Open Reduction of Anterior Shoulder Dislocations: Surgical Techniques and Protocols
Key Takeaway
Open reduction of an anterior shoulder dislocation is indicated for chronic, irreducible, or complex fracture-dislocations. Utilizing the Rowe and Zarins technique via a deltopectoral approach allows for direct visualization, subscapularis release, and capsular mobilization. Meticulous surgical technique is paramount to safely clear the fibrotic glenoid fossa, achieve concentric reduction without iatrogenic fracture, and protect the axillary nerve during subscapularis repair.
OPEN REDUCTION OF ANTERIOR SHOULDER DISLOCATIONS
While the vast majority of acute anterior shoulder dislocations can be successfully managed with closed reduction techniques in the emergency department, a distinct subset of patients requires surgical intervention. Open reduction of an anterior shoulder dislocation is a formidable orthopedic challenge, typically reserved for chronic (unreduced) dislocations, irreducible acute dislocations secondary to soft tissue interposition (e.g., the long head of the biceps tendon, capsule, or subscapularis), or complex fracture-dislocations where closed manipulation poses an unacceptable risk of iatrogenic neurovascular or osseous injury.
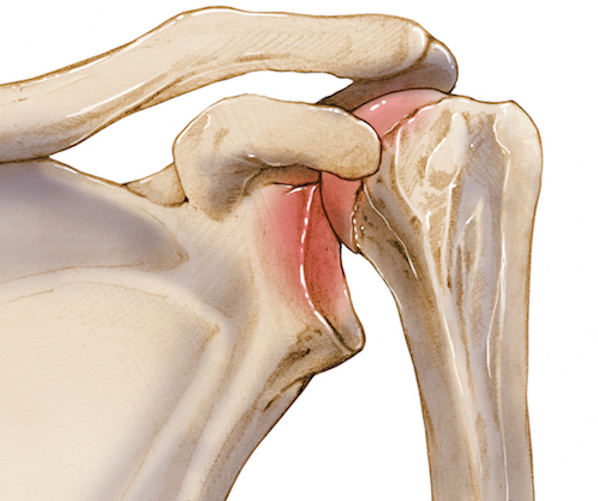
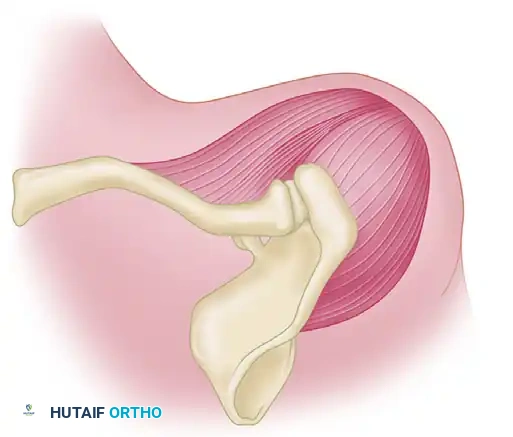
The pathoanatomy of a chronic anterior dislocation is characterized by severe soft tissue contracture and osseous remodeling. The anterior capsule and the coracohumeral ligament become profoundly contracted, tethering the humeral head in its dislocated, anteroinferior position. Concurrently, the empty glenoid fossa rapidly fills with dense, tenacious fibrous tissue, obliterating the articular concavity. Furthermore, the dislocated humeral head undergoes rapid disuse osteopenia, rendering it highly susceptible to iatrogenic crush fractures or shear injuries during forceful reduction attempts.
Preoperative Planning and Biomechanical Considerations
Thorough preoperative planning is mandatory. Standard trauma series radiographs (true anteroposterior, scapular Y, and axillary lateral views) are essential to confirm the direction of the dislocation and identify associated osseous lesions, such as a Hill-Sachs defect or an anterior glenoid rim fracture (bony Bankart lesion).
Advanced imaging, particularly Computed Tomography (CT) with 3D reconstruction, is highly recommended for chronic dislocations to quantify glenoid bone loss and assess the structural integrity of the humeral head. Magnetic Resonance Imaging (MRI) may be utilized to evaluate the status of the rotator cuff, which is frequently torn in older patients sustaining anterior dislocations.
Surgical Warning: The axillary nerve and the musculocutaneous nerve are at significant risk in chronic anterior dislocations. The humeral head often rests directly against the brachial plexus cords. Preoperative electromyography (EMG) or a meticulous clinical neurologic examination must be documented to establish a baseline before surgical intervention.
SURGICAL TECHNIQUE: THE ROWE AND ZARINS APPROACH
The technique described by Rowe and Zarins remains a foundational procedure for the open reduction of complex or chronic anterior shoulder dislocations. It utilizes a standard anterior deltopectoral approach, providing extensile access to the anterior glenohumeral joint while preserving the deltoid origin.
