Volar Wedge Bone Grafting and Internal Fixation of Scaphoid Nonunions

Introduction and Epidemiology
The scaphoid is the most frequently fractured carpal bone, representing approximately 60% to 70% of all carpal fractures and up to 15% of all upper extremity fractures. Due to its unique intra-articular position, complex tridimensional geometry, and tenuous retrograde blood supply, scaphoid fractures are notoriously susceptible to delayed union and nonunion. In orthopedic traumatology, a scaphoid fracture that fails to demonstrate both clinical and radiographic evidence of osseous bridging after six months of appropriate management is categorically defined as a nonunion. Epidemiological data indicate that nonunions complicate 5% to 10% of all scaphoid fractures. This incidence rises precipitously in fractures that are unrecognized at the time of injury, inadequately immobilized, or displaced by more than 1 mm.
The typical demographic for a scaphoid nonunion consists of young, active males between the ages of 18 and 35, frequently presenting with a history of a high-energy axial load applied to a hyperextended, ulnarly deviated wrist. However, a significant subset of patients presents insidiously without a distinct, recallable traumatic event. These patients often complain of chronic, vague radial-sided wrist pain, diminished grip strength, and limited range of motion—particularly in extension and radial deviation.
The natural history of an untreated scaphoid nonunion is highly predictable and uniformly detrimental to radiocarpal and midcarpal joint longevity. The biomechanical uncoupling of the proximal and distal carpal rows leads to altered kinematics, specifically driving a dorsal intercalated segment instability (DISI) pattern. Over time, this abnormal articulation results in a predictable, sequential pattern of degenerative arthrosis known as Scaphoid Nonunion Advanced Collapse (SNAC). The progressive stages of SNAC wrist dictate that surgical intervention is paramount to restore carpal kinematics, prevent irreversible joint destruction, and preserve wrist function. Volar wedge bone grafting, combined with rigid internal fixation, remains a cornerstone technique for addressing scaphoid waist nonunions complicated by volar bone loss and the classic "humpback" deformity.
Surgical Anatomy and Biomechanics
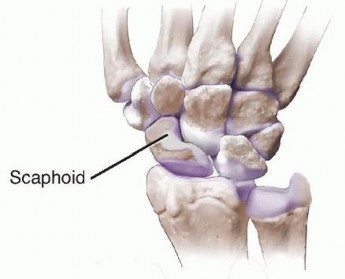
The scaphoid serves as a critical mechanical link between the proximal and distal carpal rows, functioning essentially as an osseous tie-rod that coordinates synchronous carpal motion. It is almost entirely covered by hyaline articular cartilage (accounting for approximately 80% of its total surface area). This extensive cartilaginous envelope severely limits the available surface area for vascular ingress and soft tissue attachment, predisposing the bone to ischemic complications following fracture.
The vascular anatomy of the scaphoid is the primary determinant of its healing capacity and dictates the surgical approach. Seminal microangiographic studies by Gelberman et al. demonstrated that the scaphoid receives its primary blood supply from the dorsal carpal branch of the radial artery. These vessels enter the scaphoid through the dorsal ridge at the level of the waist and provide retrograde blood flow to the proximal pole, supplying 70% to 80% of the bone's volume. A secondary, smaller vascular contribution enters the distal pole volarly via direct branches of the radial artery. Because of this retrograde perfusion, fractures at the waist or proximal pole critically disrupt the intraosseous blood supply to the proximal fragment, significantly elevating the risk of avascular necrosis (AVN) and subsequent nonunion.
Biomechanically, the scaphoid is subjected to immense bending and shear forces during normal wrist motion and physiological loading. When a fracture occurs at the waist, the scaphoid loses its structural integrity and its ability to resist these forces. The distal pole of the scaphoid is pulled into flexion and pronation by the strong radioscaphocapitate (RSC) ligament and the scaphotrapezialtrapezoidal (STT) joint capsule. Conversely, the proximal pole remains attached to the lunate via the intact scapholunate interosseous ligament (SLIL), extending with the lunate. This divergence results in the classic "humpback" deformity—a tridimensional morphological distortion characterized by scaphoid shortening, angular collapse (increased intrascaphoid angle), and a DISI posture of the proximal carpal row.
