Volar Wedge Bone Grafting and Internal Fixation of Scaphoid Nonunions

Introduction and Epidemiology
Scaphoid fractures represent the most frequently encountered carpal fractures in clinical orthopedic practice, accounting for approximately 60% to 70% of all carpal bone injuries. While the majority of acute, non-displaced scaphoid fractures achieve osseous union with appropriate cast immobilization or early percutaneous surgical intervention, a distinct and challenging subset fails to heal. A scaphoid nonunion is strictly defined as a fracture that has failed to demonstrate clinical or radiographic evidence of healing six months following the initial injury. Epidemiological data suggest that nonunions complicate 5% to 10% of all scaphoid fractures. This incidence increases precipitously in the presence of delayed initial presentation, fractures involving the proximal pole, or initial fracture displacement exceeding 1 millimeter.
The typical demographic profile for a scaphoid nonunion involves young, active male patients between the ages of 18 and 35 years. Frequently, the initial high-energy trauma or hyperextension injury is dismissed by the patient as a simple wrist sprain, leading to a critical delay in diagnosis and therapeutic intervention. Unrecognized injuries sustained during adolescence may present indolently, only becoming clinically apparent when the patient reaches middle age and begins to experience the early mechanical symptoms of progressive carpal derangement.
The natural history of an untreated scaphoid nonunion is characterized by a predictable, progressive pattern of degenerative radiocarpal and midcarpal arthrosis, universally recognized as Scaphoid Nonunion Advanced Collapse (SNAC). The altered kinematics of the uncoupled scaphoid lead to abnormal force transmission across the radioscaphoid and capitolunate articulations. Long-term outcome studies demonstrate that the incidence of symptomatic, function-limiting wrist pathology is profoundly higher in patients with untreated scaphoid nonunions. Consequently, surgical intervention is strongly indicated to restore carpal anatomy, achieve osseous union, and halt the progression of degenerative changes. Volar wedge bone grafting combined with rigid internal fixation remains the gold standard for treating scaphoid waist nonunions associated with a humpback deformity and viable fracture fragments.
Surgical Anatomy and Biomechanics
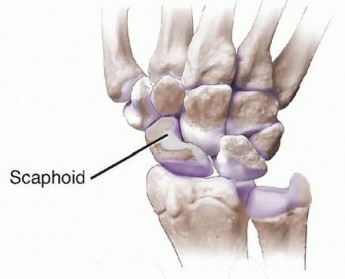
A profound understanding of scaphoid osteology, vascularity, and carpal kinematics is paramount for successful surgical reconstruction. The scaphoid serves as a critical mechanical link—a "tie-rod"—bridging the proximal and distal carpal rows. Its complex, three-dimensional, boat-like geometry makes anatomical reduction and stable internal fixation technically demanding. Furthermore, approximately 80% of the scaphoid surface is covered by hyaline articular cartilage, severely limiting the available non-articular surface area for surgical approach, vascular ingress, and hardware implantation.
Vascular Anatomy and Ischemic Risk
The tenuous blood supply of the scaphoid dictates its propensity for delayed union, nonunion, and avascular necrosis (AVN). The primary arterial supply is derived from the radial artery. Gelberman’s seminal microangiographic studies demonstrated that the dorsal carpal branch of the radial artery enters the scaphoid through the dorsal ridge and supplies the proximal 70% to 80% of the bone via an intraosseous retrograde flow network. A smaller volar branch enters the distal tubercle, supplying the distal 20% to 30% of the bone. Because the proximal pole relies entirely on this retrograde perfusion, fractures occurring at the waist or proximal pole critically disrupt the intraosseous network, rendering the proximal fragment ischemic and highly susceptible to AVN.
Carpal Kinematics and the Humpback Deformity
Biomechanically, the scaphoid is subjected to significant shear and bending forces during normal wrist motion. In the setting of a scaphoid waist fracture, the mechanical linkage between the proximal and distal carpal rows is lost. The distal scaphoid fragment tends to flex volarly under the pull of the radioscaphocapitate (RSC) ligament and the functional demands of the thumb trapezium and trapezoid. Conversely, the proximal fragment extends with the lunate due to the intact scapholunate interosseous ligament, resulting in a Dorsal Intercalated Segment Instability (DISI) posture.
