Open Reduction of Chronic Elbow Dislocations: A Comprehensive Surgical Guide
Key Takeaway
Open reduction of chronic elbow dislocations is a complex orthopedic challenge. Success is inversely proportional to the time elapsed since injury. The procedure requires meticulous ulnar nerve decompression, extensive capsuloligamentous release, and triceps lengthening. Post-reduction stability is often compromised, necessitating transarticular pinning, ligament reconstruction, or hinged external fixation to permit early range of motion and optimize functional recovery in the neglected elbow.
Introduction to Chronic Elbow Dislocations
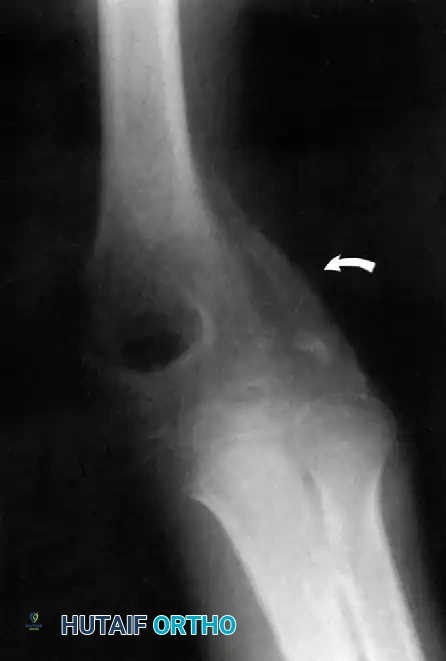
Neglected or chronic posterior dislocations of the elbow represent a formidable challenge in orthopedic surgery. While relatively rare in modern healthcare systems due to advanced imaging and prompt acute care, they remain a significant source of morbidity in developing regions or in patients with delayed presentations.
Although some authors have reported that patients can regain a useful range of flexion-extension after the open reduction of old posterior dislocations—regardless of the patient's age or the duration of the unreduced state—the overwhelming consensus in the literature dictates a more cautious prognosis. Most evidence-based reports confirm that the likelihood of restoring useful, pain-free function by open reduction alone is inversely proportional to the length of time from injury to surgery.
Prolonged dislocation leads to severe soft-tissue contractures, articular cartilage degradation, and heterotopic ossification, necessitating a highly systematic, extensive surgical approach to restore joint congruity and kinematics.
Clinical Pearl: Elbow arthroplasty (Total Elbow Arthroplasty - TEA) may be the most appropriate and predictable choice for the most chronic, difficult cases, particularly in elderly, low-demand patients with severe articular destruction. However, in young, high-demand patients, joint-preserving open reduction remains the gold standard.
Pathoanatomy and Preoperative Considerations
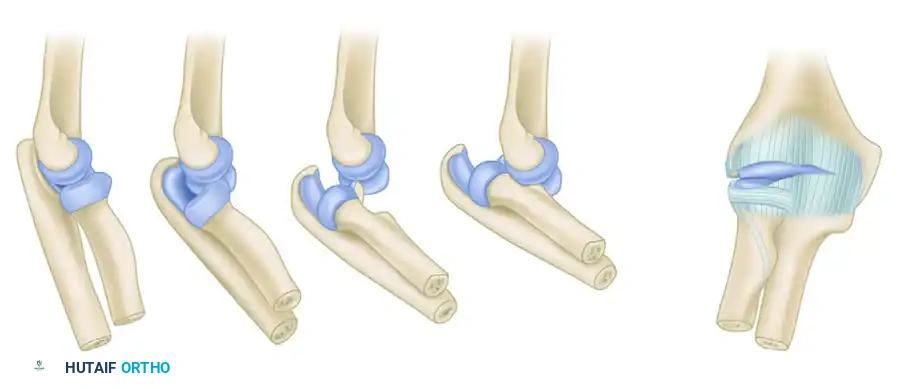
Understanding the pathoanatomy of a chronic elbow dislocation is critical for successful surgical planning. Over time, the displaced joint undergoes profound structural changes:
- Triceps Contracture: The triceps brachii muscle shortens significantly, acting as a major tether preventing anatomical reduction.
