Orthopaedic Surgery Board Review: Hand Infections, Gout, & Metacarpal Fractures MCQs | Part 22161
Key Takeaway
This module offers 31 advanced multiple-choice questions mirroring ABOS Part I and AAOS OITE exams. It comprehensively covers critical orthopaedic topics including hand infections (paronychia, flexor tenosynovitis, herpetic whitlow), gout management and diagnosis, and complex metacarpal fracture patterns with surgical considerations. Ideal for board preparation and self-assessment.
Orthopaedic Surgery Board Review: Hand Infections, Gout, & Metacarpal Fractures MCQs | Part 22161
A 58-year-old female presents with a 3-month history of progressive swelling, tenderness, and intermittent purulent discharge from the proximal and lateral nail folds of her right index finger. She works as a dishwasher and reports frequent hand immersion in water. On examination, the nail folds are boggy and erythematous, with significant cuticle loss and mild nail plate discoloration. There is no acute fluctuance, but the symptoms have been refractory to multiple courses of oral antibiotics prescribed by her primary care physician. Which of the following is the most likely etiology and the primary predisposing factor for this patient's condition?
Correct Answer: C
The patient's presentation of a 3-month history of insidious onset, boggy and erythematous nail folds, cuticle loss, nail plate discoloration, and prolonged exposure to moisture (dishwasher) is classic for chronic paronychia. Chronic paronychia is often multifactorial, but fungal colonization, primarily by Candida albicans, is a common etiology, especially in individuals with prolonged exposure to irritants or moisture, which disrupts the protective cuticle and creates a conducive environment for fungal growth. The refractory nature to oral antibiotics further supports a non-bacterial (e.g., fungal) cause.
Incorrect Options:
- A. Staphylococcus aureus infection; nail biting: This describes acute paronychia, which typically has a rapid onset, is bacterial, and often associated with minor trauma like nail biting. The patient's chronic presentation and occupational exposure make this less likely.
- B. Streptococcus pyogenes infection; minor trauma: Similar to option A, Streptococcus pyogenes is a bacterial cause of acute paronychia, usually following minor trauma. This does not fit the chronic, insidious presentation.
- D. Pseudomonas aeruginosa infection; immunocompromise: While gram-negative organisms can cause paronychia, particularly in immunocompromised individuals, Pseudomonas is less common as a primary cause of chronic paronychia compared to Candida in this specific occupational context. The case does not mention immunocompromise.
- E. Viral (HSV) infection; aggressive manicuring: Herpetic whitlow (HSV infection) presents with characteristic vesicles and is typically acute, not chronic over months. Aggressive manicuring can predispose to acute bacterial paronychia, but not typically chronic fungal infections.
A 32-year-old carpenter presents with an acute, painful, fluctuant swelling along the lateral nail fold of his left thumb, consistent with an acute paronychia with abscess formation. During incision and drainage, the surgeon makes a longitudinal incision parallel to the nail plate. Which of the following anatomical structures is most vulnerable to iatrogenic injury if the incision is made too deep or extends too far dorsally?
Correct Answer: D
The dorsal branches of the proper digital nerves provide sensory innervation to the nail unit and are located dorsolateral to the nail folds. During incision and drainage procedures for paronychia, meticulous dissection is necessary to avoid iatrogenic injury to these nerves, which can lead to permanent paresthesia or dysesthesia. While the nail matrix is also vulnerable, the question specifies an incision that is 'too deep or extends too far dorsally,' which directly implicates the dorsal digital nerves.
Incorrect Options:
- A. Proper digital artery: The proper digital arteries are located more volarly and laterally/medially along the digit, not typically directly dorsal to the nail fold where a paronychia incision is made.
- B. Flexor digitorum profundus tendon: This tendon is located on the volar aspect of the digit, deep within the flexor sheath, and is not at risk during a superficial incision for paronychia unless the infection has spread significantly and neglected.
- C. Nail matrix (germinal matrix): The nail matrix is located beneath the proximal nail fold (eponychium) and extends proximally. While it is vulnerable to injury, especially with transverse incisions or aggressive subungual dissection, an incision 'too deep or extending too far dorsally' from the lateral nail fold is more likely to injure the dorsal digital nerve first.
- E. Extensor tendon: The extensor tendon is located on the dorsal aspect of the digit, but typically more centrally and proximally than the immediate nail fold area. A superficial incision for paronychia is unlikely to directly injure the extensor tendon unless it is extremely deep and misdirected.
A 28-year-old healthcare worker presents with a painful, erythematous, and swollen right index fingertip. On examination, there are multiple clear vesicles clustered around the nail fold, some with a 'dewdrop on a rose petal' appearance. The patient reports a tingling sensation preceding the onset of the lesions. There is no fluctuance. Based on the clinical presentation, which of the following is the most appropriate initial management?
Correct Answer: C
The clinical presentation of multiple clear vesicles, a 'dewdrop on a rose petal' appearance, and a preceding tingling sensation are classic signs of Herpetic Whitlow, a viral infection caused by HSV-1 or HSV-2. This condition is a crucial contraindication for incision and drainage, as surgical intervention can worsen the infection, promote viral dissemination, and lead to secondary bacterial superinfection. Management typically involves conservative measures such as warm soaks, elevation, pain control, and sometimes oral antiviral medications (e.g., acyclovir, valacyclovir) if initiated early in the course, especially in immunocompromised patients or for severe cases.
Incorrect Options:
- A. Immediate incision and drainage with a No. 11 blade: This is absolutely contraindicated for Herpetic Whitlow and would be harmful. I&D is reserved for bacterial abscesses.
- B. Oral antibiotics targeting Staphylococcus aureus: Antibiotics are ineffective against viral infections. While secondary bacterial infection can occur, the primary treatment for Herpetic Whitlow is not antibiotics.
- D. Partial nail avulsion to decompress the subungual space: This is a surgical intervention for subungual abscesses, which are bacterial. It is inappropriate and harmful for Herpetic Whitlow.
- E. Referral for urgent MRI to rule out osteomyelitis: MRI is a high-level imaging study for complex infections or suspected osteomyelitis. It is not indicated as an initial step for a clear case of Herpetic Whitlow, which is a superficial viral infection.