Over time, volar bone resorption at the fracture site combined with this flexed posture leads to the classic "humpback" deformity. This deformity alters the intrascaphoid angle (normally 35 to 45 degrees) and decreases the overall scaphoid length. Failure to correct this humpback deformity during surgical reconstruction results in persistent carpal malalignment, restricted wrist extension, and an elevated risk of hardware failure or persistent nonunion. The volar wedge bone grafting technique specifically addresses this biomechanical derangement by inserting a structural corticocancellous graft into the volar defect, thereby restoring normal scaphoid length, correcting the DISI deformity, and re-establishing the normal intrascaphoid angle.
Indications and Contraindications
Patient selection is critical for the success of volar wedge bone grafting. The procedure is specifically tailored for scaphoid nonunions with an associated humpback deformity where the proximal pole retains adequate vascularity.
| Clinical Scenario | Management Strategy | Rationale |
|---|---|---|
| Acute Non-Displaced Waist Fracture | Non-Operative | High union rate with appropriate cast immobilization. |
| Symptomatic Waist Nonunion without Deformity | Operative In Situ Fixation with Graft | No structural correction needed; cancellous graft and compression screw suffice. |
| Symptomatic Waist Nonunion with Humpback Deformity | Operative Volar Wedge Grafting | Structural corticocancellous wedge required to restore scaphoid length and correct DISI. |
| Proximal Pole Nonunion with AVN | Operative Vascularized Bone Graft | Structural non-vascularized grafts have high failure rates in the setting of ischemia. |
| SNAC Stage II or III | Salvage Procedures | Joint preservation is no longer viable; requires proximal row carpectomy or partial wrist fusion. |
Operative Indications
Surgical intervention with a volar structural wedge graft is indicated in the presence of a symptomatic scaphoid waist nonunion characterized by volar bone loss and a humpback deformity. Radiographic parameters dictating the need for a structural wedge include an intrascaphoid angle greater than 45 degrees or a lateral intrascaphoid angle greater than 35 degrees. Crucially, the patient must possess a viable proximal pole, as evidenced by preoperative magnetic resonance imaging (MRI) or intraoperative punctate bleeding.
Contraindications
Absolute contraindications to non-vascularized volar wedge grafting include active local or systemic infection, advanced radiocarpal or midcarpal arthrosis (SNAC Stage II or III), and severe avascular necrosis of the proximal pole without structural integrity. In cases of profound proximal pole AVN, a vascularized bone graft (such as the 1,2 Intercompartmental Supraretinacular Artery pedicled graft or a free medial femoral condyle graft) is the preferred alternative. Relative contraindications include heavy tobacco use (which exponentially increases nonunion rates), uncontrolled diabetes mellitus, and patient inability to comply with strict postoperative immobilization protocols.
Pre Operative Planning and Patient Positioning
Comprehensive preoperative evaluation begins with a meticulous clinical examination. Patients typically exhibit localized tenderness over the anatomic snuffbox and the volar scaphoid tubercle. Wrist range of motion, particularly extension, is often restricted compared to the contralateral side. Provocative maneuvers, such as loaded wrist extension or the scaphoid shift test (Watson test), frequently elicit localized radial-sided pain and apprehension.
Radiographic Evaluation
Standard radiographic evaluation must include a posteroanterior (PA) view, a true lateral view, a PA view in ulnar deviation (scaphoid view), and a semi-pronated oblique view. These baseline radiographs help identify the nonunion, assess the degree of carpal collapse (DISI deformity), and rule out advanced arthritic changes indicative of a SNAC wrist.

