Total Hip Arthroplasty: Posterolateral Approach, Extensile & Minimally Invasive

Key Takeaway
Looking for accurate information on Total Hip Arthroplasty: Posterolateral Approach, Extensile & Minimally Invasive? The posterior approach is primarily indicated for primary and revision total hip arthroplasty. It is often preferred for complex cases such as stiff or ankylosed hips, congenital hip dislocations requiring femoral shortening, and revisions needing posterior column fixation or extended trochanteric osteotomy. A key advantage is its preservation of abductor musculature, which helps reduce postoperative limp.
Introduction and Epidemiology
Approaching the hip joint from a posterior direction was originally described by the German surgeon Bernard Von Langenbeck. Von Langenbeck's approach was later modified by the Swiss surgeon Theodor Kocher, who used it mainly for the treatment of septic arthritis from Mycobacterium tuberculosis. The posterior approach, as we know it today, was described by Austin T. Moore as the “low posterior approach” or “southern exposure,” because it was more inferior than the traditional posterolateral approach at that time. Historically, this approach was utilized by Moore and others for hip arthroplasty, arthrodesis, and osteotomies for congenital hip dislocations.
The approach has been further modified for arthroplasty into what is commonly referred to as the “mini-posterior” approach that utilizes shorter skin and fascial incisions (6 to 10 cm) by eliminating the proximal and distal-most aspects of the standard posterior incision. Currently, the posterior approach remains the most globally utilized surgical approach for primary and revision total hip arthroplasty (THA), as well as hip hemiarthroplasty for femoral neck fractures.
Epidemiological data from major joint replacement registries, including the National Joint Registry (NJR) of England, Wales, Northern Ireland, and the Isle of Man, as well as the American Joint Replacement Registry (AJRR), consistently demonstrate that the posterior approach is utilized in over 60% of primary THA cases. Its enduring popularity is attributed to its excellent visualization of the acetabulum and proximal femur, its extensile nature, and its preservation of the hip abductor mechanism. As surgical techniques have evolved, the integration of enhanced posterior soft tissue repair (capsulorrhaphy and reattachment of the short external rotators) has dramatically reduced the historical complication of posterior dislocation, bringing instability rates in line with, or lower than, those of anterior and lateral approaches.
Surgical Anatomy and Biomechanics
A profound understanding of the posterior hip anatomy is requisite for safe and efficacious execution of the posterolateral approach. The approach relies on muscle-splitting and muscle-detaching techniques rather than exploiting a true internervous plane.
Superficial Anatomy and Fascial Layers
The superficial dissection involves splitting the gluteus maximus muscle in line with its fibers. The gluteus maximus is innervated by the inferior gluteal nerve (L5, S1, S2). Because the muscle is split rather than retracted entirely, the posterior approach does not utilize a true internervous plane. The split is considered safe as long as it does not extend excessively medial or proximal, which could risk denervating the medial half of the muscle or injuring the superior gluteal neurovascular bundle. Distally, the split transitions into an incision through the iliotibial band and the fascia lata, exposing the vastus lateralis and the greater trochanter.
Deep Musculature and Short External Rotators
Deep to the gluteus maximus lies the crucial layer of the short external rotators of the hip. From superior to inferior, these include the piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and quadratus femoris.
* Piriformis Originates from the anterior sacrum and inserts on the superior aspect of the greater trochanter. It serves as a key anatomical landmark.
* Triceps Coxae Comprising the superior gemellus, obturator internus, and inferior gemellus, these muscles insert into the medial surface of the greater trochanter, superior to the trochanteric fossa.
* Obturator Externus Inserts into the trochanteric fossa and is often preserved during primary THA to maintain inferior stability, though it may be released in stiff hips or revisions.
* Quadratus Femoris Located inferiorly, inserting on the quadrate tubercle. The ascending branch of the medial femoral circumflex artery (MFCA) courses in close proximity to the superior border of the quadratus femoris.
Neurovascular Structures
The sciatic nerve is the most critical structure at risk during the posterior approach. It typically exits the pelvis through the greater sciatic foramen, inferior to the piriformis muscle. However, anatomical variants exist (e.g., the nerve piercing the piriformis or splitting around it), necessitating careful identification and protection. The nerve courses superficial to the short external rotators and deep to the gluteus maximus.