Failure to correct this 3D deformity during surgical reconstruction results in persistent abnormal carpal kinematics, restricted wrist extension, and an elevated risk of hardware failure and persistent nonunion. Volar wedge grafting specifically addresses the volar cortical defect, restoring the anatomical length, alignment, and load-bearing capacity of the scaphoid.
Indications and Contraindications
Rigorous patient selection is critical for the success of volar wedge bone grafting. The procedure is specifically tailored for nonunions of the scaphoid waist that exhibit a humpback deformity, provided the proximal pole remains adequately vascularized and the surrounding articular cartilage is preserved.
| Clinical Parameter | Operative Indications (Volar Wedge Graft) | Non-Operative or Alternative Indications |
|---|---|---|
| Fracture Displacement | Displacement > 1 mm, angular deformity | Undisplaced fractures (acute setting only) |
| Nonunion Morphology | Scaphoid waist nonunion with volar bone loss / humpback deformity | Asymptomatic nonunion in a low-demand, elderly patient with high surgical risk |
| Carpal Alignment | DISI deformity (Radiolunate angle > 15°, Scapholunate angle > 60°) | Stable, non-progressive alignment in a patient refusing surgery |
| Vascularity | Punctate bleeding present in proximal pole (viable bone) | Avascular necrosis (requires vascularized graft) |
| Arthrosis | Pre-arthrotic or minimal radial styloid beaking (SNAC Stage I) | SNAC Stage II/III (requires salvage procedure) |
Specific Contraindications for Volar Wedge Grafting
- Avascular Necrosis of the Proximal Pole: If preoperative MRI or intraoperative assessment (lack of punctate bleeding/paprika sign) confirms AVN of the proximal pole, non-vascularized grafting has an unacceptably high failure rate. These cases necessitate vascularized bone grafting (e.g., 1,2-Intercompartmental Supraretinacular Artery [1,2-ICSRA] pedicled graft or medial femoral condyle [MFC] free flap).
- Advanced SNAC Wrist (Stages II and III): If degenerative changes have progressed to the midcarpal joint (scaphocapitate or capitolunate articulation), restoring scaphoid anatomy will not relieve pain. Salvage procedures such as proximal row carpectomy (PRC) or scaphoid excision with four-corner arthrodesis are indicated.
- Proximal Pole Nonunions: Fractures located in the proximal third of the scaphoid are technically difficult to access, reduce, and graft via a volar approach due to the overlying radiocarpal ligaments. These are typically managed via a dorsal approach.
- Active Infection: An absolute contraindication to internal fixation and bone grafting.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is essential for the anatomical restoration of the scaphoid and the calculation of required graft dimensions.
Imaging Protocols
Standard posteroanterior (PA), lateral, pronated oblique, and supinated oblique (scaphoid view) radiographs are obtained. The lateral view must be scrutinized to measure the radiolunate and scapholunate angles to quantify the severity of the DISI deformity.
Computed Tomography (CT) is the gold standard for evaluating nonunion architecture, the exact spatial location of the fracture line, and the volumetric degree of bone loss. CT scans must be reformatted along the longitudinal axis of the scaphoid (true sagittal and true coronal planes of the scaphoid). The opposite, uninjured wrist should also be scanned to serve as a volumetric and geometric template for the required bone graft. The height-to-length ratio and the lateral intrascaphoid angle (normal is approximately 24 degrees; >35 degrees indicates significant humpback deformity) are calculated.
Magnetic Resonance Imaging (MRI) without and with gadolinium contrast is utilized to assess the vascularity of the proximal pole. A proximal pole that remains hypointense on T1-weighted images and fails to enhance post-gadolinium suggests avascular necrosis, potentially altering the surgical plan toward a vascularized graft.
Patient Positioning and Setup

