Lateral Clavicular Fractures: Comprehensive Surgical Management
Key Takeaway
Lateral clavicular fractures present unique biomechanical challenges due to the deforming forces of the trapezius and the disruption of the coracoclavicular ligaments. This guide details the Neer classification system, evaluating stable versus unstable fracture patterns. It provides a comprehensive overview of operative strategies, including hook-plate fixation and coracoclavicular ligament reconstruction, ensuring orthopedic surgeons can achieve secure fixation, high union rates, and optimal functional recovery.
INTRODUCTION TO LATERAL CLAVICULAR FRACTURES
Lateral clavicular fractures account for approximately 15% to 20% of all clavicle fractures. Unlike midshaft fractures, which generally enjoy high rates of union with conservative management, fractures of the lateral third present a unique biomechanical challenge. The inherent instability of specific fracture patterns in this region is driven by the disruptive interplay between the weight of the upper extremity and the unopposed pull of the trapezius muscle.
Historically, the treatment of displaced lateral clavicular fractures has been highly controversial. While nonoperative management can yield acceptable functional results in certain patient populations, it is historically associated with nonunion rates approaching 30% to 45% in displaced patterns. Consequently, modern orthopedic practice leans heavily toward operative intervention for displaced fractures to restore the suspensory mechanism of the shoulder girdle, mitigate the risk of nonunion, and optimize functional recovery.
This comprehensive guide delineates the pathoanatomy, classification, and evidence-based surgical management of lateral clavicular fractures, providing orthopedic surgeons with the technical nuances required to achieve secure fixation in the lateral segment.
ANATOMY AND BIOMECHANICS
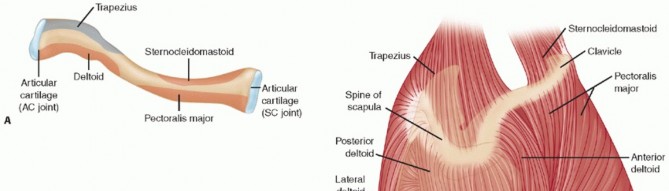
A profound understanding of the coracoclavicular (CC) ligamentous complex is paramount when evaluating and treating lateral clavicular fractures. The CC complex is the primary suspensory mechanism of the upper extremity, tethering the clavicle to the scapula via the coracoid process.
- The Conoid Ligament: Positioned medially and posteriorly, the conoid ligament is a cone-shaped structure that primarily resists superior translation of the clavicle relative to the scapula.
- The Trapezoid Ligament: Positioned laterally and anteriorly, the trapezoid ligament is broad and primarily resists axial compression toward the acromioclavicular (AC) joint.
Deforming Forces
In unstable lateral clavicular fractures, the fracture line occurs medial to the intact CC ligaments. This anatomical disruption unleashes two primary deforming forces:
1. Proximal Fragment Displacement: The trapezius muscle, inserting on the superior aspect of the lateral clavicle, acts as a powerful deforming force, pulling the proximal fracture segment superiorly and posteriorly.
2. Distal Fragment Displacement: The distal segment, remaining attached to the scapula via the intact CC ligaments and the AC joint capsule, is pulled inferiorly and medially by the weight of the arm and the pull of the pectoralis major and latissimus dorsi.
Clinical Pearl: The degree of displacement in a lateral clavicle fracture is a direct radiographic surrogate for the integrity of the coracoclavicular ligaments. Significant superior migration of the medial fragment definitively indicates CC ligament disruption or detachment.
NEER CLASSIFICATION OF LATERAL CLAVICULAR FRACTURES
Charles Neer originally described a classification system based on the relationship of the fracture line to the coracoclavicular ligaments, which dictates the inherent stability of the injury. This system remains the gold standard for guiding treatment decisions.
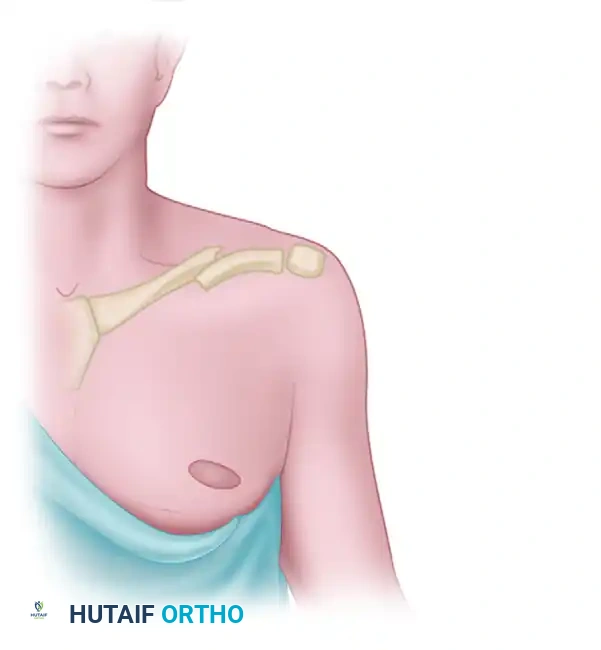
Type I: Stable, Ligaments Intact
Type I fractures occur lateral to the coracoclavicular ligaments. The conoid and trapezoid ligaments remain entirely intact and attached to the medial fragment. Because the suspensory mechanism is undisturbed, these fractures are inherently stable and exhibit minimal displacement.