A 40-year-old diabetic patient presents with a severe acute paronychia involving both lateral nail folds and tracking proximally beneath the eponychium, forming a 'horseshoe' abscess. The surgeon plans for incision and drainage. Which of the following surgical techniques is most appropriate to drain the proximal subungual space while minimizing the risk of permanent nail matrix damage?
Correct Answer: B
For a horseshoe paronychia, the most appropriate and safest technique involves making bilateral longitudinal incisions on each lateral nail fold to drain the lateral abscesses. To drain the proximal subungual space without damaging the nail matrix, the eponychial fold is gently elevated off the nail plate using a blunt instrument like a Freer elevator. This allows for drainage of pus from beneath the eponychium while preserving the integrity of the nail matrix, which is crucial for preventing permanent onychodystrophy.
Incorrect Options:
- A. A transverse incision across the eponychium (H-incision): Historically described, this technique is largely abandoned due to a very high risk of permanent nail matrix damage and subsequent severe onychodystrophy.
- C. Complete nail avulsion without addressing the eponychium: While complete nail avulsion may be necessary for a large subungual abscess, it does not directly address the pus tracking beneath the eponychium in a horseshoe configuration. Furthermore, if the eponychium is not elevated, the proximal abscess may remain undrained.
- D. A single central longitudinal incision through the eponychium and nail plate: Incising the eponychium directly carries a significant risk of damaging the underlying germinal matrix, leading to permanent nail deformity. This is generally avoided.
- E. Chemical ablation of the nail matrix with phenol: This is an aggressive technique primarily used for recalcitrant chronic fungal paronychia or ingrown toenails, aiming to destroy portions of the matrix. It is not indicated for acute bacterial horseshoe paronychia and would cause severe, permanent nail deformity.
A 22-year-old male presents to the emergency department 3 days after sustaining a minor cut to his right middle finger, which has since become progressively painful, swollen, and erythematous. He now reports exquisite pain on passive extension of the digit, uniform swelling of the entire finger, and holds the finger in a semi-flexed posture. On palpation, there is tenderness along the flexor sheath. What is the most likely complication of his initial injury?
Correct Answer: C
The patient's symptoms are classic for flexor tenosynovitis, characterized by Kanavel's cardinal signs: 1) uniform swelling of the digit, 2) semi-flexed posture of the digit, 3) exquisite tenderness along the flexor sheath, and 4) pain on passive extension of the digit. This is a severe hand infection that can rapidly lead to tendon necrosis and functional loss if not promptly treated with surgical drainage and intravenous antibiotics.
Incorrect Options:
- A. Osteomyelitis of the distal phalanx: While osteomyelitis is a serious complication, it typically presents with more chronic symptoms, bone pain, and may not have the acute, specific signs of flexor tenosynovitis. X-rays would be needed for diagnosis.
- B. Septic arthritis of the DIP joint: Septic arthritis would involve pain and swelling primarily localized to the joint, with pain on both active and passive range of motion of that specific joint. While it can cause a semi-flexed posture, the uniform swelling of the entire digit and tenderness along the flexor sheath are more indicative of tenosynovitis.
- D. Deep space infection (e.g., thenar space): Deep space infections would present with swelling and tenderness localized to the specific deep space (e.g., thenar, midpalmar). While serious, they do not typically manifest with Kanavel's signs specific to the flexor sheath of a single digit.
- E. Recurrent paronychia: A paronychia is an infection of the nail folds. While the initial injury might have been a paronychia, the described progression with Kanavel's signs indicates a spread to the flexor sheath, which is a much more severe condition than a simple recurrent paronychia.
A 65-year-old male with a history of hypertension and coronary artery disease requires incision and drainage for a subungual abscess of his right ring finger. The surgeon plans to use a digital block for anesthesia. Which of the following local anesthetic agents and additives is most appropriate for this procedure?
Correct Answer: C
For digital blocks, 1% or 2% lidocaine is a commonly used and effective local anesthetic. The crucial point is that epinephrine should *never* be used in a digital block. Epinephrine causes vasoconstriction, which can lead to digital ischemia and necrosis due to the end-arterial blood supply of the digits. While bupivacaine (Marcaine) provides longer duration, lidocaine is sufficient for most paronychia I&D procedures. The absence of epinephrine is the most critical factor.
Incorrect Options:
- A. 1% Lidocaine with epinephrine: Incorrect due to the presence of epinephrine, which can cause digital ischemia.
- B. 0.5% Bupivacaine with epinephrine: Incorrect due to the presence of epinephrine.
- D. 2% Chloroprocaine with epinephrine: Incorrect due to the presence of epinephrine. Chloroprocaine is also less commonly used for digital blocks.
- E. 0.25% Marcaine with epinephrine: Incorrect due to the presence of epinephrine. Marcaine (bupivacaine) is a brand name for a long-acting anesthetic, but the epinephrine additive is the contraindication.
A 35-year-old patient presents with an acute paronychia of the left index finger. The infection appears to have originated from a hangnail that disrupted the protective seal around the nail. Which specific anatomical structure, when compromised, most commonly serves as the initial portal of entry for bacteria in acute paronychia?
Correct Answer: D
The cuticle is a thin layer of keratinized epithelium that extends from the eponychium onto the nail plate, forming a crucial protective seal against external pathogens. Disruption of this seal, often due to minor trauma like a hangnail, nail biting, or aggressive manicuring, is a common initiator of acute paronychia, allowing bacteria to enter the potential space beneath the nail fold.
Incorrect Options:
- A. Hyponychium: The hyponychium is the thickened skin beneath the free edge of the nail plate, providing a protective seal at the distal end. While it is a barrier, it is not the primary site of entry for typical paronychial infections originating from the nail folds.
- B. Nail plate: The nail plate itself is a hard, keratinized structure that is generally impervious to bacterial entry unless it is severely damaged or lifted.
- C. Nail matrix: The nail matrix is responsible for nail growth and is located beneath the eponychium. It is not a portal of entry but rather a structure vulnerable to damage if infection spreads or during improper surgical intervention.