The patient is placed in the supine position with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The iliac crest (ipsilateral or contralateral, based on surgeon preference and graft size requirements) is simultaneously prepped and draped for structural bone graft harvesting.
Fluoroscopy is positioned either parallel or perpendicular to the hand table, ensuring unimpeded access for AP, lateral, and oblique intraoperative imaging. The surgeon typically sits on the axillary side of the arm, with the assistant opposite. Intravenous prophylactic antibiotics are administered prior to tourniquet inflation (typically inflated to 250 mmHg).
Detailed Surgical Approach and Technique
The surgical objective is to radically debride the nonunion, correct the humpback deformity, insert a structural cortico-cancellous wedge graft to restore volar length, and achieve rigid internal fixation.
The Volar Approach

A modified Russe volar approach is utilized. A longitudinal or slightly curvilinear incision is made directly over the flexor carpi radialis (FCR) tendon, extending from the level of the radial styloid proximally for approximately 4 to 5 cm. This approach provides excellent exposure to the volar aspect of the scaphoid waist and distal pole.
Superficial Dissection and Internervous Plane
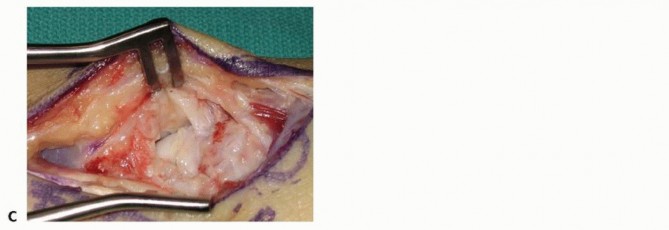
The superficial fascia is incised, and the FCR tendon sheath is opened. The FCR tendon is retracted ulnarly. The internervous plane lies between the FCR (innervated by the median nerve) and the radial artery. Extreme care must be taken to identify and protect the palmar cutaneous branch of the median nerve (PCBMN), which lies ulnar to the FCR, and the radial artery, which is situated radially. The floor of the FCR sheath is incised longitudinally to expose the volar wrist capsule.
Capsulotomy and Joint Exposure

A radiocarpal capsulotomy is performed. Various capsulotomy techniques exist (e.g., longitudinal, T-shaped, or ligament-sparing). It is critical to incise the capsule in a manner that allows for subsequent robust repair, as the volar extrinsic ligaments (specifically the radioscaphocapitate and long radiolunate ligaments) are vital for carpal stability. The capsule is elevated as full-thickness flaps to expose the underlying scaphoid nonunion. Retractors (such as Senn or small Ragnell retractors) are carefully placed to maintain exposure without damaging the delicate articular surfaces.
Debridement of the Nonunion

The nonunion site is identified. It is often filled with dense fibrous tissue, sclerotic bone, and occasionally a pseudarthrosis fluid cavity. Using sharp curettes, a high-speed burr, and rongeurs, all fibrous tissue and necrotic bone are meticulously debrided back to healthy, bleeding cancellous bone (the "paprika sign"). The sclerotic margins of both the proximal and distal fragments must be resected to expose a bleeding osseous bed. Intraoperative assessment of proximal pole vascularity is performed at this stage; the presence of punctate bleeding confirms viability and supports the use of a non-vascularized graft.
Deformity Correction

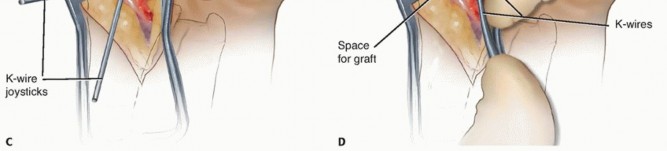
To correct the humpback deformity, 0.045-inch or 0.062-inch Kirschner wires (K-wires) are inserted into the proximal and distal scaphoid fragments to serve as joysticks. By extending the wrist over a rolled towel and manipulating the joysticks (extending the distal fragment and flexing the proximal fragment), the DISI deformity is corrected, and the volar defect is opened. This maneuver restores the anatomical length and intrascaphoid angle. The size of the resulting volar defect is measured precisely using a caliper to template the required bone graft.
Bone Graft Harvest

While local distal radius bone graft can be used for small defects, a structural cortico-cancellous graft from the anterior iliac crest is the gold standard for correcting significant humpback deformities. A small incision is made over the anterior superior iliac spine (ASIS). Dissection is carried down to the outer table of the ilium. A wedge of cortico-cancellous bone, slightly larger than the templated defect, is harvested using osteotomes or an oscillating saw. Hemostasis is achieved at the donor site, and it is closed in layers.
Graft Contouring and Insertion

On the back table, the iliac crest graft is meticulously contoured using a rongeur or high-speed burr to match the specific dimensions of the volar scaphoid defect. The cortical portion of the graft is oriented volarly to provide structural support against the compressive forces of flexion, while the cancellous portion is directed dorsally to integrate with the host cancellous bone. The graft is press-fit into the defect while maintaining the correction with the K-wire joysticks. Fluoroscopy is used to confirm the restoration of scaphoid anatomy and carpal alignment.
Internal Fixation

Rigid internal fixation is paramount. A headless compression screw is the implant of choice. For a volar approach, retrograde screw insertion (from distal to proximal) is utilized. The starting point is at the distal scaphoid tubercle, ensuring the trajectory is down the central axis of the scaphoid. Placing the screw down the central third of the scaphoid has been biomechanically proven to provide the highest stiffness and load to failure. A guidewire is advanced from the distal pole, through the graft, and into the subchondral bone of the proximal pole.
Fluoroscopy in multiple planes confirms central wire placement. The length is measured, and the bone is drilled over the wire. The headless compression screw is then inserted, ensuring the trailing threads are completely buried beneath the articular cartilage of the distal pole to prevent impingement on the trapezium. The differential pitch of the screw provides interfragmentary compression across the nonunion site and the graft.
Final Verification and Closure

