions with IMN in the proximal tibia. Shortening (Option A) is not evident as the primary significant malunion. Varus malunion (Option B) would be an apex medial angulation on the AP view, which is not seen. Recurvatum (Option C) would be an apex posterior angulation on the lateral view, which is the opposite of what is seen. Rotational malunion (Option E) cannot be definitively assessed from these two standard views alone, though it is a common complication, the most obvious deformities here are angular.
A 40-year-old male undergoes IMN for a stable, extra-articular proximal tibia fracture (AO/OTA 41-A1) with rigid fixation. The soft tissues are healthy, and there are no signs of compartment syndrome. What is the most appropriate initial post-operative weight-bearing protocol for this patient?
Correct Answer: C
The case outlines post-operative rehabilitation protocols, stating for weight-bearing: 'Weight-Bearing As Tolerated (WBAT): For stable, simple fracture patterns with rigid fixation, often initiated early if deemed safe by the surgeon.' An AO/OTA 41-A1 fracture is a simple extra-articular metaphyseal fracture, and with rigid IMN fixation and healthy soft tissues, early WBAT is appropriate. Strict NWB (Option A) or TDWB (Option B) would be reserved for more unstable or comminuted fractures, or if fixation is not fully rigid. CPM (Option D) is for range of motion, not a weight-bearing protocol. FWB without assistive devices (Option E) is generally too aggressive immediately post-operatively, even for stable fractures, as patients still need to regain strength and confidence.
A 78-year-old female with a history of osteoporosis (T-score -3.1 at the femoral neck) presents to the emergency department after a mechanical fall from standing height, sustaining a displaced intertrochanteric hip fracture. She has multiple comorbidities including well-controlled hypertension and type 2 diabetes. Pre-operative imaging confirms a comminuted intertrochanteric fracture. The orthopedic surgeon plans for cephalomedullary nailing. During the procedure, after guide wire placement and reaming, the lag screw is inserted. Intraoperative fluoroscopy reveals the following image:
Based on the principles of osteoporotic fracture fixation and the provided image, what is the most critical technical parameter to assess to prevent lag screw cut-out in this patient?
Correct Answer: C
The most critical technical parameter to assess to prevent lag screw cut-out in osteoporotic intertrochanteric fractures is the Tip-Apex Distance (TAD). As highlighted in the case, the sum of the distance from the tip of the lag screw to the apex of the femoral head on both AP and lateral fluoroscopic views must be strictly less than 25 millimeters. A TAD greater than 25 millimeters exponentially increases the risk of the lag screw cutting out through the superior aspect of the osteoporotic femoral head, leading to construct failure and the need for revision surgery, often to arthroplasty.
Option A (The angle of the lag screw relative to the femoral shaft axis) is important for achieving appropriate reduction and load sharing, but it is secondary to TAD in predicting cut-out. An incorrect angle might lead to malreduction or nonunion, but TAD directly quantifies the screw's position within the femoral head, which is crucial for resisting shear forces in osteoporotic bone.
Option B (The length of the intramedullary nail) is important for bypassing the fracture and providing adequate diaphyseal fixation, especially in subtrochanteric extensions or to prevent periprosthetic fractures. However, it does not directly address the stability of the lag screw within the femoral head.
Option D (The number of distal interlocking screws) is important for controlling rotation and preventing shortening of the femoral shaft, but it does not influence the primary failure mode of lag screw cut-out from the femoral head.
Option E (The diameter of the lag screw) can influence pull-out strength to some extent, with larger diameters generally providing more purchase. However, the position of the screw within the femoral head (TAD) is a far more significant predictor of cut-out than screw diameter, especially in severely osteoporotic bone where even a larger screw can cut out if eccentrically placed.
