Secondary Repair of Extensor Tendons: A Comprehensive Surgical Guide
Key Takeaway
Secondary repair of extensor tendons presents unique surgical challenges due to tendon retraction, muscle contracture, and soft tissue deficits. This comprehensive guide details the indications, biomechanics, and operative techniques for delayed extensor tendon reconstruction. Emphasizing thumb extensor zones (TI-TIV), it provides step-by-step protocols for direct repair, tendon grafting, and tendon transfers, ensuring optimal functional recovery and adherence to evidence-based postoperative rehabilitation protocols.
INTRODUCTION TO SECONDARY EXTENSOR TENDON REPAIR
The management of extensor tendon injuries is a foundational component of hand and upper extremity surgery. While primary repair (performed within the first 24 to 48 hours) is the gold standard, surgeons frequently encounter delayed presentations. Secondary repair is generally defined as reconstruction performed after 4 to 6 weeks from the initial injury. By this time, the proximal tendon segment has typically retracted, the muscle belly has undergone myostatic contracture, and the tendon ends may be encased in dense fibrotic scar tissue.
In cases where a segment of the tendon has been destroyed—whether through crush injury, severe abrasion, or avulsion—direct end-to-end approximation becomes biomechanically impossible without excessive tension. The surgical armamentarium for secondary reconstruction must therefore include advanced techniques such as side-to-side tenodesis, segmental tendon grafting, and regional tendon transfers.
Clinical Pearl: When evaluating a secondary extensor tendon deficit, always assess the passive range of motion of the affected joints first. Tendon reconstruction is futile in the presence of fixed joint contractures. Preoperative hand therapy to maximize passive motion is a mandatory prerequisite to surgical intervention.
BIOMECHANICS AND PREOPERATIVE CONSIDERATIONS
Pathophysiology of the Delayed Presentation
When an extensor tendon is severed, the unopposed resting tone of the corresponding muscle belly causes proximal retraction. Over a period of 4 to 6 weeks, the muscle undergoes structural changes, including sarcomere loss and interstitial fibrosis, leading to a fixed contracture. Concurrently, the empty tendon sheath collapses and fills with fibroblastic scar tissue.
If multiple tendons have been abraded or avulsed, or if the muscle has been denervated and become fibrotic, the native muscle-tendon unit may no longer be viable. In these severe scenarios, transferring a suitable, expendable muscle—such as the flexor carpi ulnaris (FCU) or flexor carpi radialis (FCR)—to the distal extensor segment is required to restore active extension.
Surgical Options for Secondary Repair
The reconstructive ladder for secondary extensor tendon repair includes:
* Direct Suture: Possible only if the tendon ends can be mobilized and approximated with minimal tension (usually limited to specific anatomical zones where retraction is anatomically blocked).
* Side-to-Side Suture (Tenodesis): Suturing the distal stump of the injured tendon to an adjacent, intact synergistic extensor tendon (e.g., attaching a lacerated extensor digitorum communis [EDC] of the ring finger to the intact EDC of the middle finger).
* Segmental Tendon Grafting: Utilizing autografts (palmaris longus, plantaris, or toe extensors) to bridge the gap. This requires a viable proximal muscle belly with adequate excursion.
* Tendon Transfer: Rerouting an expendable, functioning muscle-tendon unit (e.g., Extensor Indicis Proprius [EIP]) to the distal stump of the injured tendon.
MANAGEMENT OF THUMB EXTENSORS: ZONE-SPECIFIC PROTOCOLS
The thumb extensor mechanism is anatomically distinct from the triphalangeal digits, necessitating a highly specific approach to secondary repair based on the zone of injury.
Zones TI and TII: Interphalangeal Joint and Proximal Phalanx
Zone TI encompasses the thumb interphalangeal (IP) joint, while Zone TII overlies the proximal phalanx. Injuries in these distal zones present unique anatomical advantages for secondary repair.