The primary blood supply to the adult femoral head courses posteriorly from branches of the medial femoral circumflex artery. The MFCA gives rise to retinacular vessels that traverse the posterior and superior femoral neck. Therefore, a posterior capsulotomy and release of the short external rotators inherently disrupts this terminal blood supply. While inconsequential in arthroplasty where the femoral head is resected, this anatomy dictates the contraindications for joint-preserving procedures.
Biomechanical Considerations
Perhaps the most important advantage of the posterior approach is that the abductor musculature (gluteus medius and minimus) is preserved. These muscles, innervated by the superior gluteal nerve, are critical for maintaining a level pelvis during the single-leg stance phase of gait. Preservation of the abductors results in a lesser incidence of postoperative limp (Trendelenburg gait) in comparison to the anterolateral or direct lateral approaches (Hardinge approach), which require partial detachment and subsequent repair of the abductor mechanism. Furthermore, the posterior approach allows for excellent restoration of femoral offset and leg length, which are critical biomechanical parameters for optimizing abductor tension and joint reaction forces.
Indications and Contraindications
A major advantage of the posterolateral approach is that it is highly extensile. The standard approach, as used for arthroplasty, can be extended proximally into the Kocher-Langenbeck approach for fixation of the posterior wall of the acetabulum or the posterior column of the pelvis. It can also be extended distally to expose the femur to perform trochanteric osteotomies or to fix periprosthetic femur fractures.
Although primary and revision hip arthroplasty may be performed through multiple different approaches, there are specific scenarios in which a posterior approach is highly preferred. These include total hip replacement in cases requiring trochanteric osteotomy for exposure (the stiff or ankylosed hip), congenital hip dysplasia requiring subtrochanteric femoral shortening osteotomies, revisions in which fixation of the posterior column is required, or revisions of well-fixed femoral components requiring an extended trochanteric osteotomy (ETO) for removal.
Use of the posterior approach is controversial, and often contraindicated, in joint-preserving procedures requiring an arthrotomy, such as drainage of a septic hip, removal of a loose body, or fixation of a femoral head fracture. This is due to profound concerns regarding the disruption of the blood supply to the femoral head. Because the primary blood supply to the adult femoral head courses posteriorly from branches of the MFCA, a posterior capsulotomy risks iatrogenic osteonecrosis (avascular necrosis).
In cases of arthroplasty, the posterior approach may be avoided by some surgeons in favor of direct anterior or anterolateral approaches in patients in whom the risk of dislocation is exceptionally high. This includes patients with severe cognitive impairment, neuromuscular disorders (e.g., Parkinson's disease, cerebral palsy), or those who are non-ambulatory and wheelchair-bound. However, with modern large-diameter femoral heads and robust soft-tissue repair techniques, this is considered only a relative contraindication.
Operative vs Non Operative Indications Summary
| Pathology / Clinical Scenario | Operative Management (Posterior Approach Indicated) | Non-Operative Management or Alternative Approach Indicated |
|---|---|---|
| End-Stage Osteoarthritis | Primary THA via posterior approach (excellent exposure, abductor preservation). | Physical therapy, NSAIDs, intra-articular injections (if surgical risk is prohibitive). |
| Femoral Neck Fracture (Displaced) | Hemiarthroplasty or THA via posterior approach. | Non-operative only in non-ambulatory, high-mortality risk patients (comfort care). |
| Complex Revision THA | Highly indicated due to extensile nature (distal extension for ETO, proximal for column). | N/A (Revision typically mandates surgical intervention). |
| Developmental Dysplasia of the Hip | Indicated when subtrochanteric shortening osteotomy is anticipated. | Mild dysplasia without severe arthritis may be managed conservatively or via PAO. |
| Femoral Head Fracture (Pipkin) | Contraindicated for joint preservation due to MFCA disruption. | Surgical management preferred via Anterior (Smith-Petersen) or Trochanteric Flip approach. |
| Septic Arthritis (Native Hip) | Contraindicated for native joint drainage due to AVN risk. | Anterior arthrotomy or arthroscopic irrigation and debridement preferred. |
| Severe Neuromuscular Disorders | Relative contraindication due to higher posterior dislocation risk. | Consider Direct Anterior approach or dual-mobility articulation if surgery is mandatory. |

Pre Operative Planning and Patient Positioning
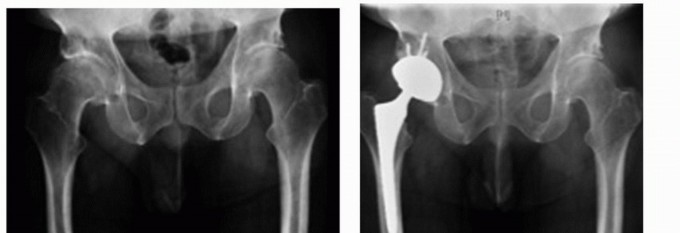
Thorough preoperative planning and precise patient positioning are paramount to the success of a total hip arthroplasty via the posterolateral approach. Planning begins with a comprehensive clinical evaluation and high-quality orthogonal radiographs: an anteroposterior (AP) view of the pelvis centered over the symphysis pubis, and an AP and cross-table lateral view of the operative hip.