- Capsuloligamentous Contracture: The medial collateral ligament (MCL) and lateral collateral ligament (LCL) complexes become fibrotic, shortened, and scarred to the displaced humeral condyles.
- Fibrous Pannus Formation: Dense fibrous tissue fills the olecranon and coronoid fossae, obliterating the normal articular spaces.
- Heterotopic Ossification: A "radial humeral horn" or other forms of periarticular ossification frequently develop due to chronic periosteal stripping and organized hematoma.
Ulnar Nerve Management
It is an absolute surgical mandate to inspect and decompress the ulnar nerve in all patients requiring open reduction for a chronic elbow dislocation. The nerve is often encased in scar tissue, stretched over the displaced medial epicondyle, or distorted by heterotopic bone. Silva advocated for the routine anterior transposition of the ulnar nerve, particularly in series where the average delay in treatment ranged from 19 to 24 months.
Surgical Positioning and Setup
- Anesthesia: General anesthesia combined with a regional block (e.g., supraclavicular or axillary nerve block) is recommended for optimal muscle relaxation and postoperative pain control.
- Positioning: The patient is typically placed in the lateral decubitus position with the operative arm draped over a padded bolster. Alternatively, the prone position can be utilized. Both positions allow excellent access to the posterior compartment of the elbow.
- Tourniquet: A sterile non-exsanguinating tourniquet is applied high on the brachium. Exsanguination by elevation rather than an Esmarch bandage is preferred if deep venous thrombosis is a concern, though standard Esmarch exsanguination is typical.
Surgical Technique: The Speed Procedure
The Speed technique utilizes a V-Y lengthening of the triceps to overcome the profound posterior contracture, combined with extensive capsular releases.
Step 1: Incision and Exposure
Make a generous longitudinal incision over the posterolateral aspect of the elbow. Begin in the midline approximately 10 cm proximal to the olecranon. Continue the incision distally to just proximal to the tip of the olecranon, curving slightly laterally over the lateral humeral condyle and the radial head. Extend the incision further distally for about 5 cm onto the proximal forearm.
Undermine and retract the edges of the wound to expose the tendinous insertion and aponeurosis of the triceps muscle on the posterior aspect of the elbow.
Step 2: Ulnar Nerve Neurolysis
Before any deep dissection or release is performed on the medial side, locate the ulnar nerve. Dissect it meticulously from its bed along the groove in the medial humeral condyle. Perform a thorough neurolysis and carefully retract the nerve using a vessel loop. Depending on the tension and chronicity, prepare the nerve for an anterior subcutaneous or submuscular transposition.
Step 3: Triceps V-Y Lengthening
Beginning proximally and using sharp dissection, reflect the aponeurosis of the triceps distally to form a flap of tissue that remains attached to the olecranon.
To perform the V-Y lengthening:
* Begin 7.5 cm proximal to the joint.
* Make an inverted "V" incision in the midline of the arm through the fibers of the triceps muscle, extending distally toward the olecranon.
* Curve this deep incision around the lateral edge of the olecranon to meet the distal end of the skin incision.
Step 4: Subperiosteal Release and Joint Debridement
Subperiosteally free all muscle attachments from the distal humerus, both anteriorly and posteriorly.
Proceed to release the attachments of the joint capsule and the shortened collateral ligaments around the condyles of the humerus.
Surgical Warning: Significant difficulty may be encountered when freeing the tissues around the medial condyle and along the anterior surface of the humerus just above the joint. Extreme care must be taken to protect the median nerve and brachial artery anteriorly.
It is essential that all contracted tissues are loosened and the distal end of the humerus is completely mobilized. Remove all fibrous tissue interposed between the distal humerus and the ulna. If a radial humeral horn of ossification is present, it must be divided and excised to permit reduction.
Step 5: Joint Reduction
Once the distal humerus is completely mobilized and the fossae are cleared of fibrous debris, gently manipulate the forearm to reduce the ulnohumeral and radiohumeral joints. Avoid excessive levering forces, as the osteopenic bone is highly susceptible to iatrogenic fracture.
Post-Reduction Stabilization Strategies
After reduction, the elbow is frequently grossly unstable due to the extensive release of the collateral ligaments and capsule. Achieving stability is paramount to allow for early rehabilitation. Several strategies exist, ranging from static pinning to dynamic external fixation.