- E. Sterile matrix: The sterile matrix is the distal portion of the nail bed that supports the nail plate. Like the germinal matrix, it is not a primary portal of entry for infection.
A 19-year-old college student presents with a 24-hour history of localized erythema, mild swelling, and tenderness along the lateral nail fold of his right ring finger after aggressively picking a hangnail. There is no visible pustule or fluctuance. He denies fever or chills. What is the most appropriate initial management for this patient?
Correct Answer: C
This patient presents with early cellulitis without evidence of abscess formation (no fluctuance or visible pustule) and no signs of systemic involvement. In such mild, early presentations of acute paronychia, non-operative management is indicated. This includes warm soaks (to promote drainage and reduce inflammation), elevation (to reduce swelling), and empiric oral antibiotics, typically targeting common skin flora like Staphylococcus aureus (e.g., cephalexin or clindamycin).
Incorrect Options:
- A. Immediate incision and drainage of the lateral nail fold: I&D is indicated for abscess formation. Performing an I&D on pure cellulitis is unnecessary and potentially harmful, creating an open wound without pus to drain.
- B. Urgent referral for MRI to assess for deep space infection: MRI is a high-level imaging study reserved for complex or chronic cases with suspicion of deeper infection. It is not indicated for early, uncomplicated cellulitis.
- D. Complete nail avulsion to prevent subungual abscess formation: Nail avulsion is a surgical procedure for subungual abscesses or severe nail dystrophy. It is an overly aggressive and inappropriate intervention for early cellulitis.
- E. Observation only, as it is likely to resolve spontaneously: While some very mild cases might resolve, given the bacterial etiology and potential for progression, active management with warm soaks and antibiotics is prudent to prevent abscess formation or spread of infection.
A 50-year-old patient underwent incision and drainage for a severe, neglected acute paronychia that had tracked proximally and distally, requiring partial nail avulsion and extensive debridement. Six months post-operatively, the patient complains of persistent pain and significant deformity of the new nail plate, which is thickened, discolored, and ridged. This complication is most likely due to iatrogenic injury to which of the following structures during the initial surgery?
Correct Answer: D
The nail matrix, specifically the germinal matrix, is responsible for producing 90% of the nail plate. Injury to the nail matrix during surgical intervention (e.g., aggressive debridement, improper incisions, or trauma during nail avulsion) can lead to permanent onychodystrophy, characterized by a deformed, thickened, discolored, or ridged nail plate. The description of the new nail plate's appearance directly points to damage to the nail-producing unit.
Incorrect Options:
- A. Proper digital artery: Injury to the proper digital artery would lead to vascular compromise, potentially resulting in tissue necrosis or delayed healing, but not directly to nail plate deformity in this manner.
- B. Dorsal digital nerve: Injury to the dorsal digital nerve would result in sensory deficits (paresthesia, dysesthesia) in the nail unit area, not directly in nail plate deformity.
- C. Flexor digitorum profundus tendon: Injury to the flexor digitorum profundus tendon would result in loss of active DIP joint flexion and potential tendon rupture or adhesion, not nail plate deformity.
- E. Hyponychium: The hyponychium is the skin beneath the free edge of the nail. While important for sealing, its injury would not typically cause the described severe nail plate dystrophy, which originates from the matrix.
A 70-year-old male with poorly controlled diabetes presents with a chronic paronychia of his great toe, which has been present for several months. He has significant pain, erythema, and swelling, and plain radiographs show cortical irregularity and periosteal reaction of the distal phalanx. Which of the following is the most appropriate initial imaging study to confirm the suspected diagnosis?
Correct Answer: C
The patient's history of chronic paronychia, poorly controlled diabetes (a risk factor for osteomyelitis), and the clinical signs of pain, erythema, and swelling, combined with the suspicion of bone involvement, make plain radiographs (X-rays) the most appropriate initial imaging study. X-rays are readily available, inexpensive, and can effectively demonstrate signs of osteomyelitis such as cortical irregularity, periosteal reaction, and bone erosion, especially in chronic infections. The question states that plain radiographs 'show cortical irregularity and periosteal reaction,' indicating that X-rays have already provided diagnostic information and are the correct initial step for suspected osteomyelitis.
Incorrect Options:
- A. Magnetic Resonance Imaging (MRI): MRI is highly sensitive for osteomyelitis and can detect early changes not visible on X-rays. However, it is a more expensive and less accessible study, typically reserved for cases where X-rays are equivocal or when the extent of soft tissue involvement needs to be precisely delineated. It is not the *initial* imaging study when osteomyelitis is suspected.
- B. Computed Tomography (CT) scan: CT scans are excellent for evaluating cortical bone detail and complex fractures but are less sensitive than MRI for early osteomyelitis and expose the patient to higher radiation. It is not the initial imaging study for suspected osteomyelitis.
- D. Ultrasound: Ultrasound can be useful for identifying and localizing fluid collections (abscesses) in soft tissues but is not the primary imaging modality for diagnosing osteomyelitis, although it can sometimes show periosteosteal fluid or cortical irregularities.
- E. Bone scintigraphy: Bone scintigraphy (bone scan) is very sensitive for detecting increased bone turnover associated with infection but lacks specificity and anatomical detail. It is often used when osteomyelitis is suspected but X-rays are negative, or to assess multifocal involvement, but it is not the initial imaging study.