Preoperative Templating
Templating, whether manual with acetate overlays or via digital software, is critical for predicting component size, restoring the center of rotation, equalizing leg lengths, and optimizing femoral offset.
1. Acetabular Templating The acetabular component is templated on the AP pelvis radiograph. The goal is to restore the native center of rotation, typically referencing the teardrop and the ilioischial line. The cup should be positioned in approximately 40 degrees of abduction and 15 to 20 degrees of anteversion.
2. Femoral Templating The femoral component is templated to determine the correct stem size, neck length, and offset. The template should fill the metaphysis adequately while restoring the vertical distance from the lesser trochanter to the center of the femoral head (leg length) and the horizontal distance from the center of the head to the central axis of the femur (offset).
Patient Positioning
The patient is placed in the lateral decubitus position on the operating table. The operative hip is positioned superiorly. Rigid pelvic fixation is absolutely critical; if the pelvis rolls anteriorly or posteriorly during the procedure, the surgeon's perception of acetabular version will be distorted, leading to malpositioning of the cup and subsequent instability.
Pelvic fixation is typically achieved using a pegboard system or a vacuum bean bag.
* Anterior Support A pubic post is placed firmly against the pubic symphysis.
* Posterior Support A sacral post is placed against the sacrum, typically at the level of the posterior superior iliac spine (PSIS).
The operating table must be perfectly level, and the patient's torso and pelvis must be strictly perpendicular to the floor. The dependent leg is flexed at the hip and knee to stabilize the patient, while the operative leg is left free to be manipulated through a full range of motion. All bony prominences, particularly the fibular head and lateral malleolus of the dependent leg, must be meticulously padded to prevent pressure necrosis and neurapraxia (e.g., common peroneal nerve palsy).
Detailed Surgical Approach and Technique
The posterolateral approach can be performed without the need for special equipment, such as a fracture table or fluoroscopy, which makes it more cost-effective than some direct anterior approaches. Furthermore, it affords limited risk to damaging the lateral femoral cutaneous nerve, a complication frequently encountered during the direct anterior approach.
Incision and Superficial Dissection
The skin incision is centered over the posterior aspect of the greater trochanter. For a standard approach, the incision begins approximately 5 to 8 cm proximal to the tip of the greater trochanter, curving distally along the posterior border of the trochanter, and extending 5 to 8 cm along the shaft of the femur. In a minimally invasive or "mini-posterior" approach, this incision is reduced to 6 to 10 cm, maintaining the central vector over the trochanter but limiting the proximal and distal extensions.
Subcutaneous tissues are divided in line with the skin incision to expose the fascia lata distally and the gluteus maximus proximally. The fascia lata is incised longitudinally over the center of the greater trochanter. Proximally, this incision is extended by bluntly splitting the fibers of the gluteus maximus. A Charnley or similar self-retaining retractor is placed to maintain exposure.
Deep Dissection and Sciatic Nerve Protection
With the superficial layer retracted, the bursa overlying the posterior trochanter is excised. The hip is internally rotated to place the short external rotators on stretch. The piriformis tendon and the conjoined tendon of the short external rotators (superior gemellus, obturator internus, inferior gemellus) are identified at their insertion on the medial aspect of the greater trochanter.
At this stage, the sciatic nerve should be conceptualized, and if necessary, palpated or visually identified. It lies embedded in fat posterior to the short external rotators. Routine formal exploration of the sciatic nerve is not required unless the anatomy is distorted by previous surgery, severe dysplasia, or post-traumatic deformity. Retractors placed posteriorly must be positioned carefully to avoid compressing or stretching the nerve.