Advanced Imaging Modalities
A computed tomography (CT) scan is mandatory for meticulous preoperative planning. Scans must be reformatted along the true longitudinal axis of the scaphoid to accurately quantify the volume of bone loss, the degree of the humpback deformity, and the precise location of the nonunion. Magnetic resonance imaging (MRI) without and with gadolinium contrast is highly recommended to assess the vascular status of the proximal pole. Lack of contrast enhancement in the proximal fragment on T1-weighted fat-suppressed images suggests avascular necrosis, which should prompt the surgeon to alter the surgical plan toward a vascularized bone graft.
Patient Positioning and Anesthesia
The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block) or general anesthesia, depending on patient and surgeon preference. The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. The fluoroscopy unit (C-arm) is positioned parallel to the hand table, entering from the distal or contralateral side, allowing for unimpeded orthogonal imaging of the wrist throughout the procedure. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The surgical execution of volar wedge bone grafting requires meticulous soft tissue handling, precise correction of carpal deformity, and rigid internal fixation. The classic Russe approach is utilized to access the volar aspect of the scaphoid, providing excellent exposure while preserving the critical dorsal blood supply.
Superficial Dissection and Exposure
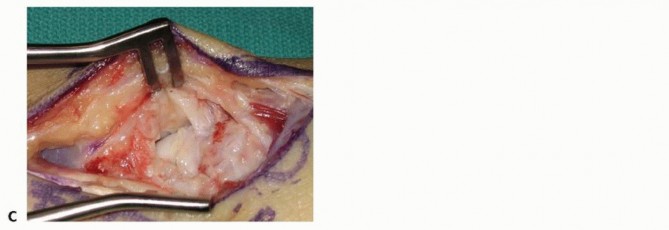
A longitudinal or slightly curvilinear incision is made over the volar radial aspect of the wrist, centered over the flexor carpi radialis (FCR) tendon. The incision extends from the distal scaphoid tubercle proximally for approximately 4 to 5 centimeters.

Subcutaneous tissues are bluntly dissected to protect branches of the superficial radial nerve and the palmar cutaneous branch of the median nerve. The FCR tendon sheath is identified and incised longitudinally. The FCR tendon is retracted ulnarly, protecting the median nerve, while the radial artery is carefully identified and retracted radially. This internervous plane provides safe and direct access to the volar wrist capsule.
Deep Dissection and Capsulotomy
The deep volar radiocarpal ligaments, specifically the radioscaphocapitate (RSC) and radiolunotriquetral (RLT) ligaments, are identified. A longitudinal or T-shaped capsulotomy is performed, taking care to preserve the integrity of the RSC ligament to allow for robust repair during closure, which is critical for preventing postoperative carpal instability.

Upon reflecting the capsule, the scaphoid nonunion site is exposed. The nonunion is often obscured by fibrous scar tissue and hypertrophic synovial proliferation, which must be meticulously excised to visualize the bony anatomy.
Preparation of the Nonunion Site
The nonunion interface is debrided using sharp curettes and a high-speed motorized burr under continuous saline irrigation to prevent thermal necrosis. All fibrous tissue, sclerotic bone, and necrotic debris must be removed until healthy, bleeding cancellous bone is encountered on both the proximal and distal fragments.

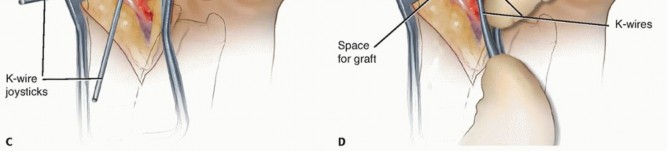
The viability of the proximal pole is assessed by releasing the tourniquet briefly to observe punctate bleeding (the "paprika sign"). Once the nonunion is fully debrided, the humpback deformity is corrected. This is achieved by extending the wrist and applying gentle traction, which opens the volar aspect of the fracture site, creating a trapezoidal or wedge-shaped defect. A lamina spreader or fine distractors can be carefully utilized to maintain the corrected alignment and restore the intrascaphoid angle.
Bone Graft Harvest
To bridge the structural defect and restore scaphoid anatomy, a corticocancellous bone graft is required. The ipsilateral anterior iliac crest is the preferred donor site due to its robust structural integrity and rich osteogenic potential. Alternatively, a graft may be harvested from the distal radius, though this may lack the necessary structural rigidity for large humpback deformities.