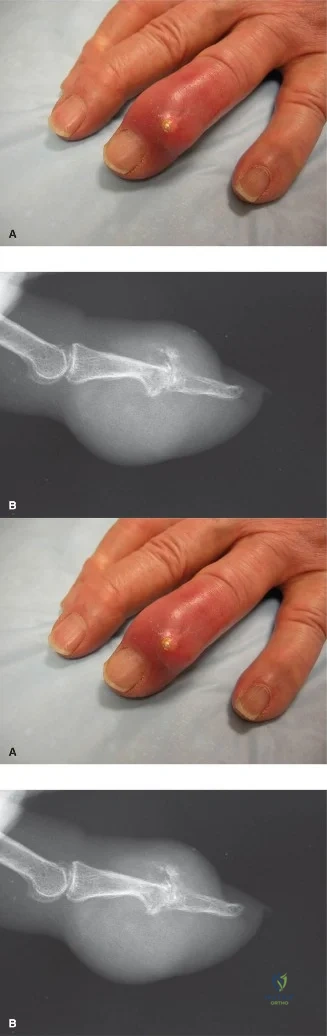
An 82-year-old male presents with acute onset of severe pain, swelling, and erythema in his right dominant hand, primarily affecting the MCP and PIP joints. He has a history of hypertension, renal insufficiency (eGFR 45 mL/min/1.73m2), and takes a thiazide diuretic. He denies any recent trauma or fever. Physical examination reveals warm, exquisitely tender, swollen joints with overlying shiny, erythematous skin. There are also several firm, non-tender subcutaneous nodules on the dorsal aspect of his hand and forearm, which he states have been present for years. Given the high suspicion for an acute gout flare in the setting of chronic tophaceous disease, an arthrocentesis is performed on the most inflamed MCP joint. The synovial fluid analysis is crucial for definitive diagnosis. Which of the following findings, as depicted in the image, is considered the gold standard for confirming the diagnosis of gout?
Correct Answer: C
The case highlights an elderly patient with an atypical presentation of gout in the hand, complicated by comorbidities. The definitive diagnostic test for gout, as emphasized in the teaching case and depicted in the image, is the identification of negatively birefringent, needle-shaped monosodium urate (MSU) crystals under polarized light microscopy in synovial fluid. This finding confirms the presence of MSU crystals, which are pathognomonic for gout.
Option A is incorrect: While an elevated serum uric acid (SUA) level supports the diagnosis of hyperuricemia, it is not definitive for an acute gout flare, as SUA can be normal or even low during an acute attack. Furthermore, hyperuricemia alone does not equate to gout.
Option B is incorrect: The 'double contour sign' on musculoskeletal ultrasound is highly suggestive of MSU crystal deposition on articular cartilage and is a valuable diagnostic tool, especially for early detection. However, it is an imaging finding and not the 'gold standard' definitive microscopic identification of the crystals themselves.
Option D is incorrect: Radiographic evidence of 'punched-out' erosions with sclerotic margins and 'overhanging edges' (Martel sign) is characteristic of chronic tophaceous gout. However, these changes are often absent in early disease and represent a consequence of long-standing crystal deposition, not the definitive acute diagnostic finding.
Option E is incorrect: A synovial fluid white blood cell (WBC) count of 60,000 cells/mm³ with 90% neutrophils is indicative of an inflammatory process, which is consistent with an acute gout flare. However, this finding is non-specific and can also be seen in septic arthritis or other inflammatory arthropathies. Without crystal identification, it cannot definitively differentiate gout from these other conditions.
A 75-year-old female presents with a 6-month history of progressive pain and swelling in her left wrist and multiple finger joints. She reports numbness and tingling in her thumb, index, and middle fingers, worse at night. Her medical history includes well-controlled diabetes, hypertension, and chronic kidney disease (Stage 3). Physical examination reveals diffuse swelling and tenderness over the wrist and MCP joints, with palpable firm, non-tender nodules on the dorsal aspect of the PIP joints. Phalen's and Tinel's signs are positive at the wrist. Plain radiographs show preserved joint spaces but demonstrate several 'punched-out' erosions with sclerotic margins in the carpal bones and adjacent to the PIP joints. Given the patient's age and presentation, which of the following is the MOST likely atypical feature of gout in this elderly patient?
Correct Answer: D
The teaching case explicitly states that gout's presentation in the elderly is often atypical, polyarticular, and commonly affects the upper extremities, mimicking various inflammatory and degenerative arthropathies. Furthermore, tophi can expand within confined anatomical spaces, such as the carpal tunnel, leading to compression neuropathies (e.g., median nerve compression), which is indicated by the patient's numbness and tingling and positive Phalen's/Tinel's signs.
Option A is incorrect: Monoarticular involvement of the first MTP joint is the classic presentation of gout, but it is less common in the elderly, who often have atypical, polyarticular involvement.
Option B is incorrect: The presence of palpable tophi is a hallmark of chronic tophaceous gout, and the patient in the vignette has 'palpable firm, non-tender nodules,' which are consistent with tophi. Their absence would be atypical, but their presence is expected in chronic disease.
Option C is incorrect: Radiographic 'punched-out' erosions with sclerotic margins are characteristic findings of chronic tophaceous gout, as described in the case. While they may be absent in early disease, their presence is a typical feature of established tophaceous gout, not an atypical one.
Option E is incorrect: While NSAIDs are a first-line treatment for acute gout flares, the response can be variable, especially in elderly patients with comorbidities like renal insufficiency, which may limit their use. A rapid response is not a defining atypical feature; rather, the presentation itself is atypical.
A 68-year-old male with a long history of uncontrolled gout presents with increasing pain and functional limitation in his right hand. He has multiple large, firm, subcutaneous nodules over his MCP and PIP joints. He reports difficulty with fine motor tasks and occasional skin breakdown over one of the nodules. His rheumatologist has optimized his urate-lowering therapy (ULT), and his serum uric acid (SUA) has been stable at 4.8 mg/dL for the past 6 months. Physical examination confirms significant mass effect from the tophi, limiting joint range of motion. There is a small, non-healing ulceration over a large tophus on the dorsal aspect of his index finger. Which of the following is the MOST appropriate indication for surgical intervention in this patient?
Correct Answer: D
The teaching case clearly outlines indications for surgical intervention in tophaceous gout. Significant functional impairment due to large tophi (mass effect limiting range of motion) and skin ulceration (or impending rupture) are explicit indications for surgery. The patient's optimized ULT and stable SUA level make him a suitable candidate for elective surgery to address these complications.
Option A is incorrect: While cosmetic deformity can be a secondary indication, the case states it is generally a secondary indication, and only if functional impairment is also present or imminent. In this patient, functional impairment and ulceration are primary concerns.
Option B is incorrect: The patient's SUA is stable at 4.8 mg/dL, which is below the target of 5 mg/dL for severe tophaceous gout, indicating controlled hyperuricemia. Uncontrolled hyperuricemia would be a contraindication for elective surgery, not an indication.