The piriformis and the short external rotators are tagged with heavy non-absorbable sutures and transected close to their femoral insertion. The obturator externus may be preserved or released depending on the required exposure. The tagged muscles are reflected posteriorly, which acts as a protective soft-tissue cushion over the sciatic nerve.
Capsulotomy and Dislocation
The posterior capsule of the hip joint is now exposed. A capsulotomy is performed, typically in a T-shaped, H-shaped, or inverted-U configuration, depending on surgeon preference. Alternatively, a continuous capsular flap can be elevated in continuity with the short external rotators to facilitate a robust repair later.
The hip is then gently dislocated by utilizing a combination of flexion, adduction, and progressive internal rotation. If the hip is stiff or severely osteophytic, aggressive rotational torque must be avoided to prevent iatrogenic spiral fractures of the femoral shaft. In such cases, in situ femoral neck osteotomy may be performed prior to dislocation.
Femoral Neck Resection and Acetabular Preparation
Once dislocated, the femoral neck is resected at the preoperatively templated level and angle, typically referencing the distance from the lesser trochanter. The femoral head is removed from the acetabulum.
Retractors are placed to expose the acetabulum. A typical configuration includes a retractor placed anteriorly over the anterior wall, one inferiorly beneath the transverse acetabular ligament, and a posterior retractor. The labrum and osteophytes are excised to define the true bony margins of the acetabulum. The acetabulum is sequentially reamed to a hemispherical shape, ensuring preservation of the subchondral bone. The acetabular component is then impacted into place, targeting 40 degrees of inclination and 15 to 20 degrees of anteversion. Adjunctive screw fixation may be utilized depending on the press-fit stability.
Femoral Preparation and Trialing
The operative leg is positioned in flexion, adduction, and internal rotation to present the proximal femur. The knee is flexed to 90 degrees, and the tibia points strictly vertical, allowing the surgeon to accurately judge femoral anteversion. The femoral canal is opened with a box osteotome or starter awl, and sequential broaching is performed to prepare the cancellous bone for the femoral stem.
Trial components (neck and head) are placed, and the hip is reduced. A comprehensive stability check is performed:
1. Posterior Stability Assessed by placing the hip in 90 degrees of flexion, adduction, and internal rotation.
2. Anterior Stability Assessed in extension and external rotation.
3. Leg Length and Offset Evaluated by palpating the relationship between the greater trochanter and the center of the femoral head, and comparing soft tissue tension (e.g., the "shuck" test).
Component Implantation and Closure
Following satisfactory trialing, the definitive femoral stem and head are implanted. The hip is reduced for the final time. Copious irrigation is performed.
The most critical step of the closure is the enhanced posterior soft-tissue repair. The posterior capsule and the short external rotators are meticulously repaired back to the greater trochanter. This is typically achieved using transosseous tunnels through the greater trochanter or robust soft-tissue repair to the gluteus medius insertion. This step is essential for minimizing the risk of postoperative posterior dislocation. The fascia lata is closed with heavy sutures, followed by standard closure of the subcutaneous tissues and skin.
Complications and Management
While the posterolateral approach is highly successful, it is associated with specific complications that surgeons must be prepared to manage. Historically, the most significant criticism of the posterior approach was a higher rate of posterior dislocation compared to anterior or lateral approaches. However, the advent of enhanced posterior soft-tissue repair techniques has largely mitigated this discrepancy.