A 65-year-old postmenopausal female with severe osteoporosis (T-score -3.5) sustains a highly comminuted, displaced 4-part proximal humerus fracture after a low-energy fall. She is physiologically active and desires to return to her previous level of function. Pre-operative CT scan reveals significant metaphyseal comminution and a deficient medial calcar. The orthopedic surgeon plans for open reduction and internal fixation (ORIF) with a locking plate. During the procedure, after reduction and plate application, the surgeon notes persistent concern for varus collapse. Which of the following intraoperative strategies is most critical to address this specific concern in osteoporotic bone?
Correct Answer: C
In osteoporotic proximal humerus fractures, the medial hinge is frequently comminuted, leading to a high risk of varus collapse post-fixation. The case specifically states a deficient medial calcar. To counteract varus deforming forces and provide structural support, the most critical strategy is to place inferomedial calcar screws into the inferior quadrant of the humeral head. These screws act as a structural strut, resisting the tendency for the humeral head to collapse into varus, which is a common failure mode in osteoporotic bone.
Option A (Utilizing a longer plate to increase the working length) is important for distributing stress and promoting secondary healing in diaphyseal fractures or when bypassing stress risers. However, it does not directly address the specific issue of varus collapse at the metaphyseal-head junction in a proximal humerus fracture.
Option B (Placing additional screws into the greater tuberosity) is important for securing the tuberosities, which is crucial for rotator cuff healing and function. While important for overall construct stability, it does not directly provide the medial column support needed to prevent varus collapse of the humeral head itself.
Option D (Performing a meticulous repair of the rotator cuff tendons) is essential for restoring shoulder function and preventing rotator cuff pathology. However, it is a soft tissue repair and does not provide the immediate mechanical support required to prevent acute varus collapse of the bony construct.
Option E (Applying a bone graft substitute to the fracture site) can be helpful to fill metaphyseal voids and promote healing, but it typically provides biological rather than immediate structural support. While it can contribute to long-term stability, it is not as immediately critical for preventing varus collapse as direct mechanical support from calcar screws.
A 72-year-old male with a history of chronic obstructive pulmonary disease and a recent fragility fracture of the distal radius is being evaluated for secondary fracture prevention. His DEXA scan shows a T-score of -2.8 at the lumbar spine. He is currently taking calcium and Vitamin D supplements. Which of the following pharmacological interventions would be the most appropriate initial step for this patient, considering his history of a fragility fracture and severe osteoporosis?
Correct Answer: C
The patient has a fragility fracture and a DEXA T-score of -2.8, which meets the criteria for osteoporosis. A fragility fracture is a sentinel event, significantly increasing the risk of subsequent fractures. The case emphasizes that antiresorptive agents, such as bisphosphonates (e.g., alendronate, zoledronic acid) or RANKL inhibitors (denosumab), are the critical initial pharmacological interventions to decrease osteoclast activity and prevent further bone degradation. Bisphosphonates are typically the first-line therapy due to their efficacy, cost-effectiveness, and long-standing evidence base.
Option A (Initiate teriparatide) and Option B (Initiate romosozumab) are anabolic agents that stimulate osteoblast-mediated bone formation. While highly effective, they are generally reserved for patients with severe osteoporosis, those who fracture while on antiresorptive therapy, or those with very high fracture risk. They are typically not the first-line agents for initial management after a first fragility fracture unless there are specific contraindications to antiresorptives or a history of multiple fractures.
Option D (Increase calcium and Vitamin D supplementation only) is insufficient. While calcium and Vitamin D supplementation form the baseline of all pharmacological regimens, they alone are not adequate to treat established osteoporosis with a fragility fracture. Active pharmacological intervention to either reduce bone resorption or stimulate bone formation is required.
Option E (Prescribe calcitonin nasal spray) is a less potent antiresorptive agent, primarily used for pain relief in acute vertebral compression fractures and has limited efficacy in preventing future fractures compared to bisphosphonates or other agents. It is not considered a first-line treatment for osteoporosis.