Option C is incorrect: Surgical intervention is generally contraindicated during an acute inflammatory flare, as it can exacerbate the inflammation. The vignette does not describe an acute flare, but rather chronic issues with functional impairment and ulceration.
Option E is incorrect: Surgical intervention is not a method for prophylaxis against future gout flares. Long-term urate-lowering therapy (ULT) and anti-inflammatory prophylaxis (e.g., colchicine) are the cornerstones of flare prevention.
A 55-year-old male presents with chronic pain and swelling in his right hand. He has a history of recurrent gout flares, but has been non-adherent to his urate-lowering therapy (ULT). Plain radiographs of his hand are obtained. Based on the information provided in the teaching case, which of the following radiographic findings is MOST characteristic of chronic tophaceous gout?
Correct Answer: D
The teaching case specifically describes the characteristic radiographic findings of chronic tophaceous gout: 'Over time, chronic tophaceous deposits within bone lead to characteristic "punched-out" erosions, often with sclerotic margins and an "overhanging edge" sign on plain radiographs, which is highly suggestive of gout.' These erosions can be extra-articular or intra-articular and often occur adjacent to an intact joint space until very late stages.
Option A is incorrect: Diffuse joint space narrowing and osteophytes are characteristic of osteoarthritis (OA).
Option B is incorrect: Central erosions with subchondral cysts and joint space narrowing can be seen in various arthropathies, including rheumatoid arthritis, but are not the classic description for gout.
Option C is incorrect: Periarticular osteopenia and symmetric joint space narrowing are classic radiographic features of rheumatoid arthritis (RA).
Option E is incorrect: While some soft tissue calcifications can occur, the specific 'punched-out' erosions with sclerotic margins and overhanging edges are the most characteristic and diagnostic radiographic feature for gout, distinguishing it from other crystal arthropathies like CPPD (which often shows chondrocalcinosis).
A 70-year-old patient with a known history of severe tophaceous gout is scheduled for surgical debulking of a large, symptomatic tophus on the dorsal aspect of his wrist that is causing significant functional impairment. He is currently experiencing an acute gout flare in his knee, with severe pain and swelling, and his serum uric acid (SUA) is 11 mg/dL. He also has a history of poorly controlled diabetes and is on warfarin for atrial fibrillation. Which of the following factors represents the MOST significant contraindication to proceeding with elective surgical intervention at this time?
Correct Answer: C
The teaching case explicitly lists 'Acute Gout Flare' and 'Uncontrolled Hyperuricemia' as contraindications for surgical intervention. 'Surgical intervention is generally contraindicated during an acute inflammatory flare. Surgery can exacerbate the inflammatory response and potentially trigger a new flare. Medical management (NSAIDs, colchicine, corticosteroids) should be optimized to quiescent the inflammation before elective surgery.' Additionally, 'elective surgical intervention should ideally be deferred until serum uric acid (SUA) levels are adequately controlled... High SUA levels increase the risk of post-operative flares and continued crystal deposition.' The patient's acute knee flare and SUA of 11 mg/dL clearly fall under these contraindications.
Option A is incorrect: While poorly controlled diabetes is a significant medical comorbidity that increases surgical risk, it is listed as a 'Significant Medical Comorbidity' that requires thorough pre-operative workup and risk-benefit analysis, rather than an absolute contraindication that would immediately halt an elective procedure if other factors were optimized.
Option B is incorrect: Warfarin use indicates a coagulopathy, which is a contraindication if uncorrected, due to increased risk of hematoma. However, coagulopathies can often be managed pre-operatively (e.g., bridging therapy) to mitigate risk. The acute flare and uncontrolled hyperuricemia are more direct and absolute contraindications for elective surgery in this context.
Option D is incorrect: While advanced age (70 years old) is associated with increased comorbidities and surgical risk, it is not an absolute contraindication in itself. Many elderly patients undergo successful elective surgeries after appropriate medical clearance.
Option E is incorrect: The location of the tophus on the dorsal wrist does not represent a contraindication to surgery; rather, it is the site of the pathology requiring intervention.
A 60-year-old male presents with chronic hand pain and progressive numbness in the distribution of the median nerve. He has a long history of gout, with multiple tophi palpable around his wrist. His rheumatologist has confirmed stable urate levels. Surgical decompression of the median nerve and excision of compressive tophi are planned. During pre-operative planning, the surgeon considers various imaging modalities to precisely map the extent of crystal deposition and its relationship to neurovascular structures. Which advanced imaging modality is specifically highlighted in the teaching case for its ability to identify and quantify monosodium urate (MSU) crystal deposits based on their unique attenuation properties?
Correct Answer: C
The teaching case specifically states: 'Dual-energy CT (DECT) can specifically identify and quantify MSU crystal deposits based on their unique attenuation properties, proving highly valuable for diagnostic confirmation, mapping crystal burden, and monitoring treatment response, especially in atypical presentations or when aspiration is difficult.'
Option A is incorrect: Plain radiographs are the initial imaging choice but primarily show bone erosions and soft tissue swelling, not direct crystal identification or quantification.
Option B is incorrect: Musculoskeletal ultrasound is highly sensitive for detecting early changes like the 'double contour sign' and identifying non-palpable tophi, and is useful for guiding aspiration. However, it does not quantify MSU crystal deposits based on unique attenuation properties in the same way DECT does.
Option D is incorrect: MRI is useful for assessing soft tissue involvement, nerve compression, and synovial thickening, and differentiating gouty inflammation from other pathologies. Tophi have variable signal intensity on MRI, but MRI does not specifically identify or quantify MSU crystals based on their unique attenuation properties.
Option E is incorrect: Standard CT provides detailed assessment of bone erosions and soft tissue tophi but lacks the specific material differentiation capabilities of DECT for MSU crystals.
A 72-year-old male undergoes surgical excision of a large tophus from his right wrist, which was causing significant mass effect and median nerve compression. The procedure involved meticulous dissection and removal of the chalky white tophaceous material, followed by carpal tunnel release. Post-operatively, the patient is started on low-dose colchicine prophylaxis. Despite this, on post-operative day 3, he develops acute onset of severe pain, swelling, and erythema localized to the surgical site, with no signs of infection. His temperature is normal. Which of the following is the MOST likely complication and its primary management strategy?
