Diagnose Posterior Labrum Tear: Your Interactive Ortho Case

Key Takeaway
Looking for accurate information on Diagnose Posterior Labrum Tear: Your Interactive Ortho Case? A **posterior labrum tear** involves damage to the cartilage rim at the back of the shoulder socket, frequently occurring after a posterior shoulder dislocation. This injury typically happens when the shoulder is flexed, adducted, and internally rotated under trauma. It can cause persistent pain, a sensation of instability, and may include a reverse Bankart lesion, where a bone fragment avulses from the posterior glenoid.
Patient Presentation and History
The patient is a 22 year old male collegiate American football offensive lineman presenting to the orthopedic clinic with a chief complaint of chronic deep posterior shoulder pain and a sensation of instability in his dominant right shoulder. The patient reports an insidious onset of symptoms over the past two seasons, which was recently acutely exacerbated during a blocking drill. He describes the mechanism of the acute exacerbation as an axial load applied to his right arm while it was positioned in forward flexion, adduction, and internal rotation. Following this specific event, he experienced a sharp, tearing sensation in the posterior aspect of the glenohumeral joint, accompanied by transient paresthesias radiating down the lateral aspect of his arm, which resolved within minutes.
He denies any frank dislocation events requiring closed reduction in the emergency department. However, he endorses multiple episodes of subluxation, colloquially described by the patient as a dead arm sensation, particularly when executing bench press exercises or engaging opposing defensive linemen.
His past medical history is unremarkable. There is no history of generalized ligamentous laxity, connective tissue disorders, or prior surgical interventions on either upper extremity. He denies any systemic symptoms, night sweats, or unexplained weight loss. Prior conservative management initiated by the athletic training staff included a six week course of non steroidal anti inflammatory drugs and a physical therapy regimen focused on periscapular strengthening, which provided only transient relief. The patient is currently unable to participate in contact drills due to apprehension and mechanical pain.
Clinical Examination Findings
A comprehensive orthopedic examination of the bilateral upper extremities was performed, with the contralateral left shoulder serving as a baseline for comparison.
Inspection and Palpation
Upon inspection, the shoulder girdle demonstrates normal contour without evidence of gross muscular atrophy in the supraspinatus or infraspinatus fossae, clinically decreasing the suspicion for advanced suprascapular nerve compression. Evaluation of scapulothoracic motion reveals mild scapular dyskinesia, specifically a Type II pattern with prominence of the entire medial border during the descent phase of forward elevation. Palpation elicits distinct point tenderness along the posterior joint line, just inferior to the posterolateral angle of the acromion. The acromioclavicular joint and the long head of the biceps tendon are non tender to palpation.
Range of Motion Assessment
Active and passive range of motion are symmetrically preserved in forward elevation and external rotation with the arm at the side. However, internal rotation at 90 degrees of shoulder abduction is limited by pain, measuring 45 degrees on the affected right side compared to 65 degrees on the contralateral side. Cross body adduction reproduces deep posterior shoulder pain.
Provocative Special Testing
Provocative testing for posterior instability and labral pathology is highly positive. The Jerk test is positive, eliciting a palpable clunk and reproducing the patient's concordant pain as the humerus is axially loaded and moved horizontally across the body. The Kim test is similarly positive, demonstrating sudden onset posterior shoulder pain with a concurrent clunk as an axial load is applied to the elbow while the arm is elevated 90 degrees and diagonally elevated.
The Load and Shift test demonstrates Grade 2 posterior translation, with the humeral head translating over the posterior glenoid rim but spontaneously reducing upon release of pressure. Anterior translation is Grade 1, normal for this patient. O Brien active compression test is positive for deep joint pain when the arm is internally rotated, which is relieved by external rotation, suggesting concomitant superior labral involvement or extension of the posterior tear.
Neurological and Vascular Evaluation
A thorough neurovascular examination reveals symmetric 5 out of 5 strength in the deltoid, biceps, triceps, and intrinsic muscles of the hand. External rotation strength is symmetric, indicating an intact infraspinatus and teres minor. Sensation is intact to light touch in all dermatomal distributions of the upper extremity. Radial and ulnar pulses are 2 plus and symmetric. Capillary refill is brisk.
Imaging and Diagnostics
Accurate diagnosis and surgical templating for posterior instability require a comprehensive imaging protocol to evaluate bone morphology, capsulolabral integrity, and potential neurovascular compromise.
