Chronic Anterior Glenohumeral Dislocation: A Case Study on Diagnosis & Imaging Challenges
Key Takeaway
Chronic anterior glenohumeral dislocation diagnosis involves a thorough clinical exam revealing deformity and restricted ROM. Advanced imaging, including CT with 3D reconstruction and MRI, is crucial to assess glenoid bone loss (e.g., bony Bankart) and humeral head defects (e.g., Hill-Sachs lesion), often missed in initial radiographs, guiding appropriate surgical planning.
Patient Presentation and History
Mechanism of Injury and Chronology
A 68-year-old male, right-hand dominant, presented to the Orthopedic Trauma Clinic complaining of persistent right shoulder pain and significant functional limitation for the past four months. He reported a fall directly onto his outstretched right arm while descending stairs approximately four months prior. The biomechanics of this injury typically involve a combination of abduction, extension, and external rotation forces applied to the glenohumeral joint, leveraging the humeral head out of the glenoid fossa anteriorly. Immediately following the injury, he experienced severe pain and an absolute inability to move his shoulder.
He initially sought care at a local urgent care facility. At that time, initial anteroposterior radiographs were reportedly interpreted as normal, and he was advised to rest, utilize a sling for comfort, and manage the pain with over-the-counter analgesics. Despite strict adherence to this conservative protocol, his pain persisted at a high baseline. He noted a constant, deep-seated mechanical sensation of the joint being incongruent, coupled with progressive, debilitating stiffness. Over the ensuing four months, he developed an inability to perform basic activities of daily living, particularly overhead reaching, personal hygiene tasks, and sleeping on the affected right side.
Demographics and Comorbidities
His medical history is significant for well-controlled essential hypertension and Type 2 Diabetes Mellitus (HbA1c 6.8%). He also reported a remote history of right shoulder impingement syndrome managed non-operatively with physical therapy and a single subacromial corticosteroid injection five years prior. He is a retired accountant, living independently, with a high baseline functional demand for his age. There is no history of prior shoulder dislocations, generalized ligamentous laxity, or seizure disorders.
He denied any acute neurological deficits or vascular compromise in the affected limb since the initial injury. The substantial delay in definitive diagnosis and presentation to a specialized orthopedic trauma service highlights the insidious nature of chronic dislocations. These injuries are frequently missed during initial assessments in emergency or urgent care settings, particularly in the elderly population where osteopenia can obscure subtle radiographic signs, or in patients presenting with atypical, less dramatic clinical deformities due to significant soft tissue envelopes or concomitant proximal humerus fractures.
Clinical Examination Findings
Inspection and Palpation
Upon rigorous inspection of the right shoulder girdle, a clear and classic deformity was evident, albeit partially masked by the chronicity of the condition. The normal rounded contour of the deltoid muscle was flattened anteriorly, and there was a palpable, prominent step-off at the lateral edge of the acromion. The humeral head was noted to be displaced anteriorly and inferiorly, creating a distinct, firm bulge in the subcoracoid region. There was no significant skin discoloration, ecchymosis, open wounds, or signs of acute inflammation, consistent with the four-month timeline. Profound muscle atrophy was notable across the entire shoulder girdle, particularly involving the deltoid, supraspinatus, and infraspinatus fossae. This global atrophy is a direct consequence of prolonged disuse and altered joint kinematics secondary to the chronic dislocation.
Palpation revealed deep, localized tenderness over the anterior aspect of the glenohumeral joint and the subcoracoid area, directly corresponding to the displaced, impacted humeral head. The posterior aspect of the glenohumeral joint felt entirely empty, with the posterior glenoid rim easily palpable beneath the atrophic posterior deltoid and infraspinatus. No gross crepitus was elicited on gentle manipulation, likely due to the rigid fibrotic fixation of the humeral head in its dislocated position.