Figure 1: Neer Type I Lateral Clavicular Fracture. Intact ligaments hold the fragments securely in place.
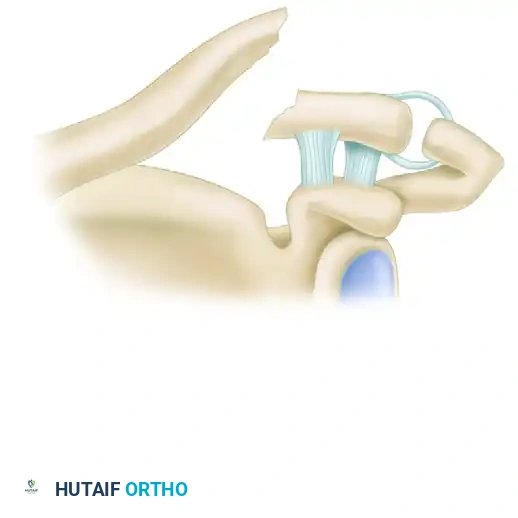
Type II: Unstable, Ligaments Detached from Medial Segment
Type II fractures are characterized by a fracture line that occurs just medial to the coracoclavicular ligaments. The proximal segment loses its ligamentous tether, allowing the trapezius to displace it superiorly. Type II is subdivided based on the specific status of the CC ligaments:
Type IIa: Both the conoid and trapezoid ligaments remain attached to the distal segment. The proximal segment, devoid of any ligamentous attachments, is significantly displaced superiorly.

Figure 2: Neer Type IIa Lateral Clavicular Fracture. Conoid and trapezoid ligaments are on the distal segment; the proximal segment is displaced.
Type IIb: The conoid ligament is ruptured, while the trapezoid ligament remains attached to the distal segment. The proximal fragment is displaced superiorly due to the loss of the conoid's restraint against superior translation.
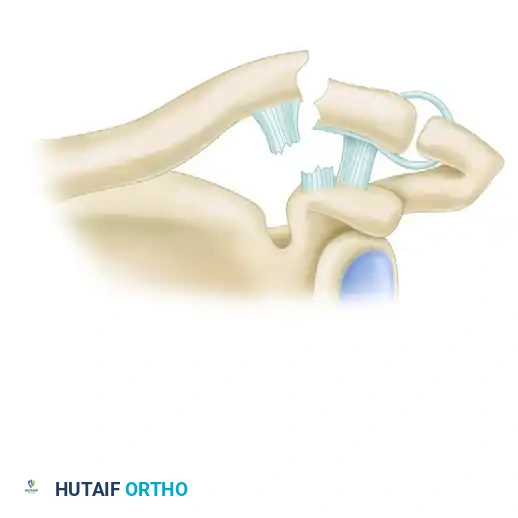
Figure 3: Neer Type IIb Lateral Clavicular Fracture. The conoid ligament is ruptured, and the trapezoid ligament remains attached to the distal segment.
Type III: Intra-articular
Type III fractures involve an intra-articular extension into the acromioclavicular (AC) joint. While the CC ligaments are typically intact (rendering the fracture relatively stable), the primary clinical concern is the subsequent development of post-traumatic AC joint arthrosis.
Expanded Classification (Types IV and V)
Later modifications to the Neer classification (often attributed to Craig) added two additional types:
* Type IV: Occurs in children and adolescents. It represents a physeal separation where the distal clavicle displaces superiorly through a tear in the thick periosteal sleeve, while the CC ligaments remain attached to the periosteum.
* Type V: A comminuted fracture pattern where an inferior cortical fragment remains attached to the intact CC ligaments, while the main proximal and distal fragments are displaced.
INDICATIONS FOR SURGERY
Treatment of lateral clavicular fractures remains controversial, though consensus is building around operative intervention for specific patterns. Good results have been reported with both operative and nonoperative treatment, even in the presence of malunions. However, the high rate of symptomatic nonunion in displaced fractures drives surgical decision-making.