Anatomy and Retraction Dynamics
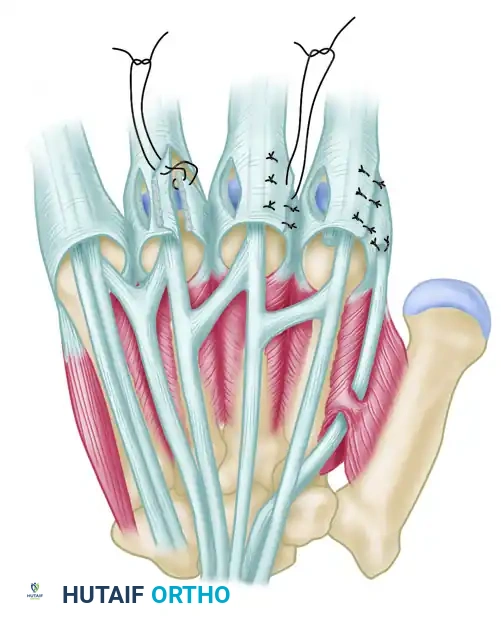
When the extensor pollicis longus (EPL) tendon is divided at or distal to the IP joint, the proximal segment does not retract appreciably. This is due to the robust insertions of the intrinsic thumb muscles—specifically the adductor pollicis, abductor pollicis brevis (APB), and extensor pollicis brevis (EPB)—into the extensor expansion. These attachments act as an anatomical tether, holding the proximal EPL stump in the vicinity of the MCP joint.
Surgical Technique for Zones TI and TII
Because of this tethering effect, the tendon can often be repaired primarily or secondarily without the need for grafting or tendon transfer, even weeks after the injury.
- Approach: A dorsal lazy-S or mid-lateral incision is utilized to expose the extensor expansion.
- Debridement: The tendon ends are identified and conservatively debrided to healthy, parallel collagen bundles.
- Tenorrhaphy: A 4-0 non-absorbable synthetic core suture (e.g., modified Kessler or cruciate technique) is placed. This must be supplemented with a 5-0 or 6-0 epitendinous cross-stitch or running locking suture to optimize biomechanical strength and minimize gap formation during early healing.
- Joint Fixation: To protect the repair, transarticular pinning of the IP joint is highly recommended. A 0.045-inch Kirschner wire (K-wire) is driven across the IP joint in full extension.
- Postoperative Protocol: The transarticular K-wire remains in place for 3 to 4 weeks. During this time, active motion of the metacarpophalangeal (MCP) joint is permitted and encouraged to prevent adherence of the proximal extensor mechanism. Following pin removal, static splinting is maintained for an additional 3 to 4 weeks. Active IP joint motion is initiated only after this total 6-to-8-week period of protection.
Surgical Pitfall: Associated fractures of the distal phalanx involving 50% or more of the articular surface, or fractures presenting with distal fragment subluxation, cannot be treated with soft-tissue repair alone. These require formal open reduction and internal fixation (ORIF) prior to, or concurrent with, tendon repair.
Closed Injuries in Zones TI and TII
Closed ruptures or avulsions of the EPL in these zones (analogous to mallet finger injuries) may be treated non-operatively, even in delayed presentations. Prolonged continuous splinting of the IP joint in extension for 8 or more weeks is the treatment of choice, provided the joint is passively correctable.
Zones TIII and TIV: Metacarpophalangeal Joint and Metacarpal
Zone TIII overlies the MCP joint, and Zone TIV encompasses the thumb metacarpal up to the wrist. Injuries in these zones are notorious for rapid and severe tendon retraction.
Anatomy and Retraction Dynamics
Unlike distal injuries, when the EPL or EPB is divided at the MCP joint or more proximally, there are no intrinsic tethers to prevent retraction. The proximal segment retracts rapidly into the forearm. By 1 month post-injury, a fixed myostatic contracture of the muscle belly has almost universally developed.
Overcoming Contracture: Rerouting the EPL
If a secondary repair is attempted within the first few weeks, the surgeon may find a gap that cannot be closed by simple traction.
1. Lister's Tubercle Release: The contracture can often be overcome by releasing the third dorsal compartment and rerouting the EPL tendon out from around Lister's tubercle.