Range of Motion Kinematics
Range of Motion (ROM) assessment demonstrated severe restriction and significant pain at the extremes of his limited arc. Active and passive ROM measurements were virtually identical, indicating a mechanical block rather than solely a pain-limited or paralytic etiology:
* Flexion: 45 degrees (normal 180 degrees)
* Abduction: 30 degrees (normal 180 degrees)
* External Rotation (at 0 degrees abduction): 0 degrees (normal 60-70 degrees)
* Internal Rotation (at 0 degrees abduction): 20 degrees (normal 70-80 degrees)
All glenohumeral movements were highly guarded, presenting with a firm, painful end-feel. The absolute lack of external rotation is a hallmark clinical sign of a chronic anterior dislocation with a significant engaging Hill-Sachs lesion impaled on the anterior glenoid rim. Apprehension testing was overwhelmingly positive on any minimal attempts at external rotation and abduction, though true apprehension was difficult to separate from the mechanical pain of the impaction.
Neurological and Vascular Assessment
A meticulous neurological assessment is paramount in chronic dislocations due to the sustained traction on the brachial plexus. The axillary nerve was evaluated clinically and found to be intact, demonstrating good deltoid and teres minor contraction against resistance (graded 4/5, limited by pain and disuse atrophy rather than denervation) and normal, symmetric light touch sensation over the lateral deltoid regimental badge area. Suprascapular, musculocutaneous, radial, ulnar, and median nerve functions were also systematically tested and found to be grossly intact.
Distal vascular status was confirmed with strong, symmetric palpable radial and ulnar pulses, normal capillary refill (under 2 seconds), and warm extremities. Assessment of the cervical spine, including Spurling's maneuver and cervical range of motion, was entirely unremarkable, effectively ruling out a concomitant cervical radiculopathy contributing to the shoulder pain or profound dysfunction.
Imaging and Diagnostics
Initial Radiographic Evaluation
The initial radiographs from the outside facility, when acquired and reviewed, were indeed subtle but retrospectively demonstrated a clear anterior glenohumeral dislocation that had been unfortunately missed. The primary error in the initial evaluation was the reliance on a single, non-orthogonal anteroposterior view without a dedicated axillary or lateral scapular projection. On the current presentation, a complete trauma series of the shoulder was obtained, consisting of a true AP glenoid (Grashey) view, an axillary lateral view, and a scapular Y-view.
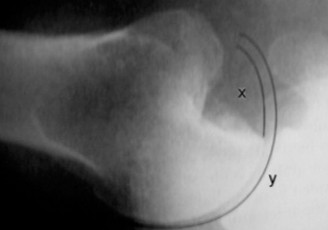
The AP Glenoid View showed the humeral head displaced anteriorly and medially relative to the glenoid fossa, lying inferior to the coracoid process. Crucially, the normal elliptical overlap of the humeral head and the glenoid (the "half-moon" sign) was absent. Instead, the humeral head was completely medial to the anterior glenoid rim.

The Axillary View is the absolute gold standard and most crucial radiograph for confirming the direction of any glenohumeral dislocation. In this case, it unequivocally depicted the humeral head resting completely anterior to the glenoid vault. Furthermore, this view allowed for a preliminary assessment of significant anterior glenoid bone loss and a massive, deep Hill-Sachs defect on the posterolateral humeral head, which was actively engaging the anterior glenoid rim.
The Scapular Y-View provided additional confirmation, demonstrating the humeral head lying anterior to the intersection of the coracoid, acromion, and scapular body (the center of the "Y"), further corroborating the subcoracoid position of the dislocation.
Advanced Cross Sectional Imaging
Given the chronicity of the dislocation (four months) and the radiographic evidence of significant bony defects, advanced cross-sectional imaging was mandated for preoperative planning and precise quantification of bone loss. A non-contrast Computed Tomography (CT) scan of the right shoulder with 3D reconstructions was ordered.

The CT scan is the definitive modality for evaluating the osseous anatomy in chronic instability. The axial and sagittal reformats, along with the 3D surface-rendered images with digital subtraction of the humeral head, revealed a catastrophic pathoanatomy.
1. Glenoid Bone Loss: There was severe attritional bone loss of the anterior glenoid rim, estimated at approximately 35% of the anterior-posterior width of the inferior glenoid circle. The anterior rim was blunted and sclerotic, indicating chronic mechanical wear.