Final fluoroscopic images are obtained in all planes to verify hardware placement, fracture reduction, and restoration of the intrascaphoid angle. The joysticks are removed. The wrist is taken through a full range of motion under fluoroscopy to ensure stability and the absence of hardware impingement. The volar capsule is meticulously repaired using non-absorbable sutures to restore the integrity of the extrinsic volar ligaments. The FCR sheath is left open to prevent postoperative stenosis, and the skin is closed with subcutaneous and subcuticular sutures.
Complications and Management
Despite meticulous surgical technique, scaphoid nonunion surgery carries inherent risks. Recognizing and managing these complications is crucial for optimizing patient outcomes and preventing end-stage carpal collapse.
| Complication | Incidence | Etiology | Management / Salvage Strategy |
|---|---|---|---|
| Persistent Nonunion | 10% - 20% | Inadequate debridement, unrecognized AVN, loss of fixation, smoking | Revision grafting (consider vascularized graft), prolonged immobilization, or salvage procedure if arthrosis develops. |
| Hardware Prominence | 5% - 10% | Incomplete seating of headless screw, screw back-out, or incorrect length selection | Screw removal once union is achieved; immediate revision if causing acute articular damage to STT or radioscaphoid joints. |
| Avascular Necrosis | Variable | Progressive ischemia of the proximal pole despite grafting | Vascularized bone grafting (1,2-ICSRA or Medial Femoral Condyle). If collapsed, proceed to PRC or Four-Corner Fusion. |
| SNAC Progression | 5% - 15% | Failure to correct humpback deformity (persistent DISI) leading to altered kinematics | Stage-dependent salvage: Radial styloidectomy, Proximal Row Carpectomy (PRC), or Scaphoid excision with Four-Corner Arthrodesis. |
| Infection | < 2% | Surgical site contamination, compromised soft tissue envelope | Superficial: Oral antibiotics. Deep: Operative irrigation and debridement, hardware removal if unstable, IV antibiotics. |
| Donor Site Morbidity | 10% - 15% | Lateral femoral cutaneous nerve injury, hematoma, chronic pain at iliac crest | Careful dissection at ASIS, local anesthetic infiltration, hematoma evacuation if symptomatic. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation must delicately balance the need for rigid immobilization to facilitate bony union with the desire to prevent profound wrist stiffness and complex regional pain syndrome (CRPS).
Phase I: Immobilization (Weeks 0 to 6)
Immediately postoperatively, the patient is placed in a bulky dressing and a well-molded short-arm thumb spica splint. At the first postoperative visit (10 to 14 days), sutures are removed, and the patient is transitioned to a short-arm thumb spica cast. Finger, elbow, and shoulder range of motion exercises are initiated immediately to prevent proximal and distal stiffness and to promote venous return.
Phase II: Clinical and Radiographic Assessment (Weeks 6 to 12)
At 6 to 8 weeks, the cast is removed, and clinical evaluation is performed. Absence of tenderness in the anatomic snuffbox and over the scaphoid tubercle is a positive clinical sign of progressing union. Plain radiographs are obtained to assess for early bridging trabeculae. Because plain films can be misleading due to the presence of the dense cortical graft and metallic hardware, a fine-cut CT scan reformatted along the longitudinal axis of the scaphoid is highly recommended at 8 to 12 weeks to definitively confirm osseous integration of the graft before allowing return to heavy loading.
Phase III: Mobilization and Strengthening (Weeks 12+)
Once CT confirms union, the patient is transitioned to a removable splint and begins aggressive active and active-assisted range of motion under the guidance of a certified hand therapist. Strengthening exercises are gradually introduced. Return to contact sports or heavy manual labor is typically restricted until 4 to 6 months postoperatively, contingent upon full radiographic union and restoration of functional grip strength.
Summary of Key Guidelines
- Definition: Scaphoid nonunion is defined as a lack of clinical and radiographic healing at 6 months post-injury.
- Deformity: The classic "humpback" deformity consists of volar bone loss, scaphoid shortening, and a DISI posture of the proximal carpal row.
- Vascularity: The proximal pole is highly susceptible to AVN due to the retrograde intraosseous blood supply from the dorsal carpal branch of the radial artery.
- Surgical Goal: Volar wedge grafting aims to restore scaphoid length, correct the intrascaphoid angle, and provide a biologic scaffold for union.
- Fixation: Central axis placement of a headless compression screw provides the optimal biomechanical construct for union.
- Contraindications: Volar non-vascularized grafting is contraindicated in the presence of proximal pole AVN (requires vascularized graft) or midcarpal arthrosis (requires salvage procedure).
You Might Also Like