A 68-year-old female presents with a displaced intra-articular distal radius fracture after a fall. She has a history of osteoporosis and is otherwise healthy. Pre-operative CT scan confirms significant comminution of the articular surface. The orthopedic surgeon plans for open reduction and internal fixation (ORIF) with a volar locking plate. During the approach, the surgeon identifies the flexor carpi radialis (FCR) tendon. Which of the following statements regarding the surgical technique for volar plating of the distal radius in osteoporotic bone is most accurate?
Correct Answer: B
In osteoporotic distal radius fractures, the metaphyseal cancellous bone is often crushed, leaving a void upon reduction. The volar locking screws act as a rigid structural scaffold holding the articular fragments in space. Therefore, placing the distal locking screws as close to the subchondral bone as possible is crucial to support the articular surface and prevent dorsal settling, which is a common complication in osteoporotic bone.
Option A (The plate should be positioned distal to the watershed line to maximize articular support) is incorrect. The plate must be positioned proximal to the watershed line to prevent flexor tendon irritation and subsequent rupture. Positioning distal to the watershed line significantly increases the risk of flexor tendon complications.
Option C (Direct anatomical reduction of every fragment is paramount to ensure optimal outcome) is incorrect. The case emphasizes that in osteoporotic bone, direct exposure and anatomical reduction of every fragment will inevitably strip the periosteal blood supply, leading to nonunion and implant failure. Indirect reduction techniques are preferred, focusing on restoration of length, alignment, and rotation (spatial reduction) rather than absolute anatomical cortical contact.
Option D (The brachioradialis insertion must be preserved to maintain wrist stability) is incorrect. The case states that release of the brachioradialis insertion is often necessary to neutralize its deforming supinator and flexing forces on the distal fragment, especially in comminuted fractures, to achieve adequate reduction.
Option E (Non-locking screws are preferred to allow for dynamic compression at the fracture site) is incorrect. The case explicitly states that volar locking plates are the implant of choice for distal radius fragility fractures. Locking screws thread directly into the plate, creating a fixed-angle construct that functions as an internal fixator, which is essential in osteoporotic bone where standard cortical screws often strip due to poor bone quality.
A 70-year-old male with severe osteoporosis (T-score -3.0) sustains a subtrochanteric femur fracture. He is medically optimized for surgery. The orthopedic surgeon plans for intramedullary nailing. During the procedure, the surgeon encounters difficulty achieving adequate purchase with standard cortical screws for distal locking, noting the bone feels 'crunchy' and prone to stripping. This observation is consistent with the biomechanical properties of osteoporotic bone. Which of the following statements best describes the microarchitectural changes contributing to this challenge?
Correct Answer: B
The case describes that cortical bone in osteoporotic patients undergoes significant thinning, with increased porosity secondary to the expansion of Haversian canals and heightened intracortical remodeling. This geometric alteration drastically reduces the area moment of inertia, leading to diminished bending and torsional strength. This microarchitectural degradation directly contributes to the 'crunchy' feel and susceptibility to stripping during screw insertion, as the thin, porous cortices cannot withstand the torque required for adequate purchase.
Option A (Increased bone mineral density leading to excessive rigidity) is incorrect. Osteoporosis is characterized by decreased bone mineral density, not increased, leading to fragility rather than excessive rigidity.
Option C (Pathological conversion of rod-like trabeculae to plate-like structures in cancellous bone) is incorrect. The case states the opposite: there is a pathological conversion of plate-like trabeculae to mechanically inferior rod-like structures, leading to a critical loss of connectivity and reduced ability to resist compressive and shear loads.
Option D (Increased collagen cross-linking leading to enhanced bone toughness) is incorrect. The case states that alterations in collagen cross-linking and mineral crystal size lead to increased brittleness and reduced toughness, making the bone more susceptible to comminution.
Option E (Reduced porosity of cortical bone, making it denser but more brittle) is incorrect. Cortical bone in osteoporosis exhibits *increased* porosity, not reduced, due to Haversian canal expansion, which makes it weaker and more prone to stripping, not denser.