2. Hill-Sachs Defect: A massive, deep, and wide Hill-Sachs lesion was identified on the posterolateral aspect of the humeral head. Measuring the volume and orientation of this defect confirmed it was an "engaging" lesion.
3. Glenoid Track Paradigm: Applying the glenoid track concept, the massive Hill-Sachs lesion was entirely "off-track." The width of the Hill-Sachs defect far exceeded the remaining intact anterior glenoid articular surface, explaining the absolute mechanical block to external rotation and the impossibility of maintaining a stable closed reduction.
Magnetic Resonance Imaging (MRI) was considered but ultimately deemed secondary to CT in this specific scenario. While MRI is excellent for evaluating the rotator cuff and capsulolabral structures, the primary surgical driver in a 4-month chronic dislocation with massive bone loss in a 68-year-old is the osseous deficiency and joint arthrosis. The CT scan provided sufficient data to confirm that joint preservation would be highly likely to fail, making the status of the labrum irrelevant. However, the CT did show significant fatty infiltration and atrophy of the subscapularis and infraspinatus muscles (Goutallier stage 3), which heavily influenced the final surgical decision-making process.
Differential Diagnosis
When evaluating a patient with chronic shoulder pain, profound stiffness, and functional loss following a traumatic event several months prior, the differential diagnosis must encompass missed mechanical derangements, massive soft tissue failures, and secondary fibrotic conditions. The table below outlines the primary differential diagnoses considered during the evaluation of this patient.
| Differential Diagnosis | Clinical Presentation Nuances | Radiographic Hallmarks | Distinguishing Features from Current Case |
|---|---|---|---|
| Chronic Anterior Glenohumeral Dislocation | Severe limitation in all planes, absolute block to external rotation, palpable anterior fullness, flattened lateral deltoid. | AP: Loss of half-moon sign. Axillary: Humeral head anterior to glenoid. CT: Anterior glenoid wear, posterolateral Hill-Sachs. | This is the definitive diagnosis. Matches the subcoracoid fullness, specific ROM blocks, and exact radiographic findings. |
| Chronic Posterior Glenohumeral Dislocation | Arm locked in internal rotation, severe limitation of external rotation and elevation. Prominent coracoid anteriorly, fullness posteriorly. | AP: "Lightbulb" sign (internal rotation of humerus), empty glenoid sign. Axillary: Humeral head posterior to glenoid. | The patient had an anterior, not posterior, bulge. Radiographs definitively showed anterior, not posterior, displacement. |
| Massive Rotator Cuff Tear (Pseudoparalysis) | Active elevation typically less than 90 degrees, but passive ROM is often relatively preserved or full. Weakness is the primary driver, not a mechanical block. | Radiographs may show superior migration of the humeral head (decreased acromiohumeral interval). MRI confirms massive tendinous retraction. | This patient had a rigid, firm mechanical block to both active and passive ROM, ruling out a simple soft-tissue pseudoparalysis. |
| Adhesive Capsulitis (Frozen Shoulder) | Insidious onset of global stiffness (capsular pattern: ER > Abduction > IR). Pain at end-range. Often idiopathic or linked to diabetes. | Radiographs are typically entirely normal. MRI may show thickening of the coracohumeral ligament and joint capsule. | While the patient is diabetic and stiff, the clear history of trauma, the visible deformity, and the grossly abnormal radiographs rule out simple adhesive capsulitis. |
Surgical Decision Making and Classification
Rationale for Operative Intervention
The management of chronic anterior glenohumeral dislocations is complex and dictated by the duration of the dislocation, the age and functional demand of the patient, the extent of osseous defects, and the condition of the rotator cuff and articular cartilage. Non-operative management is universally poorly tolerated, leaving the patient with a permanently painful, mechanically useless extremity, and progressive neurovascular risk due to chronic traction. Therefore, operative intervention is strictly indicated for this patient.