Nonoperative Management:
* Indicated for Neer Type I and Type III fractures.
* Indicated for non-ambulatory patients or those with severe medical comorbidities precluding surgery.
* Protocol involves a brief period of sling immobilization for comfort, followed by early progressive range of motion.
Operative Management:
* Indicated for Neer Type II (IIa and IIb) and Type V fractures with >100% displacement.
* Open fractures or fractures with impending skin compromise (skin tenting).
* Polytrauma patients requiring early upper extremity weight-bearing.
* Floating shoulder injuries (ipsilateral scapular neck and clavicle fractures).
SURGICAL POSITIONING AND APPROACH
Patient Positioning
The patient is typically placed in the beach chair position with the head secured in a neutral position. This setup allows the weight of the arm to assist in reducing the superiorly displaced proximal fragment. Alternatively, a supine position with a bump between the scapulae can be utilized, though it may make intraoperative fluoroscopy of the AC joint more cumbersome.
The entire forequarter, including the base of the neck, shoulder, and arm down to the wrist, should be prepped and draped free to allow for dynamic manipulation of the upper extremity during reduction.
Surgical Approach
- Incision: A superior approach is utilized. The incision is made either directly over the clavicle or slightly anterior to it (saber incision), extending from the mid-clavicle to the lateral edge of the acromion.
- Dissection: Subcutaneous tissues are divided. The supraclavicular nerves should be identified and protected to prevent postoperative anterior chest wall numbness or painful neuromas.
- Fascial Incision: The deltotrapezial fascia is incised longitudinally over the superior aspect of the clavicle. Full-thickness subperiosteal flaps are elevated to expose the fracture site.
- Joint Exposure: If an intra-articular fracture is present or a hook plate is planned, the AC joint capsule is carefully exposed.
Surgical Warning: Meticulous preservation of the soft tissue envelope and periosteum is critical. Over-stripping the lateral fragment, which is already small and poorly vascularized, significantly increases the risk of nonunion and avascular necrosis.
OPERATIVE FIXATION STRATEGIES
The primary surgical challenge in lateral clavicular fractures is obtaining secure fixation in the small, often comminuted, distal segment. Several strategies have been developed to address this biomechanical hurdle.
1. Subacromial Hook-Plate Fixation
The subacromial hook plate is a highly effective implant designed specifically for lateral clavicle fractures and AC joint dislocations. The plate is fixed to the superior aspect of the proximal clavicle, while a specialized hook extends under the acromion, posterior to the AC joint.
- Biomechanics: The hook acts as a lever under the acromion, effectively reducing the proximal clavicle and neutralizing the superior deforming force of the trapezius. It does not rely on screw purchase in the small distal fragment.
- Outcomes: High rates of union (95% or higher) and excellent shoulder function have been reported with the use of hook-plates.
- Pitfalls: The primary drawback is patient discomfort and the risk of acromial osteolysis or subacromial impingement. Because the hook alters the kinematics of the AC joint, plate removal is generally required as soon as clinical and radiographic union occurs (typically at 3 to 5 months postoperatively).
2. Superior Precontoured Locking Plates
Advancements in locking plate technology have popularized the use of anatomically precontoured distal clavicle locking plates. These plates feature a cluster of small-diameter locking screws (e.g., 2.4 mm or 2.7 mm) at the lateral end, allowing for multiple points of fixation in the small distal fragment.
- Technique: The fracture is reduced and provisionally held with K-wires. The plate is applied superiorly. At least three, and preferably four to six, locking screws are placed into the distal fragment.
- Advantages: Avoids the need for routine hardware removal associated with hook plates. Preserves AC joint kinematics.
- Limitations: May not provide sufficient stability if the distal fragment is severely comminuted or osteoporotic. In such cases, plating over to the acromion to gain greater fixation (spanning the AC joint) may be necessary, though this also requires subsequent hardware removal.
3. Supplemental Coracoclavicular (CC) Fixation
Because the fundamental pathology of a Type II fracture involves the loss of CC ligamentous restraint, supplementing plate fixation with a CC reconstruction is a highly effective strategy. This can be achieved using heavy nonabsorbable sutures or cortical button devices passed from the clavicle to the coracoid.