A 82-year-old frail female with severe dementia and a non-displaced femoral neck fracture is admitted. She is non-ambulatory at baseline and experiences minimal pain with passive range of motion. Her medical history includes severe cardiac disease (ASA V), making her an extremely high anesthetic risk. Her family is primarily concerned with her comfort. Based on the provided case, what is the most appropriate management strategy for this patient?
Correct Answer: C
The case provides specific non-operative indications for proximal femur fractures: 'Non-ambulatory patient with severe dementia and minimal pain; Unacceptable anesthetic risk (ASA V).' This patient perfectly fits these criteria. Given her severe dementia, non-ambulatory status, minimal pain, and unacceptable anesthetic risk (ASA V), the primary goal shifts from restoring ambulation to ensuring comfort and avoiding the significant physiological burden of surgery. Non-operative management with analgesia and comfort care is the most appropriate strategy.
Option A (Urgent hemiarthroplasty to allow for immediate weight-bearing) and Option E (Total hip arthroplasty to ensure long-term stability) are typically the gold standard for displaced femoral neck fractures in physiologically active osteoporotic patients to allow immediate weight-bearing and prevent avascular necrosis. However, for this specific patient, the anesthetic risk and baseline functional status contraindicate major surgery.
Option B (Open reduction and internal fixation with cannulated screws) is generally reserved for non-displaced or minimally displaced femoral neck fractures in younger, physiologically active patients, or as a temporizing measure. It carries a high risk of failure and avascular necrosis in osteoporotic bone and is not suitable for this patient given her comorbidities and functional status.
Option D (Delayed surgical intervention after medical optimization for 72 hours) is generally discouraged for hip fractures. The case states that current guidelines strongly advocate for surgical intervention within 24 to 48 hours of admission, as delays beyond this window are independently associated with increased mortality. While medical optimization is crucial, delaying surgery for 72 hours in a patient who is already ASA V and likely to remain so, with the intent to operate, would be inappropriate and potentially harmful.
A 75-year-old female with known osteoporosis presents with severe, intractable back pain after a fall, diagnosed with an L1 vertebral compression fracture. She has developed progressive neurological deficits, including lower extremity weakness and bowel/bladder dysfunction. Her pain has failed to respond to four weeks of medical management and bracing. Based on the case, which of the following interventions is most indicated for this patient?
Correct Answer: D
The case explicitly lists 'Progressive neurological deficit' as an operative indication for vertebral compression fractures. While cement augmentation (vertebroplasty/kyphoplasty) is indicated for severe, intractable pain failing medical management, the presence of progressive neurological deficits necessitates surgical decompression and stabilization to address the spinal cord or nerve root compression. This is a critical distinction, as cement augmentation alone does not decompress neural elements.
Option A (Continued non-operative management with increased analgesia and physical therapy) is inappropriate given the progressive neurological deficit and intractable pain that has failed four weeks of medical management. This patient requires more aggressive intervention.
Option B (Vertebroplasty or kyphoplasty for cement augmentation) is indicated for severe, intractable pain failing medical management, but it does not address neurological deficits. Cement augmentation primarily stabilizes the vertebral body and reduces pain, but it does not decompress the spinal canal.
Option C (Referral to a pain management specialist for nerve blocks) might be considered for pain management in stable fractures, but it does not address the underlying mechanical instability or the progressive neurological deficit, which requires surgical intervention.
Option E (Initiation of anabolic agents for bone formation) is part of secondary fracture prevention and long-term osteoporosis management. While important, it is not an acute treatment for a symptomatic vertebral compression fracture with neurological compromise.
A 70-year-old female undergoes open reduction and internal fixation (ORIF) of a comminuted intertrochanteric hip fracture with a cephalomedullary nail. Post-operatively, she is allowed immediate weight-bearing as tolerated (WBAT). Six months later, she presents with new onset thigh pain and is diagnosed with a periprosthetic fracture distal to the tip of the intramedullary nail. The case describes this as a common complication in osteoporotic bone. What is the most likely mechanism for this complication, and what is the general salvage strategy?