2. Straight-Line Transposition: By placing the EPL in a straight line from the musculotendinous junction to the thumb, the anatomical detour is bypassed, effectively gaining 1 to 2 centimeters of functional length.
3. Repair: If this maneuver allows the tendon ends to meet with minimal tension (the tendon should not blanch, and the wrist should not need to be acutely extended to maintain coaptation), a direct core and epitendinous repair is performed.
Surgical Warning: Attempting to primarily repair an EPL tendon in Zone III/IV under excessive tension will inevitably lead to repair rupture or a severe extension contracture of the thumb. If rerouting does not provide sufficient length, you must proceed to a tendon transfer or interposition graft.
Extensor Indicis Proprius (EIP) to EPL Transfer
When direct repair is impossible due to gap size or muscle fibrosis, the transfer of the EIP to the distal EPL stump is the gold standard reconstructive procedure. The EIP is synergistic, has appropriate excursion, and its harvest leaves a negligible extensor deficit in the index finger (provided the EDC to the index is intact).
Step-by-Step EIP Transfer Technique:
1. Incision and Identification: A transverse incision is made over the index MCP joint. The EIP is identified ulnar and volar to the EDC tendon of the index finger.
2. Harvest: The EIP is divided just proximal to the extensor hood. The distal stump of the EIP is sutured to the adjacent EDC to prevent extensor lag of the index finger.
3. Proximal Dissection: A second incision is made over the dorsal wrist (fourth compartment). The EIP is withdrawn into the wrist incision.
4. Routing: A subcutaneous tunnel is created from the wrist incision to the thumb MCP joint incision (where the distal EPL stump is located). The tunnel must be wide enough to allow frictionless gliding.
5. Weave and Tensioning: The EIP is woven into the distal EPL stump using a Pulvertaft weave. Tensioning is critical: with the wrist in neutral, the thumb should rest in full extension. The weave is secured with multiple 4-0 non-absorbable mattress sutures.
BIOLOGICAL CONSIDERATIONS AND ADHESION PREVENTION
The success of secondary extensor tendon repair is heavily dependent on the biological environment of the healing tendon. The extensive literature on tendon healing highlights the delicate balance between achieving sufficient biomechanical strength and preventing restrictive peritendinous adhesions.
The Role of Suture Technique
Biomechanical studies demonstrate that the strength of a tendon repair is directly proportional to the number of core suture strands crossing the repair site and the caliber of the suture material. However, increasing the bulk of the repair (e.g., using 6-strand or 8-strand techniques) increases the gliding resistance within the extensor retinaculum. For secondary extensor repairs, a 4-strand core repair utilizing a locking technique (which provides superior resistance to gap formation during cyclical loading compared to grasping techniques) is generally preferred. The addition of a peripheral epitendinous suture not only increases the ultimate tensile strength by 10% to 50% but also smooths the repair site, significantly reducing gliding resistance and subsequent adhesion formation.
Modulating the Healing Environment
In secondary repairs, the tendon sheath is often compromised, and the surrounding soft tissue bed may be heavily scarred. Research into biological modulation has explored several avenues to mitigate adhesion formation:
* Hyaluronic Acid and Phospholipids: Application of these substances at the repair site has been shown in animal models to reduce peritendinous adhesions by providing a boundary lubrication layer.
* Amniotic Membrane and Seprafilm: Physical barriers can be utilized in severe cases where the tendon must glide over a scarred bony bed (e.g., following a concomitant metacarpal fracture).
* Growth Factors: While still largely experimental, the up-regulation of Transforming Growth Factor-beta (TGF-β) and Basic Fibroblast Growth Factor (bFGF) plays a critical role in tenocyte proliferation and collagen synthesis. Future therapies may utilize targeted growth factor delivery to accelerate intrinsic tendon healing while minimizing extrinsic scar formation.
POSTOPERATIVE REHABILITATION PROTOCOLS
The postoperative management of secondary extensor tendon repairs requires a highly disciplined approach, balancing the need to protect the compromised repair with the necessity of early motion to prevent adhesions.