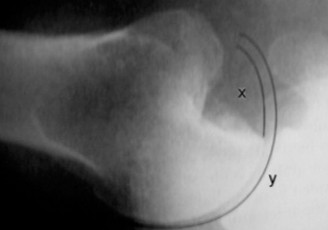
Radiographic Evaluation
Standard radiographic series of the right shoulder, including True Anteroposterior Grashey, Scapular Y, and Axillary lateral views, were obtained. The Grashey view demonstrates a concentric joint space without evidence of degenerative joint disease. The Axillary lateral view is critical and confirms a centered humeral head without static posterior subluxation. There is no evidence of a reverse Hill Sachs lesion on the anterior aspect of the humeral head, and the posterior glenoid rim appears intact without gross osseous deficiency or fragmentation.
Advanced Cross Sectional Imaging
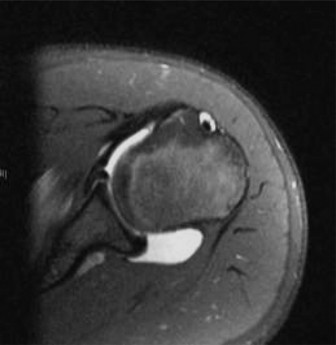
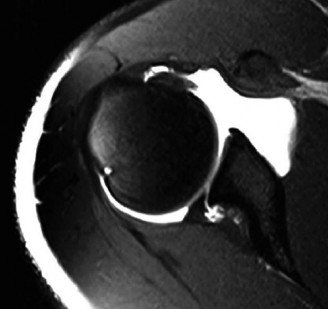
Given the clinical suspicion for a capsulolabral injury, Magnetic Resonance Arthrogram is the gold standard diagnostic modality and was subsequently ordered. The intra articular gadolinium distends the joint capsule, allowing for superior visualization of labral pathology.
The axial T1 fat saturated images demonstrate contrast imbibition between the posterior labrum and the glenoid articular cartilage, extending from the 7 o clock to the 10 o clock position, diagnostic of a posterior labral tear. There is associated stripping of the posterior capsule, consistent with a posterior labrocapsular periosteal sleeve avulsion lesion.
Furthermore, the sagittal oblique and coronal images reveal a patulous posterior capsule, indicative of capsular redundancy secondary to repetitive microtrauma. Evaluation of the spinoglenoid notch shows no evidence of a paralabral cyst, and the muscle bellies of the rotator cuff demonstrate no fatty infiltration or atrophy. The anterior labrum and the long head of the biceps tendon anchor appear intact.

Glenoid Version Templating
Axial Magnetic Resonance imaging cuts were also utilized to calculate glenoid version. The patient demonstrates 8 degrees of retroversion, which falls within the normal physiological range and rules out severe glenoid dysplasia as the primary etiology of his posterior instability.
Differential Diagnosis
The presentation of posterior shoulder pain and mechanical symptoms in a young, overhead, or contact athlete requires a broad differential. The following table outlines the primary differential diagnoses considered during the clinical evaluation.
| Pathology | Mechanism of Injury | Key Clinical Findings | Diagnostic Imaging Hallmarks |
|---|---|---|---|
| Posterior Labrum Tear | Axial load to flexed, adducted, internally rotated arm | Positive Jerk test, Kim test. Pain with cross body adduction. | MRA shows contrast under posterior labrum, capsular stripping, possible paralabral cyst. |
| SLAP Tear | Traction injury, overhead throwing, direct trauma | Positive O Brien test, Crank test, deep vague shoulder pain. | MRA shows superior labral detachment, contrast extending superior to glenoid equator. |
| Suprascapular Neuropathy | Repetitive overhead motion, compression by paralabral cyst | Infraspinatus atrophy, weakness in external rotation, vague posterior pain. | MRI shows spinoglenoid cyst, fatty infiltration of infraspinatus. EMG confirms denervation. |
| Internal Impingement | Extreme external rotation and abduction (late cocking phase) | Posterior joint line pain in abduction/external rotation. Positive impingement signs. | MRI shows articular sided partial rotator cuff tear, posterosuperior labral fraying. |
| Posterior Capsular Contracture | Repetitive microtrauma, altered throwing mechanics | Glenohumeral internal rotation deficit, altered scapular kinematics. | Clinical diagnosis based on ROM deficit. MRI may show thickened posterior capsule. |
Surgical Decision Making and Classification
The management of posterior shoulder instability is dictated by the etiology, chronicity, and specific anatomic lesions present. In this patient, the decision to proceed with operative intervention is based on several critical factors.
Indications for Operative Management
The patient has failed a comprehensive, supervised non operative rehabilitation program lasting longer than three months. Non operative management typically focuses on strengthening the dynamic stabilizers, specifically the posterior deltoid, infraspinatus, teres minor, and periscapular musculature. Despite compliance with this regimen, the patient experiences persistent mechanical symptoms, apprehension, and an inability to return to his previous level of athletic competition. In a young, high demand contact athlete with a confirmed structural lesion, the risk of recurrent instability and progressive chondral damage is high, making surgical stabilization the definitive treatment of choice.