Correct Answer: C
The teaching case explicitly lists 'Acute Post-operative Flare' as a common complication (5-20% incidence). It states: 'Prevention is Key: Prophylaxis with low-dose colchicine (0.5-0.6 mg BID) or NSAIDs initiated pre-operatively and continued for several weeks post-operatively. Treatment: Oral corticosteroids (e.g., prednisone 0.5 mg/kg/day for 5-10 days, then taper) are often preferred over NSAIDs due to potential renal issues in elderly. Colchicine can be restarted.' The patient's symptoms (acute pain, swelling, erythema localized to the surgical site, no signs of infection, normal temperature) are classic for a post-operative gout flare, even with prophylaxis.
Option A is incorrect: While infection is a possible complication, the absence of fever and other systemic signs of infection, along with the specific description of 'no signs of infection,' makes an acute gout flare more likely in this context. Infection would typically present with fever, purulent discharge, and worsening pain that is not responsive to anti-inflammatory measures.
Option B is incorrect: Iatrogenic nerve injury would typically present with new or worsened neurological deficits (e.g., motor weakness, sensory loss), not primarily with acute inflammatory signs like erythema and swelling at the surgical site.
Option D is incorrect: Hematoma formation would present with swelling and potentially ecchymosis, but typically not with the intense erythema and inflammatory signs characteristic of a gout flare. While hematoma can occur, the clinical picture points more strongly to inflammation.
Option E is incorrect: Tendon rupture would present with loss of active motion or specific functional deficits related to the affected tendon, not primarily with acute inflammatory signs like erythema and swelling.
A 65-year-old male with a history of chronic tophaceous gout in his hands is undergoing pre-operative evaluation for excision of a large, ulcerated tophus on his dominant index finger. He has multiple comorbidities, including renal impairment (eGFR 40 mL/min/1.73m2) and hypertension. During the pre-operative workup, the orthopedic surgeon reviews the patient's laboratory results. Which of the following lab findings is MOST critical to assess for long-term management and to minimize the risk of post-operative complications related to gout?
Correct Answer: C
The teaching case emphasizes the importance of 'Uncontrolled Hyperuricemia' as a contraindication for elective surgery and states: 'elective surgical intervention should ideally be deferred until serum uric acid (SUA) levels are adequately controlled by urate-lowering therapy (typically below 6 mg/dL, or below 5 mg/dL in severe tophaceous gout). High SUA levels increase the risk of post-operative flares and continued crystal deposition.' Therefore, assessing and optimizing SUA is critical for long-term management and minimizing post-operative complications.
Option A is incorrect: CBC is important to assess for anemia or leukocytosis (indicating infection/inflammation), but it is not the most critical for long-term gout management or specific post-operative gout complications.
Option B is incorrect: ESR is a non-specific inflammatory marker, useful during acute flares or infection, but not the primary lab for long-term gout control.
Option D is incorrect: A coagulation profile is essential, especially if extensive dissection is anticipated, to assess bleeding risk. However, while important for surgical safety, it is not the most critical for the long-term management of gout itself or the specific risk of post-operative gout flares/recurrence.
Option E is incorrect: CRP is another non-specific inflammatory marker, similar to ESR, and not the primary lab for long-term gout control.
A 48-year-old male presents with a 3-month history of progressive swelling and pain in his right index finger, accompanied by a 'catching' sensation during flexion. He has a history of gout, but has been inconsistent with his medication. Physical examination reveals a palpable nodule at the A1 pulley of the index finger, with tenderness and triggering. An ultrasound confirms a tophaceous deposit within the flexor tendon sheath. Given this presentation, which anatomical structure is MOST likely affected by the tophus, leading to the described symptoms?
Correct Answer: C
The teaching case states: 'The flexor and extensor tendon sheaths are common sites for tophus formation, often leading to tenosynovitis, trigger digit, or even spontaneous tendon rupture.' The patient's symptoms of a 'catching' sensation during flexion, a palpable nodule at the A1 pulley, and ultrasound confirmation of a tophaceous deposit within the flexor tendon sheath are classic for a trigger digit caused by tophaceous tenosynovitis.
Option A is incorrect: While DIP joints can be affected by gout, involvement of the synovium here would typically cause joint pain and swelling, not a 'catching' sensation indicative of tendon pathology.
Option B is incorrect: MCP joint capsule involvement would lead to joint pain, swelling, and reduced range of motion, but not the specific triggering phenomenon associated with tendon sheaths.
Option D is incorrect: Periarticular ligaments of the PIP joint would primarily affect joint stability and cause localized pain, not a trigger digit.
Option E is incorrect: Subchondral bone involvement would lead to erosions and pain, but not the mechanical obstruction of tendon gliding that causes triggering.
A 78-year-old female with a history of chronic tophaceous gout in her hands undergoes surgical debulking of a large tophus on her left middle finger. The procedure is uneventful. Post-operatively, the patient is placed in a protective splint. During the rehabilitation phase, the hand therapist emphasizes early and aggressive mobilization. Which of the following is the MOST critical aspect of long-term post-operative management to prevent recurrence of tophi and progressive joint destruction?
Correct Answer: C
The teaching case explicitly states under 'Advanced Phase' of rehabilitation: 'Medical Management Reinforcement: Crucial to emphasize continued adherence to urate-lowering therapy and regular follow-up with the rheumatologist to prevent future flares and crystal deposition. This is paramount to surgical success and long-term joint health.' ULT is the cornerstone of preventing recurrence and progression of gout.
Option A is incorrect: While initial protection with a splint is necessary, prolonged immobilization is a risk factor for joint stiffness and reduced range of motion, as mentioned in the complications section. Early, guided mobilization is crucial for rehabilitation.
Option B is incorrect: High-dose NSAIDs are used for acute flare management, but their long-term use is often limited by side effects, especially in the elderly with comorbidities like renal impairment. They are not the primary strategy for preventing tophi recurrence.