The chronicity of the dislocation (four months) represents a critical threshold. Dislocations neglected for longer than 3-4 weeks undergo profound pathoanatomical changes. The joint capsule becomes severely contracted and fibrotic. The displaced humeral head becomes firmly adherent to the anterior scapular neck and coracoid process through dense scar tissue. Attempting a closed reduction in a dislocation older than 4 weeks is strictly contraindicated due to the unacceptably high risk of iatrogenic proximal humerus fractures, catastrophic brachial plexus traction injuries, and axillary artery intimal tears or ruptures.
Treatment Algorithm and Classification Assessment
The surgical decision-making process requires a careful evaluation of joint preservation versus joint replacement.
1. Open Reduction and Internal Fixation / Soft Tissue Stabilization: In a young patient (under 40) with a chronic dislocation of a few weeks, open reduction via a deltopectoral approach, extensive soft tissue release, and concurrent stabilization (e.g., Latarjet procedure for anterior bone loss, Remplissage for the Hill-Sachs) might be considered.
2. Arthroplasty: In older patients, or those with prolonged chronicity (months to years), joint preservation is generally doomed to failure. The articular cartilage of the humeral head undergoes rapid degeneration (chondrolysis) due to lack of synovial fluid nutrition and continuous mechanical impaction against the glenoid rim. Furthermore, the massive osseous defects (35% anterior glenoid loss, massive off-track Hill-Sachs) make achieving stability with native bone nearly impossible.
In this 68-year-old patient, several factors mandated a reconstructive arthroplasty approach rather than joint preservation:
* Age and Chronicity: 68 years old with a 4-month neglected dislocation implies irreversible cartilage damage and severe soft tissue contracture.
* Bone Loss: Severe anterior glenoid deficiency and a massive engaging Hill-Sachs lesion.
* Rotator Cuff Status: CT evidence of Goutallier stage 3 fatty infiltration of the subscapularis and infraspinatus indicates that the rotator cuff is functionally compromised and unlikely to provide dynamic stability or adequate function post-operatively.
Selection of Arthroplasty Construct
Given the decision to proceed with arthroplasty, the choice between Anatomic Total Shoulder Arthroplasty (aTSA) and Reverse Total Shoulder Arthroplasty (RTSA) must be made. An aTSA relies on an intact and functioning rotator cuff to maintain the humeral head centered on the glenoid. Given the severe subscapularis insufficiency (stretched over the dislocated head for months, fatty infiltrated) and the massive anterior glenoid bone loss (which would make seating an anatomic glenoid component highly prone to anterior eccentric wear and early loosening), an anatomic replacement is contraindicated.
Therefore, Reverse Total Shoulder Arthroplasty (RTSA) is the definitive procedure of choice. RTSA biomechanically bypasses the need for a functioning rotator cuff by medializing the center of rotation and distalizing the humerus, thereby recruiting the deltoid to act as the primary elevator and stabilizer. Furthermore, the baseplate of the RTSA can be securely fixed to the remaining native glenoid vault, and the semi-constrained nature of the reverse articulation provides inherent stability against anterior translation, effectively neutralizing the massive bone loss and soft tissue incompetence.
Surgical Technique and Intervention
Patient Positioning and Anesthesia
The patient was brought to the operating room and placed in the beach chair position after the administration of general endotracheal anesthesia. A preoperative interscalene regional nerve block was performed by the anesthesia team to ensure optimal perioperative pain control. The right upper extremity was prepped and draped in standard sterile orthopedic fashion, allowing for full, unencumbered mobility of the arm. A mechanical arm positioner was utilized to assist with precise intraoperative positioning.
Surgical Approach and Extensive Soft Tissue Releases
A standard extended deltopectoral approach was utilized. The skin incision followed the coracoid process distally toward the deltoid tuberosity. The cephalic vein was identified and retracted laterally with the deltoid to protect its delicate venous drainage.
Upon entering the deltopectoral interval, the profound distortion of the normal anatomy was immediately apparent. The humeral head was firmly encased in a dense, fibrotic pseudocapsule anterior to the glenoid and directly inferior to the coracoid process. The conjoint tendon was identified and gently retracted medially. The axillary nerve was meticulously palpated and protected at the inferior border of the subscapularis; its course was significantly distorted due to the anteroinferior displacement of the proximal humerus.