Immobilization vs. Early Active Motion
Historically, extensor tendon repairs were treated with static immobilization for 4 to 6 weeks. However, modern protocols favor controlled early motion to enhance intrinsic tendon healing and improve ultimate excursion.
- Static Splinting (Traditional): Indicated for non-compliant patients, children, or cases where the soft tissue bed is tenuous (e.g., following complex grafting). The wrist is splinted in 30° to 40° of extension, with the MCP joints in 0° to 10° of flexion.
- Early Passive Motion (Dynamic Splinting): A dynamic extension splint allows active flexion of the digits against rubber band traction, which then passively extends the digits. This provides tendon excursion (3-5 mm is required to prevent dense adhesions) while protecting the repair from active contractile forces.
- Early Active Motion (EAM): Reserved for robust repairs (minimum 4-strand core + epitendinous suture). EAM protocols utilize a relative motion extension splint or a place-and-hold technique. The patient actively maintains extension after the therapist passively places the digit in the extended position.
Specific Protocol for Thumb Extensor Reconstruction
Following an EIP to EPL transfer or a complex secondary repair of the thumb extensors:
* Weeks 0-3: The thumb and wrist are immobilized in a forearm-based thumb spica splint. The wrist is positioned in 30° of extension, the thumb CMC in radial abduction, and the MCP/IP joints in full extension.
* Weeks 3-4: If transarticular pins were used, they are removed. A removable thermoplastic splint is fabricated. Gentle active range of motion of the thumb is initiated out of the splint.
* Weeks 4-6: Active flexion and extension exercises are progressed. The splint is worn between exercise sessions and at night.
* Weeks 6-8: Splinting is discontinued. Progressive strengthening is initiated.
* Weeks 8-12: Unrestricted use of the hand is gradually permitted.
COMPLICATIONS AND SALVAGE PROCEDURES
Despite meticulous surgical technique, secondary extensor tendon repairs carry a higher complication rate than primary repairs.
- Tendon Rupture: Usually occurs between weeks 2 and 4 when the repair is at its weakest (the fibroblastic phase). Rupture requires prompt re-exploration and often necessitates a tendon transfer, as the tendon ends will be severely frayed.
- Extensor Lag: A common complication resulting from either stretching of the repair site (gap formation) or restrictive adhesions proximal to the joint. Mild lags (<15°) are often well-tolerated. Severe lags may require secondary tenolysis (performed no earlier than 3 to 6 months postoperatively) or a secondary tendon transfer.
- Joint Contracture: Aggressive therapy is the first line of treatment. If a fixed flexion contracture persists, a dorsal capsulotomy may be required in conjunction with tenolysis.
CONCLUSION
Secondary repair of extensor tendons is a complex surgical endeavor that demands a profound understanding of hand biomechanics, tendon healing biology, and advanced reconstructive techniques. Whether managing a tethered EPL laceration at the interphalangeal joint or executing a complex EIP tendon transfer for a retracted Zone IV injury, the surgeon must meticulously balance tension, glide, and biological viability. Adherence to strict, evidence-based surgical principles and rigorous postoperative rehabilitation protocols is paramount to restoring optimal function to the injured hand.
📚 Medical References
- extensor tendon repair in zones V to VII, J Hand Surg 28B:224, 2003.
- Cannon NM, Strickland JW: Therapy following fl exor tendon surgery, Hand Clin 1:147, 1985.
- Chow JA, Dovelle S, Thomas LJ, et al: A comparison of results of extensor tendon repair followed by early controlled mobilisation versus static immobilisation, J Hand Surg 14B:18, 1989.
- Chow JA, Thomes LJ, Dovelle S, et al: A combined regimen of controlled motion following fl exor tendon repair in “no man’s land,” Plast Reconstr Surg 79:447, 1987.
- Chow JA, Thomes LJ, Dovelle S, et al: Controlled motion rehabilitation after fl exor tendon repair and grafting, J Bone Joint Surg 70B:591, 1988.
- Crosby CA, Wehbé MA: Early motion after extensor tendon surgery, Hand Clin 12:57, 1996.