Option D is incorrect: Aggressive passive range of motion exercises immediately post-op can jeopardize wound healing and surgical repairs, especially if tendon or joint capsule repairs were performed. Rehabilitation progresses gradually from protected AROM to PROM.
Option E is incorrect: While revision surgery for symptomatic residual tophi may be considered, it is not the primary long-term management strategy for prevention. The goal is to prevent new tophi formation and dissolve existing ones through medical management.
A 62-year-old male presents with acute, severe pain and swelling in his right wrist and multiple MCP joints. He has a history of hyperuricemia but has never been formally diagnosed with gout. His symptoms are accompanied by warmth and erythema. Given the inflammatory nature of his presentation, the orthopedic surgeon considers a differential diagnosis that includes septic arthritis, rheumatoid arthritis, and calcium pyrophosphate deposition disease (CPPD), in addition to gout. An arthrocentesis is performed on the most inflamed MCP joint. The synovial fluid analysis reveals a WBC count of 75,000 cells/mm³ with 92% neutrophils. Gram stain is negative. Which of the following additional findings from the synovial fluid analysis, as shown in the image, would definitively confirm a diagnosis of gout and rule out the other inflammatory conditions?
Correct Answer: B
The teaching case explicitly states that 'Synovial Fluid Analysis: This is the gold standard for definitive diagnosis... Polarized light microscopy: Crucial for identifying negatively birefringent, needle-shaped MSU crystals. This is the definitive diagnostic test.' The image provided also depicts these classic crystals. This finding definitively confirms gout and differentiates it from septic arthritis (ruled out by negative Gram stain and culture), CPPD (which has positively birefringent crystals), and rheumatoid arthritis (which lacks specific crystal findings).
Option A is incorrect: Positively birefringent, rhomboid-shaped crystals are characteristic of Calcium Pyrophosphate Deposition Disease (CPPD), also known as pseudogout, not gout.
Option C is incorrect: While the absence of bacteria on culture helps rule out septic arthritis, it does not definitively confirm gout, as other sterile inflammatory arthropathies (like RA or CPPD) would also have negative cultures.
Option D is incorrect: A low synovial fluid glucose level can be seen in septic arthritis or severe inflammatory conditions, but it is not specific for gout and does not definitively confirm the diagnosis.
Option E is incorrect: A high synovial fluid lactate level can be indicative of infection or severe inflammation, but it is not specific for gout and does not definitively confirm the diagnosis.
A 32-year-old construction worker presents to the emergency department approximately 45 minutes after sustaining a high-energy crush injury to his right hand. Clinical examination reveals significant swelling, ecchymosis, and deformity, particularly over the dorsum. Two small, punctate lacerations, each less than 1 cm, are noted over the dorsum of the hand, one proximal to the 4th metacarpal head and another over the mid-shaft of the 5th metacarpal. X-rays confirm multiple displaced metacarpal fractures. Based on the initial presentation, what is the most appropriate immediate management step for the open injury component?
Correct Answer: B
The presence of small punctate lacerations communicating with the fracture sites classifies these as Gustilo-Anderson Type I open fractures. According to the case, 'Open fractures mandate surgical debridement and irrigation to prevent infection, often combined with stable internal fixation.' Therefore, the most appropriate immediate management step is formal irrigation and debridement in the operating room, along with the administration of intravenous broad-spectrum antibiotics. Delaying debridement (Option E) increases the risk of infection. Oral antibiotics (Option A) are insufficient for an open fracture, and primary closure without debridement (Option C) is contraindicated. An MRI (Option D) is not an immediate priority for acute open fracture management and debridement.
A 32-year-old male sustains a high-energy crush injury to his right hand. Initial radiographs are obtained upon presentation to the emergency department.
Based on the provided PA radiograph and the clinical description, which of the following statements accurately describes the fracture characteristics of the 5th metacarpal?

Correct Answer: C
The case explicitly states that the 5th metacarpal presented with 'A highly unstable, spiral shaft fracture of the right fifth metacarpal was observed, with substantial dorsal angulation (approximately 45 degrees), 7 mm of shortening, and significant rotational displacement, manifesting as overlap of the distal shaft fragment over the 4th metacarpal on the PA view.' The provided radiograph clearly shows the spiral nature, significant shortening, and overlap indicative of rotational deformity. Options A, B, D, and E describe different fracture patterns or less severe displacement that do not match the detailed description or the visual evidence for the 5th metacarpal.
Considering the patient's clinical presentation, radiographic findings (including the initial PA radiograph shown in the previous question), and the high-energy mechanism, which of the following is the MOST compelling indication for operative intervention (ORIF) for this patient's multiple metacarpal fractures?
Correct Answer: C
While all options except E (past medical history) are factors influencing surgical decision-making, the most compelling indication for operative fixation to restore function and prevent long-term disability is significant rotational malalignment. The case states, 'Rotational malunion is one of the most debilitating complications of metacarpal fractures, leading to significant functional impairment (finger overlap during gripping) that is poorly tolerated and extremely difficult to revise. This is an absolute indication for operative fixation.' Option B (open fracture) is an absolute indication for surgical debridement and irrigation, but the rotational malalignment is the primary driver for *fixation* to prevent functional impairment. Options A (age/occupation) and D (10 degrees angulation of 2nd MC) are contributing factors but not as critical as rotational deformity, which is poorly tolerated in any metacarpal.
During the initial clinical examination of the patient's right hand, it was noted that the 5th digit appeared to be scissoring over the 4th digit in gentle flexion. This specific finding is of critical importance in the management of metacarpal fractures because:
Correct Answer: C
The case explicitly highlights the importance of this finding: 'The normal cascade of the digits was disrupted, with the 5th digit appearing to scissoring over the 4th digit in gentle flexion, indicative of malrotation.' It further emphasizes, 'Rotational malunion is one of the most debilitating complications of metacarpal fractures, leading to significant functional impairment (finger overlap during gripping) that is poorly tolerated and extremely difficult to revise. This is an absolute indication for operative fixation.' Therefore, scissoring is a critical sign of rotational malalignment requiring surgical correction. Options A, B, D, and E are incorrect; scissoring is not indicative of tendon injury, carpal ligament injury, or compartment syndrome, nor does it resolve spontaneously.