The most critical and technically demanding phase of chronic dislocation surgery is the soft tissue release. The subscapularis tendon was found to be severely attenuated, stretched, and scarred. A tenotomy of the subscapularis was performed approximately 1 cm medial to its insertion on the lesser tuberosity. The underlying anterior capsule, which was heavily thickened, was excised.
To mobilize the rigidly fixed humeral head, a circumferential capsular release was mandatory. This included a complete release of the coracohumeral ligament, release of the superior capsule, and a careful inferior capsular release, staying strictly on the humeral side to avoid iatrogenic injury to the axillary nerve. Despite these releases, the humeral head remained impacted on the anterior glenoid rim.
Humeral Head Resection and Glenoid Preparation
To facilitate exposure of the glenoid and safely disimpact the joint without causing a humeral shaft fracture, an in situ humeral head resection was performed. The anatomic neck was identified, and a reciprocating saw was used to perform the humeral osteotomy while the head remained dislocated. Once the osteotomy was complete, the resected humeral head—which exhibited severe full-thickness cartilage loss and the massive posterolateral Hill-Sachs defect—was extracted from the joint space.
Removal of the humeral head finally provided excellent visualization of the glenoid face. The glenoid exhibited the anticipated severe anterior attritional bone loss. The labrum was completely absent anteriorly, replaced by dense scar tissue. The glenoid vault was meticulously cleared of all remaining capsular tissue and labral remnants.
Component Implantation
Glenoid Reconstruction: The center point for the baseplate was identified. Due to the anterior bone loss, the starting point was shifted slightly posterior and inferior to maximize bone purchase in the native vault. The glenoid was reamed to correct the version and create a concentric surface. Care was taken to avoid over-reaming, which would deplete the already compromised subchondral bone stock. A standard RTSA baseplate with a central compressive screw was impacted into place. Peripheral locking screws were then placed—superiorly into the base of the coracoid and inferiorly down the scapular pillar—achieving excellent rigid, bi-cortical fixation. A standard 38mm glenosphere was then impacted and secured via a Morse taper mechanism.
Humeral Reconstruction: The proximal humerus was prepared using sequential broaches to accommodate the humeral stem. Given the patient's age and bone quality, a cemented humeral stem was selected to ensure immediate rigid fixation and prevent subsidence. A trial reduction was performed using a standard polyethylene insert.
Reduction and Stability Assessment
The joint was reduced, and a rigorous assessment of stability and soft tissue tension was conducted. The construct demonstrated excellent stability in all planes. There was no impingement of the humeral component on the scapular neck during adduction, and the conjoint tendon tension was appropriate, indicating adequate distalization and medialization of the joint center of rotation.
The final cemented humeral stem was implanted, and the definitive polyethylene articular insert was impacted into place. The joint was definitively reduced. Given the severe attenuation and fatty infiltration of the subscapularis, a formal repair of the subscapularis tendon was deemed impossible and unnecessary, as the RTSA construct relies on the deltoid for stability and function. A standard layered closure was performed over a closed suction drain.

Post-operative radiographs confirmed excellent positioning of the Reverse Total Shoulder Arthroplasty components. The baseplate was flush with the prepared glenoid, the screws were appropriately sized and positioned, and the humeral stem was centrally aligned within the medullary canal with adequate distalization.
Post Operative Protocol and Rehabilitation
The post-operative rehabilitation protocol following a Reverse Total Shoulder Arthroplasty for a chronic dislocation requires a delicate balance between protecting the implant fixation and restoring functional mobility in a shoulder that has been rigidly immobilized for months.
Phase I: Immediate Post-Operative Protection (Weeks 0-4)
The patient was placed in a standard shoulder immobilizer sling immediately post-operatively. The primary goal during this phase is to allow for soft tissue healing, particularly the deltopectoral interval, and to manage pain and swelling.
* Immobilization: The sling is worn continuously, removed only for hygiene and specific directed exercises.