The iliac crest is exposed via a small incision posterior to the anterior superior iliac spine (ASIS). A block of corticocancellous bone is harvested using osteotomes or an oscillating saw, ensuring the cortical strut is maintained intact. Hemostasis is achieved at the donor site utilizing bone wax or topical hemostatic agents, and the wound is closed in layers.
Graft Preparation and Insertion
The harvested bone graft is meticulously contoured on the back table to match the precise dimensions of the volar scaphoid defect. The graft is shaped into a wedge, with the cortical surface intended to sit flush with the volar cortex of the scaphoid, providing structural support to prevent recurrent collapse.

The shaped corticocancellous wedge is press-fit into the distraction gap of the scaphoid. The cortical face of the graft must be positioned volarly to act as a buttress, maintaining the corrected intrascaphoid angle and restoring the overall length of the scaphoid.

Provisional Fixation
Once the graft is seated and the carpal alignment is deemed satisfactory under orthogonal fluoroscopy, provisional fixation is achieved using multiple 0.045-inch or 0.062-inch Kirschner wires (K-wires). These wires are driven from the distal scaphoid pole, across the graft, and into the proximal pole. Care must be taken to place the K-wires peripherally to avoid obstructing the central trajectory required for the definitive compression screw.
Definitive Internal Fixation
Rigid internal fixation is paramount for promoting primary bone healing and graft incorporation. A headless compression screw (e.g., Acutrak, Herbert, or similar systems) is the implant of choice. For a volar approach, the screw is typically inserted in a retrograde fashion (from distal to proximal).
A central guide wire is inserted down the true longitudinal axis of the scaphoid, aiming for the apex of the proximal pole. The position and length of the guide wire are verified on multiple fluoroscopic views to ensure it does not breach the radiocarpal joint.

The appropriate screw length is measured, typically subtracting 2 to 4 millimeters to ensure the screw is countersunk beneath the articular cartilage at both poles. The scaphoid is drilled over the guide wire, and the headless compression screw is inserted. As the screw advances, its variable pitch design compresses the distal fragment, the interposed wedge graft, and the proximal fragment into a single rigid construct.