Patient Positioning and Anesthesia
- Anesthesia: General endotracheal anesthesia is preferred, often supplemented with an interscalene regional nerve block for optimal postoperative pain control and intraoperative muscle relaxation.
- Positioning: The patient is placed in the beach-chair (modified Fowler) position, with the head and neck secured in a neutral posture.
- Draping: The affected upper extremity is prepped and draped free to allow for unrestricted manipulation of the arm during the reduction maneuver. A sterile Mayo stand or arm board can be used to support the limb.
The Deltopectoral Approach
- Incision: Make a longitudinal incision extending from the lateral third of the clavicle, coursing inferiorly and slightly laterally along the deltopectoral groove for approximately 10 to 12.5 cm.
- Superficial Dissection: Identify the deltopectoral interval by locating the cephalic vein. The vein is typically retracted laterally with the deltoid muscle to preserve its primary venous tributaries, although medial retraction with the pectoralis major is an acceptable alternative depending on the specific venous anatomy encountered.
- Deep Dissection: Separate the deltoid and pectoralis major muscles to expose the clavipectoral fascia. Incise the fascia lateral to the conjoined tendon (comprising the short head of the biceps brachii and the coracobrachialis).
- Retraction: Retract the conjoined tendon medially. At this stage, the dislocated humeral head may be directly visualized or palpated with a blunt instrument resting in an abnormal position inferior to the coracoid process.
Capsular Mobilization and Joint Preparation
The critical barrier to reduction in a chronic setting is the contracted soft tissue envelope and the fibrotic obliteration of the glenoid.
- Subscapularis Management: The subscapularis muscle is often stretched tightly over the dislocated humeral head. Release of the subscapularis is necessary to access the joint. This can be performed via a vertical tenotomy approximately 1 cm medial to its insertion on the lesser tuberosity, or via a lesser tuberosity osteotomy, depending on surgeon preference and tissue quality.
- Capsulotomy: Open the anterior joint capsule. It is imperative to completely divide the contracted coracohumeral ligament, which acts as a primary tether preventing the humeral head from translating posteriorly and inferiorly back into the glenoid.
- Glenoid Clearance: Inspect the glenoid cavity. In chronic cases, it will be filled with dense, organized fibrous tissue. Use a combination of curettes, rongeurs, and periosteal elevators to meticulously free the glenoid cavity of this fibrotic material. Failure to completely clear the glenoid fossa will result in an eccentric reduction and immediate postoperative instability.
The Reduction Maneuver
Clinical Pearl: Avoid using excessive mechanical force or heavy metallic levers (e.g., bone skids or Cobb elevators) against the articular surface. The osteoporotic bone of the chronically dislocated humeral head or the glenoid rim is exceptionally fragile and will fracture under focal pressure.
- Gentle Manipulation: Apply gentle, sustained longitudinal traction to the arm while simultaneously translating the humeral head laterally and posteriorly.
- Soft Tissue Stretching: Slowly stretch the contracted soft tissues. Manipulate the shoulder through a gradual range of motion until the joint kinematics feel almost normal.
- Concentric Reduction: Gently guide the humeral head back into the prepared glenoid cavity. Confirm concentric reduction visually and via fluoroscopy if necessary.
Closure and Axillary Nerve Protection
- Capsular Management: Due to severe chronic contracture, the anterior capsule will often be too tight to close primarily once the humeral head is reduced. Do not force capsular closure, as this will severely restrict external rotation and obligate posterior subluxation of the humeral head.
- Subscapularis Repair: Carefully repair the subscapularis tendon using heavy non-absorbable sutures. If a lesser tuberosity osteotomy was performed, repair it with heavy transosseous sutures or suture anchors.
Surgical Warning: Remember that the axillary nerve lies just inferior to the muscular border of the subscapularis as it passes from anterior to posterior through the quadrangular space. Meticulous suture placement is required during the inferior aspect of the subscapularis repair to avoid iatrogenic entrapment or ligation of the axillary nerve.
EXTENSILE EXPOSURES: THE DELTOID TURN-DOWN APPROACH
In cases of severe chronic unreduced dislocations where the standard deltopectoral approach provides insufficient access to the posterior and superior aspects of the shoulder capsule, a combined or extensile approach may be indicated.
As described by Rowe and Zarins for highly complex reconstructions, a deltoid turn-down approach can be utilized to expose both the anterior and posterior aspects of the shoulder joint simultaneously.