Common Complications and Salvage Strategies
| Complication | Incidence | Etiology / Risk Factors | Prevention and Salvage Strategies |
|---|---|---|---|
| Posterior Dislocation | 0.5% - 2.0% | Component malposition (retroversion), inadequate soft-tissue repair, non-compliance with precautions, neuromuscular disorders. | Prevention: Meticulous capsulorrhaphy and repair of short external rotators. Optimize cup version and femoral offset. Use larger femoral heads (≥32mm). Management: Closed reduction under sedation. If recurrent, revision surgery to correct component malposition or utilize dual-mobility bearings or constrained liners. |
| Sciatic Nerve Palsy | 0.5% - 1.0% | Excessive retraction, limb lengthening >4cm, direct trauma, hematoma compression. | Prevention: Careful retractor placement (avoiding the posterior quadrant deep to the rotators). Release tension on the nerve by flexing the knee if lengthening is significant. Management: Immediate post-op evaluation. If a compressive hematoma is suspected, emergent evacuation. Otherwise, supportive care, AFO for foot drop. Most neurapraxias recover within 6-12 months. |
| Leg Length Discrepancy (LLD) | 1.0% - 3.0% | Inaccurate preoperative templating, failure to reference intraoperative landmarks, prioritizing stability over length. | Prevention: Rigorous templating. Intraoperative measurement from a fixed pelvic pin to a femoral mark. Management: Mild LLD (<1cm) is usually tolerated and managed with a shoe lift. Severe, symptomatic LLD may require revision arthroplasty to adjust modular neck lengths or stem position. |
| Infection (PJI) | 0.5% - 1.5% | Patient comorbidities (diabetes, obesity, smoking), prolonged operative time. | Prevention: Optimization of host factors, perioperative antibiotics, meticulous hemostasis, chlorhexidine preparation. Management: Acute: DAIR (Debridement, Antibiotics, Implant Retention). Chronic: Two-stage revision with antibiotic spacer. |
| Intraoperative Fracture | 0.5% - 1.0% | Forceful dislocation, over-reaming, aggressive broaching of the femur, unrecognized osteopenia. | Prevention: In situ neck cut for stiff hips. Careful sequential broaching. Prophylactic cerclage wiring if a fissure is noted. Management: Intraoperative cerclage wiring for calcar cracks. Long-stem revision bypass for diaphyseal fractures. |
Post Operative Rehabilitation Protocols
The rehabilitation protocol following a posterior approach THA is designed to restore mobility, strengthen the preserved abductor musculature, and prevent dislocation during the early phase of soft-tissue healing.
Standard Posterior Precautions
Traditionally, patients are placed on "posterior hip precautions" for 6 to 12 weeks postoperatively to protect the posterior capsular repair. These precautions typically include:
1. No hip flexion past 90 degrees.
2. No adduction of the operative leg across the midline of the body.
3. No internal rotation of the operative leg.
Patients are instructed on safe methods for transferring from bed to chair, utilizing elevated toilet seats, and avoiding low chairs or deep squatting.
Modern ERAS Protocols
With the implementation of Enhanced Recovery After Surgery (ERAS) pathways and robust posterior soft-tissue repairs, many high-volume arthroplasty centers are liberalizing or entirely discarding strict posterior precautions. Recent literature suggests that in primary THA with large diameter heads (≥32mm) and meticulous capsulorrhaphy, the removal of strict precautions does not increase the dislocation rate but significantly improves early patient satisfaction and return to function.
Weight-bearing is typically allowed as tolerated (WBAT) immediately postoperatively, utilizing a walker or crutches for balance. Physical therapy focuses on gait training, abductor strengthening (which is facilitated by the preservation of the gluteus medius and minimus during the approach), and progressive range of motion. Chemical and mechanical deep vein thrombosis (DVT) prophylaxis is strictly enforced per institutional and national guidelines.
Summary of Key Literature and Guidelines
The evolution and validation of the posterolateral approach are heavily documented in orthopedic literature.
- Moore AT (1957): Austin T. Moore's original description of the "southern exposure" established the foundation for the modern posterior approach, highlighting its simplicity, excellent exposure, and avoidance of the abductor mechanism.
- Pellicci et al. (1998): A landmark study that revolutionized the posterior approach by introducing the enhanced posterior soft-tissue repair. Pellicci demonstrated that meticulous repair of the posterior capsule and short external rotators reduced the dislocation rate from over 4% to less than 1%, effectively neutralizing the primary criticism of the approach.
- Masonis and Bourne (2002): A comprehensive meta-analysis comparing surgical approaches in THA. The study confirmed that while the posterior approach historically had higher dislocation rates without repair, the implementation of soft-tissue repair techniques yielded dislocation rates comparable to the anterolateral approach, while maintaining superior outcomes regarding postoperative limp and abductor function.
- American Academy of Orthopaedic Surgeons (AAOS) Guidelines: Current clinical practice guidelines do not mandate a specific surgical approach for THA, noting that excellent outcomes can be achieved with posterior, anterior, and lateral approaches. The choice of approach should be dictated by surgeon experience, patient anatomy, and the specific indications of the case. The guidelines emphasize that the posterior approach remains a highly versatile, extensile, and safe option for both primary and complex revision arthroplasty.
You Might Also Like