Correct Answer: C
The case explicitly lists 'Periprosthetic Fracture' as a complication with a mechanism of 'Stress riser effect at the end of a rigid construct.' The salvage strategy is 'Managed by bypassing the fracture with a longer intramedullary nail or overlapping locking plates.' This perfectly matches the clinical scenario described, where the fracture occurs distal to the tip of the nail, indicating a stress concentration at the junction of the rigid implant and the osteoporotic bone.
Option A (Implant breakage due to material fatigue; Salvage requires removal of the broken implant and re-nailing with a stronger material) is incorrect. The case states that 'Hardware failure in osteoporotic bone rarely occurs due to implant breakage; rather, it occurs at the bone-implant interface.'
Option B (Nonunion at the original fracture site leading to increased stress on the distal femur; Salvage requires revision ORIF with bone grafting) is a possible complication, but it's not the primary mechanism for a *periprosthetic fracture distal to the implant tip*. A nonunion would typically lead to failure at the original fracture site, not a new fracture distal to the implant.
Option D (Infection around the implant leading to bone lysis; Salvage requires debridement, antibiotics, and potentially implant removal) is a serious complication, but the clinical vignette does not suggest infection. While infection can lead to implant loosening and bone loss, the described mechanism of a periprosthetic fracture at the implant tip is typically mechanical.
Option E (Excessive weight-bearing post-operatively; Salvage requires a period of non-weight-bearing and cast immobilization) is incorrect. The case emphasizes that the surgical construct must be engineered to withstand weight-bearing as tolerated (WBAT) immediately post-operatively, and early mobilization is critical. The periprosthetic fracture is a failure of the construct's ability to distribute stress, not necessarily due to 'excessive' weight-bearing in a patient allowed WBAT.
A 60-year-old female with a history of chronic steroid use for rheumatoid arthritis (a risk factor for secondary osteoporosis) presents with a displaced femoral neck fracture. She is otherwise healthy and active. After thorough medical optimization, the orthopedic surgeon is considering surgical options. Based on the principles outlined in the case for osteoporotic fractures, which surgical approach is generally considered the gold standard for this patient?
Correct Answer: B
The case explicitly states: 'For displaced femoral neck fractures in the osteoporotic patient, arthroplasty (hemiarthroplasty or total hip arthroplasty) is the gold standard. Osteosynthesis in this cohort carries an unacceptably high rate of avascular necrosis and fixation failure. Arthroplasty allows for immediate weight-bearing, which is critical for survival.' This patient is active and otherwise healthy, making arthroplasty the most appropriate choice to ensure a durable outcome and early mobilization.
Option A (Open reduction and internal fixation with multiple cannulated screws) is generally reserved for non-displaced or minimally displaced femoral neck fractures, or in younger patients where preserving the femoral head is a priority. In osteoporotic patients with displaced fractures, the risk of avascular necrosis and fixation failure with osteosynthesis is unacceptably high.
Option C (Intramedullary nailing with a lag screw) is the preferred technique for intertrochanteric fractures, not typically for displaced femoral neck fractures, where the primary concern is the blood supply to the femoral head and the high risk of nonunion or avascular necrosis.
Option D (External fixation followed by delayed internal fixation) is rarely used for femoral neck fractures and is generally reserved for highly contaminated open fractures or severe pelvic injuries. It is not a standard treatment for a displaced femoral neck fracture in an osteoporotic patient.
Option E (Non-operative management with traction and bed rest) is associated with catastrophic morbidity and mortality in geriatric patients with hip fractures and is considered unacceptable for a displaced femoral neck fracture in an active patient.