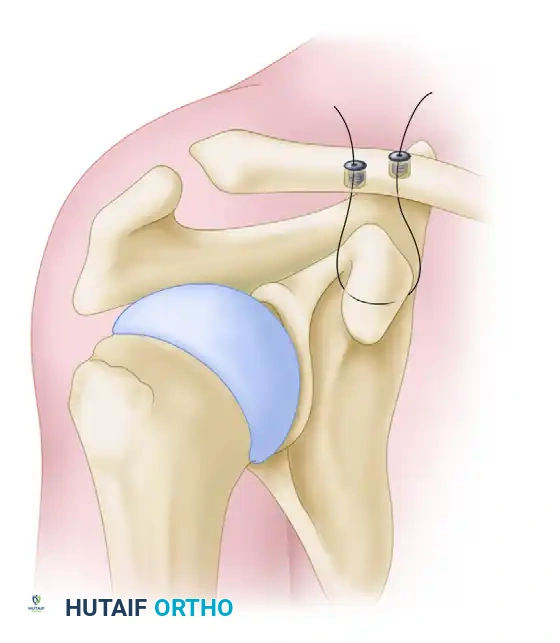
Figure 4: Supplemental suture fixation from the clavicle to the coracoid over the acromion for lateral clavicular fracture.
- Technique:
- The base of the coracoid is exposed via blunt dissection through the deltopectoral interval or directly inferior to the clavicle.
- Heavy nonabsorbable sutures (e.g., #5 or tape-like sutures) are passed under the base of the coracoid.
- Drill holes are made in the proximal clavicle fragment.
- The fracture is reduced, and the sutures are passed through the clavicular drill holes and tied over the superior cortex (or over a plate), effectively recreating the conoid and trapezoid ligaments.
- Advantages: Directly neutralizes the deforming forces, offloads the osteosynthesis hardware, and allows for robust biological healing of the fracture. It is particularly useful when the distal fragment is too small for adequate screw purchase.
Clinical Pearl: When utilizing CC suture fixation, ensure the sutures are passed under the base of the coracoid rather than the tip. Passing sutures too anteriorly on the coracoid tip risks anterior translation of the clavicle and potential cut-out through the bone.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Successful outcomes depend as much on meticulous postoperative rehabilitation as on surgical execution. The protocol must balance the need for early mobilization to prevent adhesive capsulitis with the necessity of protecting the fixation construct.
Phase I: Protection (Weeks 0-4)
- The patient is placed in a standard shoulder sling.
- Pendulum exercises are initiated immediately.
- Active range of motion (AROM) of the elbow, wrist, and hand is encouraged.
- Passive range of motion (PROM) of the shoulder is limited to 90 degrees of forward elevation and 30 degrees of external rotation to prevent excessive stress on the CC ligaments or hook plate.
Phase II: Active Motion (Weeks 4-8)
- The sling is discontinued.
- Active-assisted and active range of motion exercises are initiated.
- If a hook plate was used, elevation above 90 degrees may still be restricted or uncomfortable until the plate is removed.
- Radiographs are obtained at 6 weeks to assess callus formation and hardware integrity.
Phase III: Strengthening (Weeks 8-12+)
- Once clinical and radiographic union is confirmed, progressive resistance exercises are introduced.
- Focus is placed on periscapular stabilizers and rotator cuff strengthening.
- Return to heavy lifting or contact sports is typically delayed until 4 to 6 months postoperatively, and only after hardware removal if a hook plate or AC-spanning plate was utilized.
COMPLICATIONS
- Nonunion: While operative fixation drastically reduces nonunion rates compared to conservative management, it can still occur, particularly in cases of inadequate distal fixation or deep infection. Treatment requires revision open reduction internal fixation (ORIF) with autologous bone grafting.
- Hardware Prominence: The subcutaneous nature of the clavicle makes hardware prominence a common complaint. Up to 30% of patients may request plate removal after fracture consolidation.
- Acromial Osteolysis: Specifically associated with hook plates. The constant pressure of the hook against the undersurface of the acromion can lead to bone resorption and, rarely, acromial fracture. Early plate removal (at 3-4 months) is the definitive preventative measure.
- Post-traumatic AC Joint Arthrosis: Common in Type III fractures or cases where the AC joint was violated during surgery. If symptomatic, it is treated with intra-articular corticosteroid injections or, ultimately, a distal clavicle excision (Mumford procedure).
CONCLUSION
Lateral clavicular fractures demand careful evaluation of the coracoclavicular ligamentous complex. While stable Type I and III fractures are amenable to nonoperative care, unstable Type II fractures require surgical intervention to counteract the deforming forces of the trapezius and the weight of the arm. By employing advanced techniques such as precontoured locking plates, subacromial hook plates, and supplemental CC suture fixation, orthopedic surgeons can achieve the secure fixation necessary for high union rates and the restoration of optimal shoulder kinematics.
You Might Also Like