Technique for Deltoid Turn-Down
- Skin Incision: A broader, superiorly based skin incision is utilized (indicated by the heavy dotted line in preoperative planning). This allows for a massive skin flap to be elevated, exposing the entire acromion and the origin of the deltoid.
- Acromial Osteotomy: Rather than detaching the deltoid directly from the bone—which carries a high risk of postoperative deltoid dehiscence and catastrophic functional loss—a precise osteotomy of the acromion is performed.
- Bone Sleeve: As illustrated (light dotted line), the osteotomy is made to leave approximately 5 mm of acromial bone attached to the proximal origin of the deltoid muscle.
- Reflection: The deltoid muscle, along with its attached bony sleeve, is then turned down (reflected distally). This provides unparalleled, 270-degree visualization of the glenohumeral joint, allowing for extensive capsular releases, management of severe osseous defects, and safe mobilization of the chronically displaced humeral head.
- Repair: During closure, the bony sleeve is rigidly repaired back to the native acromion using heavy transosseous sutures or tension band wiring, ensuring a robust bone-to-bone healing environment for the deltoid origin.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative care following an open reduction of an anterior shoulder dislocation must be carefully tailored to balance the need for joint stability with the prevention of debilitating postoperative stiffness. The protocol varies depending on whether adjunctive internal fixation was required (e.g., for associated fractures or severe instability).
Phase I: Immobilization and Early Protection (Weeks 0 to 3)
- Standard Rowe and Zarins Protocol: If the standard soft-tissue open reduction technique is used without internal osseous fixation, the arm is supported in a sling or shoulder immobilizer.
- Internal Fixation Protocol: If internal fixation is utilized (e.g., screw fixation of a large glenoid rim fracture or tuberosity fracture), the arm must be supported in the desired position of stability. This may require an abduction splint or, historically, a spica cast.
- Duration: Arm supports and immobilizers are generally maintained strictly for the first 3 weeks to allow the subscapularis repair and anterior capsular healing to initiate.
- Exercises: During this phase, active range of motion of the elbow, wrist, and hand is encouraged to prevent distal edema and stiffness.
Phase II: Early Motion (Weeks 3 to 6)
- Hardware Removal: If temporary internal fixation (such as transarticular Kirschner wires) was used to maintain reduction in a highly unstable joint, it is typically removed at the 3 to 4-week mark.
- Pendulum Exercises: At 3 to 4 weeks postoperatively, gentle pendulum (Codman) exercises are initiated.
- Passive and Active-Assisted Motion: Active-assisted and passive motion of the shoulder are introduced shortly thereafter. These exercises must be strictly continued within the ranges of comfort. Aggressive passive stretching, particularly into external rotation, is contraindicated at this stage to protect the subscapularis repair.
Phase III: Strengthening and Functional Return (Weeks 6 and Beyond)
- Active Motion: Progression to full active range of motion is encouraged as tolerated by pain and tissue healing.
- Night Splinting: Because the dynamic stabilizers of the shoulder (rotator cuff and deltoid) have undergone significant atrophy during the chronic dislocation and postoperative immobilization periods, the shoulder remains vulnerable during sleep. The shoulder should probably be supported in a splint at night for several months until fairly strong, active abduction and dynamic stability have been regained.
- Strengthening: Isotonic and isokinetic strengthening of the rotator cuff and periscapular stabilizers begins at 6 to 8 weeks, focusing heavily on the subscapularis and infraspinatus to restore the transverse force couple of the glenohumeral joint.
COMPLICATIONS AND PITFALLS
Surgeons undertaking the open reduction of chronic anterior dislocations must be prepared to manage several high-risk complications:
- Iatrogenic Fractures: As emphasized, the osteopenic humeral head is highly prone to indentation or catastrophic fracture during reduction. Forceful leverage must be avoided. If the head cannot be reduced gently, further soft tissue release (particularly the inferior capsule and coracohumeral ligament) is mandatory.
- Axillary Nerve Injury: The axillary nerve is tethered by scar tissue in chronic dislocations. It must be identified or definitively protected during the inferior capsular release and subscapularis repair. Postoperative deltoid atony should prompt immediate neurologic evaluation.
- Osteonecrosis (Avascular Necrosis): Extensive soft tissue stripping to achieve reduction can compromise the delicate blood supply to the humeral head (primarily the anterior humeral circumflex artery). Patients must be counseled on the risk of late-onset osteonecrosis, which may eventually necessitate prosthetic arthroplasty.
- Postoperative Stiffness: While recurrent instability is a risk, severe postoperative stiffness is far more common following open reduction of chronic dislocations. A meticulous, patient-compliant rehabilitation program is the only defense against a frozen shoulder outcome.
📚 Medical References
You Might Also Like