Classification of Posterior Labral Tears
Understanding the specific morphology of the posterior labral tear is essential for surgical planning. Posterior labral tears are frequently classified using the Kim Classification system, which categorizes the pathology based on arthroscopic findings.
Type I lesions represent an incomplete detachment of the labrum without a frank capsular tear. Type II lesions involve a complete detachment of the labrum from the glenoid rim, creating a reverse Bankart lesion. Type III lesions are characterized by a posterior labral tear with associated chondral erosion of the posterior glenoid articular surface. Type IV lesions involve a flap tear of the posterior labrum with a concomitant capsular tear.
Additionally, the lesion must be evaluated for a Posterior Labrocapsular Periosteal Sleeve Avulsion. Unlike a standard reverse Bankart lesion where the periosteum is torn, a POLPSA lesion involves an intact periosteal sleeve that is stripped from the posterior glenoid neck, creating a redundant recess that allows the humeral head to subluxate posteriorly.
Based on the Magnetic Resonance Arthrogram, this patient presents with a Type II complete detachment with POLPSA morphology, necessitating an arthroscopic posterior labral repair with capsular plication to restore anatomic tension.

Surgical Technique and Intervention
Arthroscopic posterior labral repair is a technically demanding procedure that requires meticulous setup, precise portal placement, and a thorough understanding of posterior glenohumeral anatomy.
Patient Positioning and Setup
The procedure is performed under general endotracheal anesthesia supplemented with an interscalene regional nerve block for postoperative analgesia. The patient is positioned in the lateral decubitus position. This position is preferred over the beach chair position for posterior instability cases as it provides superior visualization of the posterior and inferior glenohumeral recesses and facilitates easier capsular shifting.
The operative arm is placed in a balanced suspension system. The arm is positioned in approximately 45 degrees of abduction and 15 degrees of forward flexion. Ten to fifteen pounds of longitudinal traction is applied to distract the joint. Care is taken to ensure all bony prominences, including the common peroneal nerve and the axillary region, are adequately padded.
Portal Placement
Standard diagnostic arthroscopy is initiated via a standard posterior viewing portal, located approximately 2 centimeters inferior and 1 centimeter medial to the posterolateral acromial angle. An anterior mid glenoid portal is established via an outside in technique using a spinal needle through the rotator interval, serving as a working and viewing portal.
For posterior labral repair, an accessory posterolateral portal, also known as the 7 o clock portal, is critical. This portal is established approximately 3 to 4 centimeters inferior and lateral to the standard posterior portal. The trajectory of this portal must be parallel to the posterior glenoid articular surface to allow for proper anchor insertion without skiving or penetrating the articular cartilage.
Diagnostic Arthroscopy and Preparation
The arthroscope is introduced, and a systematic diagnostic tour of the joint is performed. The anterior labrum, superior labrum, and rotator cuff are probed and confirmed to be intact. The arthroscope is then transitioned to the anterior portal to provide an unobstructed, en face view of the posterior labrum.
The posterior labral tear is identified, extending from the 7 o clock to the 10 o clock position. A probe is used to assess the mobility of the labrum and the volume of the posterior capsule. The drive through sign is positive, indicating capsular laxity.
Preparation of the glenoid bed is paramount for biological healing. An arthroscopic elevator and tissue liberator are used to mobilize the labrocapsular complex off the posterior glenoid neck. The mobilization must extend inferiorly to the 6 o clock position to allow for an adequate superior shift of the capsule. A motorized burr is then used to decorticate the posterior glenoid neck down to bleeding subchondral bone, creating an optimal healing environment.
Fixation Construct and Suture Management
The repair is performed using all suture anchors to minimize bone removal and reduce the risk of postoperative hardware complications. The first anchor is placed at the most inferior aspect of the tear, typically at the 7 o clock position. The drill guide is introduced through the accessory posterolateral portal, and the anchor is deployed on the articular margin of the glenoid.
A crescent suture hook loaded with a shuttle relay is introduced through the standard posterior portal. The hook is passed through the posterior band of the inferior glenohumeral ligament and the posterior labrum, taking a substantial bite of capsular tissue inferior to the anchor to effect a superior and medial capsular plication. The suture is shuttled, and a sliding locking knot, backed up by alternating half hitches, is tied using a knot pusher.
This process is repeated sequentially, moving superiorly along the glenoid rim. Anchors are placed at the 8 o clock and 9 o clock positions. Care is taken to balance the capsular tension, ensuring that the posterior capsule is adequately plicated without over constraining the joint.