* Precautions: Strict avoidance of combined shoulder extension, adduction, and internal rotation (the position of dislocation for an RTSA).
* Exercises: Immediate initiation of active range of motion for the elbow, wrist, and hand to prevent distal stiffness. Passive Range of Motion (PROM) of the shoulder is initiated under the strict guidance of a physical therapist. Forward elevation is limited to 90 degrees, and external rotation is limited to 20 degrees to protect the anterior soft tissue envelope.
Phase II: Active-Assisted Range of Motion (Weeks 4-8)
As soft tissue healing progresses, the focus shifts to restoring the arc of motion safely.
* Sling Discontinuation: The sling is gradually weaned for activities of daily living in safe environments.
* Exercises: Transition from passive to Active-Assisted Range of Motion (AAROM). Pulleys, wand exercises, and wall walks are introduced. The limits on forward elevation and external rotation are gradually advanced based on patient tolerance and the absence of pain. Deltoid isometric activation exercises are initiated.
Phase III: Active Range of Motion and Early Strengthening (Weeks 8-12)
- Exercises: Progression to full Active Range of Motion (AROM) in all planes. The patient is encouraged to use the arm for light, functional activities below shoulder level.
- Strengthening: Introduction of light, progressive resistive exercises focusing on the deltoid and the remaining intact periscapular musculature (trapezius, serratus anterior, rhomboids). TheraBand exercises and light dumbbells (1-2 lbs) are utilized.
Phase IV: Advanced Strengthening and Functional Return (Months 3-6+)
- Exercises: Continued progression of deltoid and periscapular strengthening. Focus on proprioception and neuromuscular control.
- Functional Return: Gradual return to heavier activities of daily living and recreational pursuits. Patients are generally advised to avoid repetitive heavy lifting (greater than 15-20 lbs) or high-impact activities permanently to maximize the longevity of the arthroplasty components.
Clinical Pearls and Pitfalls
Clinical Pearls
- The Mandatory Axillary View: The most critical pearl in the evaluation of any shoulder trauma is the absolute necessity of obtaining an orthogonal axillary lateral radiograph. A standard AP view alone is insufficient and is the primary reason anterior and posterior dislocations are missed in the acute setting.
- High Index of Suspicion in the Elderly: Chronic dislocations present insidiously in older patients. They may not exhibit the classic severe, acute pain of a young athlete. Any elderly patient presenting with persistent shoulder pain, profound stiffness, and a history of a fall must be evaluated for a missed dislocation.
- In Situ Resection for Chronic Cases: When performing an arthroplasty for a chronically dislocated shoulder, attempting to lever the humeral head back into the glenoid prior to resection carries a massive risk of iatrogenic spiral fractures of the humerus. Performing an in situ osteotomy of the humeral neck allows for safe extraction of the head and significantly reduces fracture risk.
- RTSA as the Ultimate Salvage: Reverse Total Shoulder Arthroplasty is the workhorse procedure for chronic dislocations in older patients. It simultaneously addresses the massive glenoid bone loss, the engaging Hill-Sachs defect, the compromised rotator cuff, and the severe articular cartilage degeneration.
Clinical Pitfalls
- Attempting Closed Reduction: Attempting a closed reduction in the emergency department or under sedation for a dislocation that has been present for longer than 3-4 weeks is a dangerous pitfall. The fibrotic adhesions and bone loss make successful closed reduction impossible and highly likely to result in neurovascular injury or iatrogenic fracture.
- Underestimating Bone Loss: Relying solely on plain radiographs to assess glenoid bone loss in chronic instability is inadequate. A 3D CT scan is mandatory for accurate preoperative templating. Failure to recognize severe anterior wear can lead to improper baseplate positioning, early loosening, and catastrophic implant failure.
- Neglecting the Axillary Nerve: The axillary nerve is highly vulnerable in chronic anterior dislocations due to chronic traction and anatomic distortion by the displaced humeral head. Failure to carefully identify, mobilize, and protect the nerve during the inferior capsular release can result in permanent deltoid paralysis, which is devastating for the function of a Reverse Total Shoulder Arthroplasty.
You Might Also Like