- Duran RJ, Houser RG: Controlled passive motion following fl exor tendon repair in zones 2 and 3. In American Academy of Orthopaedic Surgeons: Symposium on tendon surgery in the hand, St Louis, 1975, Mosby. Duran RJ, Houser RG, Coleman CR, et al: A preliminary report in the use of controlled passive motion following fl exor tendon repair in zones II and III, J Hand Surg 1:79, 1976.
- Evans RB: Immediate active short arc motion following extensor tendon repair, Hand Clin 11:483, 1995.
- Gerbino PG, Saldana MJ, Westerbeck P, et al: Complications experienced in the rehabilitation of zone I fl exor tendon injuries with dynamic traction splinting, J Hand Surg 16A:680, 1991.
- Hagberg L, Selvik G: Tendon excursion and dehiscence during early controlled mobilization after fl exor tendon repair in zone II: an x-ray stereophotogrammetric analysis, J Hand Surg 16A:669, 1991.
- Ip WY, Chow SP: Results of dynamic splintage following extensor tendon repair, J Hand Surg 22B:283, 1997.
- Jansen CWS, Watson MG: Measurement of range of motion of the fi nger after fl exor tendon repair in zone II of the hand, J Hand Surg 18A:411, 1993.
- Karlander LE, Berggren M, Larsson M, et al: Improved results in zone 2 fl exor tendon injuries with a modifi ed technique of immediate controlled mobilization, J Hand Surg 18B:26, 1993.
- Kerr CD, Burczak JR: Dynamic traction after extensor tendon repair in zones 6, 7, and 8: a retrospective study, J Hand Surg 14B:21, 1989.
- Kitsis CK, Wade PJF, Krikler SJ, et al: Controlled active motion following primary fl exor tendon repair: a prospective study over 9 years, J Hand Surg 23B:344, 1998.
- Kubota H, Manske PR, Aoki M, et al: Effect of motion and tension on injured fl exor tendons in chickens, J Hand Surg 21A:456, 1996.
- Kutz JE: Controlled mobilization of acute fl exor tendon injuries: Louisville technique. In Hunter JM, Schneider LH, Mackin EJ, eds: Tendon surgery in the hand, St Louis, 1987, Mosby. May EJ, Silfverskiöld KL: Rate of recovery after fl exor tendon repair in zone II: a prospective longitudinal study of 145 digits, Scand J Plast Reconstr Hand Surg 27:89, 1993.
- May EJ, Silfverskiöld KL, Sollerman CJ: Controlled mobilization after fl exor tendon repair in zone II: a prospective comparison of three methods, J Hand Surg 17A:942, 1992.
- May EJ, Silfverskiöld KL, Sollerman CJ: The correlation between controlled range of motion with dynamic traction and results after fl exor tendon repair in zone II, J Hand Surg 17A:1133, 1992.
- Minamikawa Y, Peimer CA, Yamaguchi T, et al: Wrist position and extensor tendon amplitude following repair, J Hand Surg 17A:268, 1992.
- Newport ML, Shukla A: Electrophysiologic basis of dynamic extensor splinting, J Hand Surg 17A:272, 1992.
- Panchal J, Mehdi S, Donoghue JO, et al: The range of excursion of fl exor tendons in zone V: a comparison of active vs. passive fl exion mobilisation regimes, Br J Plast Surg 50:517, 1997.
- Saldana MJ, Choban S, Westerbeck P, et al: Results of acute zone III extensor injuries treated with dynamic extension splinting, J Hand Surg 16A:1146, 1991.
- Schenck RR, Lenhart DE: Results of zone II fl exor tendon lacerations in civilians treated by the Washington regimen, J Hand Surg 21A:984, 1996.
- Silfverskiöld KL, May EJ: Flexor tendon repair in zone II with a new suture technique and an early mobilization program combining passive and active fl exion, J Hand Surg 19A:53, 1994.
- Silfverskiöld KL, May EJ, Törnvall AH: Flexor digitorum profundus tendon excursions during controlled motion after fl exor tendon repair in zone II: a prospective clinical study, J Hand Surg 17A:122, 1992.