Final Assessment
Once all anchors are placed and knots are tied, the joint is dynamically assessed. The arthroscope is used to visualize the repair, confirming that the labrum is anatomically reduced to the glenoid rim and the posterior capsular volume is appropriately reduced. The humeral head is noted to be well centered on the glenoid. The portals are closed with non absorbable sutures, and the arm is placed in a specialized abduction sling with a neutral rotation wedge.
Post Operative Protocol and Rehabilitation
The success of an arthroscopic posterior labral repair is heavily dependent on strict adherence to a phased postoperative rehabilitation protocol. The primary goal is to protect the healing labrocapsular complex while gradually restoring range of motion, strength, and neuromuscular control.
Phase One Immediate Post Operative Period
This phase encompasses weeks zero through four. The patient is strictly immobilized in a sling with a small abduction pillow, maintaining the arm in neutral to slight external rotation. Internal rotation, forward flexion, and cross body adduction are strictly contraindicated, as these motions place direct stress on the posterior repair.
Therapeutic interventions during this phase are limited to active range of motion of the cervical spine, elbow, wrist, and hand. Submaximal, pain free isometric exercises for the deltoid and periscapular musculature are initiated. Cryotherapy is utilized extensively for pain and edema control.
Phase Two Intermediate Range of Motion
Spanning weeks four through eight, the sling is gradually discontinued. Passive range of motion is initiated, progressing to active assisted range of motion. Forward elevation is permitted in the scapular plane, progressing to 90 degrees by week six and full elevation by week eight. External rotation is progressed as tolerated.
Internal rotation is introduced cautiously. The patient is allowed to perform internal rotation stretching in the scapular plane, but combined positions of forward flexion, internal rotation, and horizontal adduction are avoided until week eight. Scapular stabilization exercises, including rows and prone extensions, are incorporated.
Phase Three Strengthening and Neuromuscular Control
From weeks eight through twelve, the focus shifts to restoring muscular strength and endurance. Isotonic strengthening exercises for the rotator cuff and periscapular musculature are advanced. Proprioceptive training, including closed kinetic chain exercises such as wall push ups and rhythmic stabilization drills, is emphasized to restore dynamic joint stability.
Phase Four Return to Sport
Beginning at three to four months postoperatively, the patient transitions to sport specific training. For an offensive lineman, this includes progressive resistance training, plyometrics, and blocking drills. Return to unrestricted contact sports is typically permitted between five and six months, contingent upon the patient demonstrating symmetric range of motion, normal scapulothoracic kinematics, and isokinetic strength testing revealing at least 90 percent strength compared to the contralateral extremity.
Clinical Pearls and Pitfalls
Mastering the diagnosis and surgical management of posterior labral tears requires an appreciation of several nuanced pearls and avoidance of common pitfalls.
Diagnostic Pearls
A high index of suspicion must be maintained for posterior labral pathology in contact athletes presenting with vague posterior shoulder pain, even in the absence of a frank dislocation. The Kim test and Jerk test are highly specific when performed correctly. Always evaluate for concomitant pathology, such as anterior labral tears or SLAP lesions, as multidirectional instability or pan labral tears require a modified surgical approach.
Surgical Pearls
Visualization is the key to a successful repair. Utilizing the anterior mid glenoid portal for viewing provides a panoramic perspective of the posterior labrum that cannot be achieved from the standard posterior portal.
Adequate tissue mobilization is critical. The posterior capsule and labrum must be completely freed from the glenoid neck down to the 6 o clock position. Failure to achieve this will result in a repair under excessive tension and a high risk of failure.
The use of the accessory posterolateral portal is non negotiable. Attempting to place anchors at the 7 o clock position from the standard posterior portal will result in a severe angle of approach, leading to anchor skiving, articular cartilage damage, or inadequate fixation.
Potential Pitfalls
A major pitfall is failing to recognize and treat a paralabral cyst. If a cyst is identified on preoperative Magnetic Resonance Imaging, it must be decompressed intraoperatively to relieve pressure on the suprascapular nerve. This is typically achieved by finding the capsular defect feeding the cyst and utilizing a motorized shaver to evacuate the mucinous contents.
Over tightening the posterior capsule is another significant pitfall. While capsular plication is necessary to eliminate redundancy, excessive plication will result in a severe glenohumeral internal rotation deficit. This loss of motion can alter throwing mechanics or blocking techniques, leading to secondary shoulder pathology or subacromial impingement.
Finally, poor anchor trajectory can lead to disastrous complications. Anchors placed too medially will not adequately restore the labral bumper, while anchors placed too laterally will violate the articular cartilage, leading to rapid onset glenohumeral osteoarthritis. Strict adherence to proper portal placement and the use of drill guides parallel to the articular surface will mitigate this risk.
You Might Also Like