1. Transarticular Pinning
For stability, some authors advocate the use of Kirschner wires or Steinmann pins. The pins are driven transarticularly, transfixing the olecranon to the humerus, or transfixing the capitellum to the radial head.
Mehta et al. and Elzohairy both reported good functional improvement in patients treated with complete capsular and ligamentous release, a Speed V-Y lengthening, and Kirschner wire joint fixation.
* Protocol: Pins are typically removed at 2 weeks postoperatively to initiate range-of-motion exercises. A protective sling is continued for 6 weeks or more when the patient is not actively exercising.
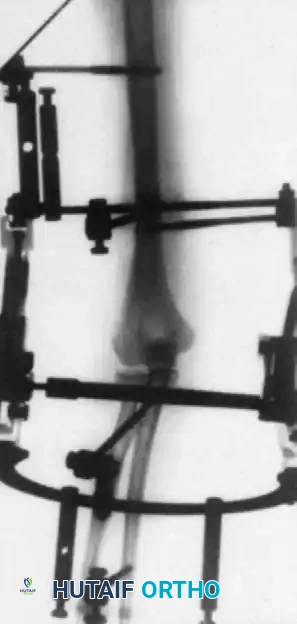
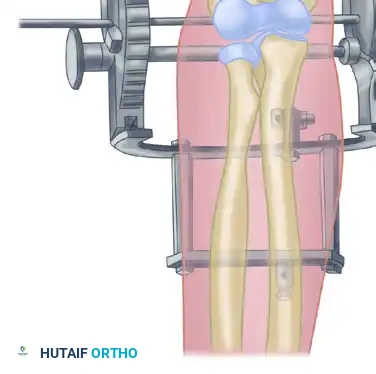
2. Hinged External Fixation
Many contemporary orthopedic surgeons prefer the application of a hinged external fixator. Although technically more complex and resource-intensive, a hinged fixator maintains concentric joint reduction while allowing immediate, guided range of motion. This theoretically improves cartilage nutrition, reduces intra-articular adhesion formation, and optimizes functional results.

Surgical Pitfall: The axis of the hinged external fixator must perfectly align with the anatomical axis of elbow rotation (passing through the center of the capitellum and the anteroinferior aspect of the medial epicondyle). Malalignment will lead to eccentric loading, subluxation, and rapid pin loosening.
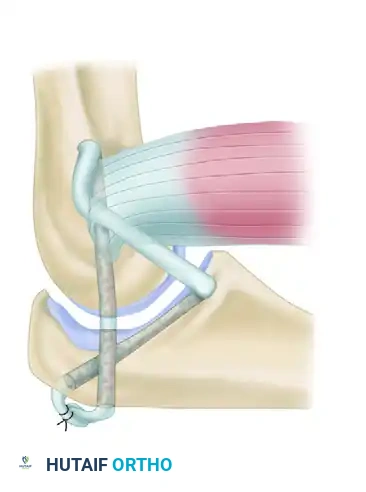
3. Ligament Reconstruction (The Arafiles Technique)
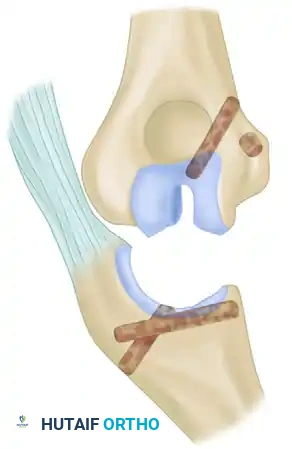
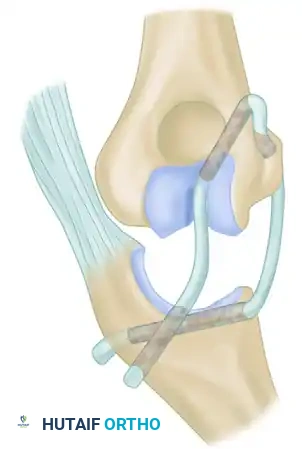
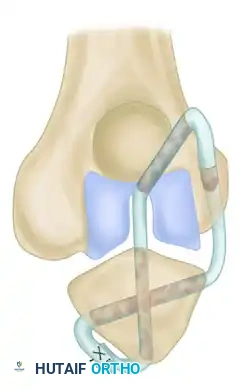
In cases of profound instability where dynamic fixation is unavailable or insufficient, surgeons may opt for ligament reconstruction with or without adjunctive fixation. The Arafiles technique utilizes a tendon graft routed through precisely drilled osseous tunnels to recreate the stabilizing vectors of the collateral ligaments.