Following screw insertion, the provisional K-wires are removed. Final fluoroscopic images are obtained through full wrist range of motion to confirm stable fixation, anatomical restoration of the scaphoid, and the absolute absence of hardware protrusion into the radiocarpal or midcarpal joints. The volar capsule and RSC ligament are meticulously repaired, and the wound is closed in a standard fashion.
Complications and Management
Despite meticulous surgical technique, volar wedge bone grafting of scaphoid nonunions carries inherent risks. Anticipation and prompt management of complications are essential for optimizing patient outcomes.
| Complication | Estimated Incidence | Management and Salvage Strategies |
|---|---|---|
| Persistent Nonunion | 10% - 20% | Assess vascularity via MRI/CT. If proximal pole is viable, consider revision grafting with robust fixation. If AVN is present, utilize a vascularized bone graft. |
| Hardware Prominence | 5% - 10% | Leads to rapid chondral damage. Requires prompt surgical removal or exchange of the prominent screw. |
| Progression to SNAC Wrist | Variable | If symptomatic arthrosis develops despite union, salvage procedures (Four-corner fusion, Proximal Row Carpectomy) are indicated. |
| Donor Site Morbidity (ICBG) | 15% - 25% | Hematoma, lateral femoral cutaneous nerve neuropraxia, or chronic pain. Managed with analgesics, local blocks, and time. |
| Complex Regional Pain Syndrome | 2% - 5% | Early recognition is critical. Aggressive hand therapy, neuropathic pain modulators (Gabapentin/Pregabalin), and sympathetic blocks. |
Persistent nonunion remains the most frustrating complication. It is often multifactorial, stemming from inadequate debridement of sclerotic bone, failure to recognize proximal pole ischemia, insufficient graft structural integrity, or suboptimal screw placement resulting in poor interfragmentary compression. If a nonunion persists at six months postoperatively, a thorough reassessment with fine-cut CT and contrast-enhanced MRI is warranted. Revision surgery using a vascularized bone graft from the distal radius (1,2 ICSRA) or a free medial femoral condyle graft should be strongly considered.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must carefully balance the need for rigid immobilization to promote osseous healing with the desire to prevent debilitating wrist and hand stiffness.
Immediately postoperatively, the patient is placed in a bulky dressing reinforced with a volar thumb spica splint. The arm is elevated to minimize edema, and immediate active range of motion of the fingers, elbow, and shoulder is encouraged to facilitate venous return and prevent tendon adhesions.
At two weeks postoperatively, the surgical dressing is removed, and the incision is inspected for healing. Sutures are removed, and the patient is transitioned into a custom-molded short arm thumb spica cast or a rigid thermoplastic splint. The duration of immobilization is highly dependent on radiographic evidence of healing.
Clinical follow-up with serial radiographs is typically performed at 6, 12, and 16 weeks.
Because plain radiographs can be notoriously unreliable for confirming scaphoid union, a fine-cut CT scan reformatted along the longitudinal axis of the scaphoid is highly recommended at the 8 to 12-week mark. Once bridging trabecular bone is confirmed across greater than 50% of the cross-sectional area at both the proximal and distal graft interfaces, the cast is discontinued. The patient is then referred to a specialized hand therapist to initiate a progressive range of motion and strengthening protocol. Return to heavy manual labor or contact sports is generally restricted until at least 4 to 6 months postoperatively, contingent upon full radiographic consolidation and functional recovery.
Summary of Key Literature and Guidelines
The evolution of surgical management for scaphoid nonunions is deeply rooted in landmark orthopedic literature. The fundamental concept of utilizing a volar structural graft to correct the humpback deformity was pioneered by Fisk in the 1980s and subsequently refined by Fernandez. The Fisk-Fernandez technique established the biomechanical necessity of restoring the volar cortical length to correct the associated DISI deformity and unload the radiocarpal joint, thereby mitigating the progression of SNAC arthropathy.
The volar surgical approach to the scaphoid, utilizing the internervous plane between the FCR and the radial artery, was popularized by Russe. The Russe approach remains the standard for addressing waist and distal pole nonunions, providing excellent exposure for debridement and grafting while preserving the critical dorsal blood supply to the proximal pole.
The advent of headless compression screws revolutionized the internal fixation of scaphoid fractures and nonunions. Studies by Herbert and Fisher demonstrated the superiority of rigid internal compression over K-wire fixation, leading to significantly higher union rates and allowing for earlier mobilization. More recent biomechanical and clinical studies by Slade and Dodds have further optimized screw trajectory and design, emphasizing the importance of central screw placement along the longitudinal axis of the scaphoid to maximize biomechanical stability and interfragmentary compression.
Current clinical guidelines strongly support the use of non-vascularized structural corticocancellous bone grafting (volar wedge) combined with headless compression screw fixation for scaphoid waist nonunions with a humpback deformity, provided the proximal pole remains adequately vascularized. Under these precise indications, contemporary literature reports union rates ranging from 80% to 90%, with significant improvements in patient-reported outcome measures and long-term preservation of carpal kinematics.
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
You Might Also Like