A 70-year-old female with severe osteoporosis undergoes open reduction and internal fixation (ORIF) of a comminuted proximal humerus fracture with a locking plate. Post-operatively, she is allowed immediate weight-bearing as tolerated (WBAT). The orthopedic surgeon emphasizes the importance of a Fracture Liaison Service (FLS) and secondary fracture prevention. Which of the following statements best describes the rationale for this emphasis?
Correct Answer: C
The case explicitly states: 'Orthopedic surgeons must not view the treatment of an osteoporotic fracture as complete upon skin closure. A fragility fracture is a sentinel event; the occurrence of one osteoporotic fracture drastically increases the risk of subsequent fractures. The implementation of a Fracture Liaison Service (FLS) or a dedicated bone health optimization protocol is mandatory.' The primary rationale for FLS and secondary prevention is to treat the underlying systemic skeletal disease and prevent subsequent fractures, which are highly likely after an initial fragility fracture.
Option A (To ensure compliance with post-operative physical therapy protocols) is important for rehabilitation, but it is not the primary role or rationale for a Fracture Liaison Service, which focuses on bone health.
Option B (To monitor for implant-related complications such as screw pull-out or plate breakage) is part of routine post-operative follow-up by the orthopedic surgeon, but it is distinct from the broader scope of secondary fracture prevention and bone health management.
Option D (To manage acute post-operative pain and reduce opioid dependence) is a critical aspect of perioperative care but is not the primary function of an FLS, which focuses on long-term bone health.
Option E (To assess the patient's nutritional status and optimize wound healing) is part of general medical optimization and post-operative care, but it is not the specific, overarching goal of a dedicated secondary fracture prevention program like FLS.
A 76-year-old male with a history of multiple medical comorbidities, including severe cardiac disease and chronic kidney disease, sustains a displaced intertrochanteric hip fracture. He is deemed an ASA IV patient. The orthopedic team is discussing the timing of surgery. Based on the AAOS Clinical Practice Guidelines mentioned in the case, what is the recommended timeframe for surgical intervention for this patient?
Correct Answer: B
The case explicitly states: 'The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for the Management of Hip Fractures in the Elderly strongly recommend surgical intervention within 24 to 48 hours of admission to minimize mortality.' While medical optimization is crucial, it should occur concurrently to facilitate surgery within this critical window. Delays beyond this window are independently associated with increased mortality.
Option A (Within 6-12 hours of admission to minimize mortality) is often an ideal goal but may not be feasible for all patients, especially those with significant comorbidities requiring some degree of optimization. The 24-48 hour window is the widely accepted and evidence-based recommendation.
Option C (Delay surgery for 3-5 days to allow for extensive medical workup) is incorrect. Delays beyond 48 hours are associated with increased mortality and complications. While a thorough workup is needed, it should be expedited to meet the 24-48 hour target.
Option D (Only after all comorbidities are fully resolved, regardless of time) is impractical and harmful. Many elderly patients have chronic, unresolvable comorbidities. The goal is optimization, not resolution, to allow for surgery within the recommended timeframe.
Option E (Non-operative management due to high ASA status) is generally reserved for patients with unacceptable anesthetic risk (ASA V) who are non-ambulatory and have minimal pain, as described in a previous question. For an ASA IV patient, the goal is still surgical intervention after optimization, as the mortality and morbidity of non-operative management for hip fractures are extremely high.
To decrease the risk of construct over-stiffness and promote secondary bone healing while using a locked plate, which strategy is most biomechanically sound?
To maximize fixation longevity in her osteoporotic bone, a locked plating construct is chosen. This construct differs from conventional plating by providing stability through which primary mechanism?
What is the primary advantage of utilizing dual locked plating for this specific injury in this demographic?
If mechanical failure occurs due to poor bone quality, which mechanism is most characteristic of a fully locked construct?
The decision to proceed with early total care versus a staged approach (spanning external fixation followed by delayed ORIF) is primarily dictated by which of the following?
What is the optimal surgical interval to address this specific fracture fragment with buttress plating?
None