- Silfverskiöld KL, May EJ, Törnvall AH: Tendon excursions after fl exor tendon repair in zone II: results with a new controlledmotion program, J Hand Surg 18A:403, 1993.
- Stewart KM: Review and comparison of current trends in the postoperative management of tendon repair, Hand Clin 7:447, 1991.
- Strickland JW, Glogovac SV: Digital function following fl exor tendon repair in zone II: a comparison of immobilization and controlled passive motion techniques, J Hand Surg 5:537, 1980.
- Sylaidis P, Youatt M, Logan A: Early active mobilization for extensor tendon injuries, J Hand Surg 22B:594, 1997.
- Tang JB, Gu YT, Rice K, et al: Evaluation of four methods of fl exor tendon repair for postoperative active mobilization, Plast Reconstr Surg 107:742, 2001.
- Thomes LJ, Thomes BJ: Early mobilization method for surgically repaired zone II extensor tendons, J Hand Ther 8:195, 1995.
- Vucekovich K, Gallardo G, Fiala K: Rehabilitation after fl exor tendon repair, reconstruction, and tenolysis, Hand Clin 21:257, 2005.
- Wada A, Kubota H, Miyanishi K, et al: Comparison of postoperative early active mobilization and immobilization in vivo utilizing a four-strand fl exor tendon repair, J Hand Surg 26B:301, 2001.
- Tendon Repair Aoki M, Manske P, Pruitt DL, et al: Work of fl exion after fl exor tendon repair according to the placement of sutures, Clin Orthop Relat Res 320:205, 1995.
- Aoki M, Manske PR, Pruitt DL, et al: Work of fl exion after tendon repair with various suture methods, J Hand Surg 20B:310, 1995.
- Amadio PC, Cooney WP: Current concepts of fl exor tendon repair, Adv Orthop Surg 10:207, 1987.
- Angeles JG, Heminger H, Mass DP: Comparative biomechanical performances of 4-strand core suture repairs for zone II fl exor tendon lacerations, J Hand Surg 27A:508, 2002.
- Aslam A, Afoke A: A new core suture technique for fl exor tendon repair: biomechanical analysis of tensile strength and gap formation, J Hand Surg 25B:390, 2000.
- Barrie KA, Tomak SL, Cholewicki J, et al: Effect of suture locking and suture caliber on fatigue strength of fl exor tendon repairs, J Hand Surg 26A:340, 2001.
- Barrie KA, Tomak SL, Cholewicki J, et al: The role of multiple strands and locking sutures on gap formation of fl exor tendon repairs during cyclical loading, J Hand Surg 25A:714, 2000.
- Barrie KA, Wolfe SW, Shean C, et al: A biomechanical comparison of multistrand fl exor tendon repairs using an in situ testing model, J Hand Surg 25A:499, 2000.
- Boardman ND 3rd, Morifusa S, Saw SS, et al: Effects of tenorraphy on the gliding function and tensile properties of partially lacerated canine digital fl exor tendons, J Hand Surg 24A:302, 1999.
- Brunelli G, Vigasio A, Brunelli F: Slip-knot fl exor tendon suture in zone II allowing immediate mobilization, Hand 15:352, 1983.
- Bruner JM: Surgical exposure of the fl exor pollicis longus tendon, Hand 7:241, 1975.
- Bunnell S: The early treatment of hand injuries, J Bone Joint Surg 33A:807, 1951.
- Burt JD, Siddins M, Morrison WA: Laser photo irradiation in digital fl exor tendon repair, Plast Reconstr Surg 108:688, 2001.
- Dona E, Gianoutsos MP, Walsh WR: Optimizing biomechanical performance of the 4-strand cruciate fl exor tendon repair, J Hand Surg 29A:571, 2004.
- Dona E, Turner AWL, Gianoutsos MP, et al: Biomechanical properties of four circumferential fl exor tendon suture techniques, J Hand Surg 28A:824, 2003.
You Might Also Like