The following sequence illustrates the complex reconstruction for an old posterior dislocation of the elbow, demonstrating the slot created in the trochlea and the specific lines of drill holes (A to D) that dictate the course of the tendon graft.


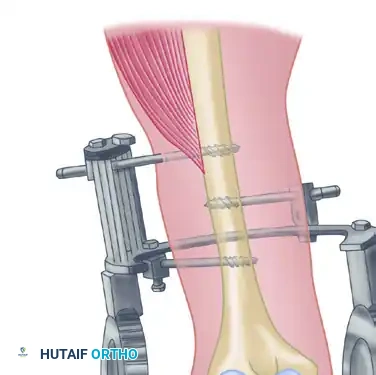

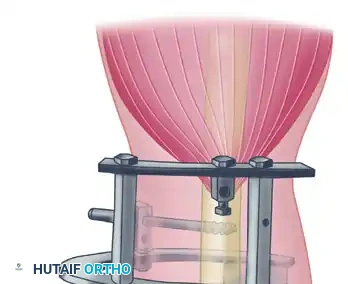

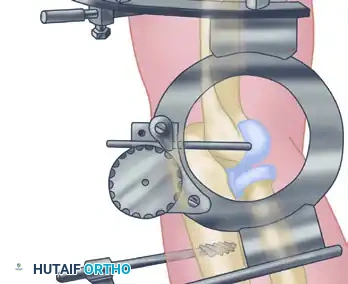
Note the intact forearm flexor origin during the completed repair, which provides secondary dynamic stability to the medial aspect of the reconstructed joint.
Postoperative Protocol and Rehabilitation
The postoperative rehabilitation protocol must strike a delicate balance between protecting the tenuous soft-tissue repairs and preventing recurrent stiffness.
- Phase I (0-2 Weeks): If transarticular pins are used, the elbow is immobilized in a well-padded posterior splint at 90 degrees of flexion. If a hinged external fixator is applied, continuous passive motion (CPM) or active-assisted range of motion (AAROM) may begin within 24 to 48 hours, provided the reduction remains concentric on fluoroscopy.
- Phase II (2-6 Weeks): Transarticular pins are removed in the clinic at the 2-week mark. The patient is transitioned to a hinged elbow brace. Active and active-assisted exercises are initiated under the strict guidance of a specialized physical therapist. A sling is utilized for comfort between exercise sessions.
- Phase III (6+ Weeks): The hinged brace is gradually weaned. Strengthening exercises for the biceps, triceps, and forearm musculature are introduced. Maximum medical improvement may not be reached until 12 to 18 months postoperatively.
Heterotopic Ossification Prophylaxis
Given the extensive surgical dissection and the chronicity of the injury, patients are at an exceptionally high risk of developing postoperative heterotopic ossification (HO).
* Pharmacologic: Indomethacin (75 mg sustained release daily) or Celecoxib for 3 to 6 weeks is routinely prescribed unless contraindicated.
* Radiation: A single dose of localized radiation therapy (700-800 cGy) administered within 72 hours postoperatively may be considered in high-risk patients or those with a history of prior HO.
Conclusion
The open reduction of a chronic elbow dislocation is a demanding procedure that requires a deep understanding of altered pathoanatomy. Through meticulous ulnar nerve management, extensive capsuloligamentous release, triceps lengthening via the Speed V-Y technique, and rigid post-reduction stabilization—whether through temporary pinning, ligamentous reconstruction, or hinged external fixation—surgeons can restore a functional arc of motion to a severely compromised joint. Careful patient selection and rigorous postoperative rehabilitation remain the cornerstones of long-term success.
You Might Also Like