Following initial radiographs, a Computed Tomography (CT) scan of the right hand was performed. Given the high-energy mechanism, suspicion of open fractures, and multiple comminuted fractures, the CT scan was indicated. Which of the following pieces of information was the CT scan LEAST likely to provide that was crucial for surgical planning in this specific case?
Correct Answer: E
The case details the benefits of the CT scan: 'The CT scan confirmed the complex fracture patterns identified on X-ray, providing superior detail regarding comminution and displacement... Coronal and sagittal reconstructions confirmed a stable transverse fracture, with minimal comminution... Axial and sagittal views better delineated the degree of dorsal comminution... No intra-articular extension was found... The spiral nature and multiplanar displacement of the 5th metacarpal fracture were precisely mapped... The carpal bones and CMC joints were found to be intact, ruling out associated carpal fractures or major ligamentous injuries.' However, the case explicitly states under 'MRI Indications' that 'an MRI might be considered in cases with suspected significant ligamentous injury (e.g., sagittal band rupture, CMC ligamentous instability), occult tendon injury, or if neurovascular compromise was equivocal after initial workup.' CT is excellent for bone detail but has limited utility for subtle tendon ruptures or neurovascular compromise compared to MRI or direct clinical assessment.
During the open reduction and internal fixation of the multiple metacarpal fractures, a single dorsal longitudinal incision was utilized to expose the 2nd, 4th, and 5th metacarpal shafts. Meticulous care was taken to identify and protect specific anatomical structures. Which of the following structures is MOST at risk of iatrogenic injury during this dorsal approach, particularly when retracting soft tissues to expose the metacarpals?
Correct Answer: C
The case specifically mentions, 'Meticulous care was taken to identify and protect the dorsal sensory nerves (branches of the radial and ulnar nerves) and extensor tendons.' These superficial sensory nerves are located dorsally and are highly susceptible to injury during dorsal approaches to the metacarpals due to their proximity to the incision and retraction. The median nerve (Option A), ulnar artery (Option B), deep palmar arch (Option D), and flexor digitorum profundus tendons (Option E) are all located on the volar aspect of the hand or deeper within the palm and are not typically at direct risk during a dorsal metacarpal approach.
The surgical intervention involved open reduction and internal fixation of the 2nd, 4th, and 5th metacarpal fractures using 1.5 mm low-profile locking plates. The 4th metacarpal fracture was described as a short oblique, comminuted shaft fracture. Which of the following statements accurately describes the fixation strategy employed for this specific fracture pattern?
Correct Answer: B
The case explicitly details the fixation strategy for the 4th metacarpal: 'The short oblique, comminuted shaft fracture required careful reduction. A 1.5 mm low-profile locking plate (6 holes) was applied. Due to the comminution, the plate acted as a bridging plate, and locking screws were strategically placed. One lag screw was applied through the plate for interfragmentary compression of the oblique component, augmenting stability.' This approach combines the benefits of bridging for comminution with a lag screw for interfragmentary compression of the oblique component. Options A, C, D, and E describe different fixation methods not used or appropriate for this specific fracture as described in the case.
Immediately following open reduction and internal fixation, the patient's right hand was placed in a well-padded bulky dressing incorporating a dorsal protective plaster splint. The splint maintained the wrist in 20-30 degrees of extension, MCP joints in 70-90 degrees of flexion, and IP joints in full extension. What is the primary rationale for positioning the MCP joints in 70-90 degrees of flexion (the "position of safety")?
Correct Answer: C
The case states: 'A well-padded bulky dressing incorporating a dorsal protective plaster splint... maintaining the wrist in 20-30 degrees of extension, MCP joints in 70-90 degrees of flexion, and IP joints in full extension (the "position of safety"). This position protects the repair while preventing MCP collateral ligament shortening.' When the MCP joints are extended, the collateral ligaments are lax and can shorten, leading to stiffness in extension. Flexing the MCP joints tightens these ligaments, maintaining their length and preventing contracture, thus preserving MCP joint mobility. Options A, B, D, and E are incorrect rationales for this specific splinting position.
Despite successful surgical intervention and stable fixation, a critical pitfall in the management of multiple metacarpal fractures, particularly those involving the 5th metacarpal, is inadequate correction of rotational deformity. If this complication were to occur and go uncorrected, what would be the MOST likely functional consequence for the patient?
Correct Answer: C
The case explicitly identifies 'Inadequate Rotational Correction' as 'The most common and functionally disabling complication.' It further states, 'Often subtle, but evident on clinical exam (scissoring of fingers during flexion). A malunited rotation is poorly tolerated and extremely difficult to revise.' Rotational malunion causes the affected finger to overlap or scissor with an adjacent finger during flexion, severely impairing grip function. While other complications like angulation (A), shortening (B), nonunion (D), or CRPS (E) can occur, scissoring due to rotational malunion is the most direct and debilitating functional consequence of uncorrected rotational deformity.
The patient undergoes post-operative radiographic assessment following open reduction and internal fixation of his multiple metacarpal fractures.
Based on the provided post-operative PA radiograph, which of the following statements is the MOST accurate assessment of the surgical outcome?

Correct Answer: C
The case describes the post-operative radiograph as 'Post-operative PA radiograph demonstrating anatomical reduction and stable internal fixation of the 2nd, 4th, and 5th metacarpal fractures with low-profile locking plates and screws.' Visually, the image confirms that the metacarpals are well-aligned, their lengths are restored, and the plates and screws are appropriately placed and intact. There is no evidence of persistent angulation (A), significant shortening (B), hardware failure (D), or intra-articular extension (E) on this PA view. The surgical goal of anatomical reduction and stable fixation appears to have been achieved.
What is the most appropriate initial management and empiric antibiotic of choice?
What is the most likely diagnosis?
What is the maximum acceptable volar angulation for this fracture before reduction or surgical intervention is definitively indicated to prevent functional deficit?
Radiographs demonstrate well-defined periarticular erosions with sclerotic overhanging margins ('Martel sign') and preserved joint spaces. What is the most likely composition of these soft tissue masses?
None
