Open Reduction and Internal Fixation of Thumb Carpometacarpal Injuries

Key Takeaway
Open reduction and internal fixation (ORIF) of thumb carpometacarpal (CMC) joint injuries is critical for restoring hand biomechanics. This comprehensive guide details the Buchler external fixation technique for comminuted fractures, miniplate osteosynthesis for T-type Rolando fractures, and ligamentous repair for CMC dislocations. Emphasizing precise anatomical reduction and rigid fixation, these evidence-based protocols ensure optimal functional recovery and minimize post-traumatic osteoarthritis in complex thumb base trauma.
Introduction to Thumb Carpometacarpal Joint Trauma
Injuries to the thumb carpometacarpal (CMC) joint, including complex intra-articular fractures (such as Rolando fractures) and pure dislocations, present significant challenges to the orthopedic surgeon. The thumb CMC joint is a highly mobile, biconcave saddle joint that relies on a complex capsuloligamentous network for stability. Disruption of this joint—whether through highly comminuted intra-articular fractures or ligamentous avulsions—compromises the pinch and grip strength of the entire hand.
Open reduction and internal fixation (ORIF) is the gold standard for displaced intra-articular fractures and unstable dislocations of the thumb base. The primary surgical objective is the exact anatomical restoration of the articular surface to prevent rapid-onset post-traumatic osteoarthritis, coupled with stable fixation to allow early mobilization.
Clinical Pearl: The deforming forces at the thumb base are relentless. The abductor pollicis longus (APL) exerts a strong proximal and dorsal pull on the metacarpal shaft, while the adductor pollicis draws the distal metacarpal toward the palm. Any fixation construct must be robust enough to counteract these dynamic forces during the healing phase.
Surgical Anatomy and Biomechanics
Understanding the stabilizing structures of the thumb CMC joint is paramount for successful surgical intervention. Cadaveric and biomechanical studies have definitively identified the dorsoradial ligament (DRL) and the volar oblique ligament (VOL) as the primary restraints against joint subluxation and dislocation.
- The Volar Oblique Ligament (VOL): Originates from the volar tubercle of the trapezium and inserts onto the volar beak of the thumb metacarpal. It is a critical stabilizer during pinch mechanisms.
- The Dorsoradial Ligament (DRL): Often considered the strongest and most important ligament in preventing dorsal dislocation, it spans from the dorsal trapezium to the dorsal base of the metacarpal.
When a fracture occurs at the base of the thumb metacarpal (e.g., Bennett or Rolando fractures), the volar ulnar fragment typically remains anatomically reduced, tethered to the trapezium by the intact VOL. The larger metacarpal shaft fragment is displaced proximally, dorsally, and radially by the APL.
Preoperative Planning and Patient Positioning
Thorough preoperative evaluation requires true anteroposterior (AP), lateral, and Robert's view radiographs of the thumb to accurately assess the fracture pattern, degree of comminution, and articular step-off. Computed tomography (CT) with 3D reconstruction is highly recommended for complex, multi-fragmentary Rolando fractures to map the articular fragments.
Positioning:
* The patient is placed supine with the operative arm extended on a radiolucent hand table.
* A well-padded pneumatic tourniquet is applied to the proximal arm.
* Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, supplemented with intravenous sedation or general anesthesia depending on patient factors.
* Intraoperative fluoroscopy (C-arm) is positioned parallel to the hand table to allow seamless orthogonal imaging without disrupting the surgical field.
Surgical Technique 1: The Buchler Technique for Comminuted Fractures
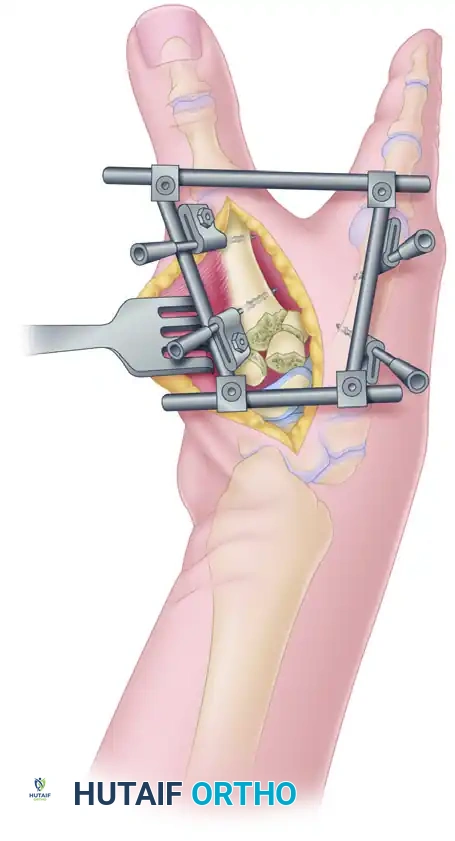
For highly comminuted intra-articular fractures of the thumb base where standard plate osteosynthesis is impossible due to fragment size, the Buchler technique utilizing an AO mini external fixator combined with limited open reduction is the treatment of choice. This technique leverages ligamentotaxis while allowing direct articular restoration.
Step 1: External Fixator Application
Place the AO mini external fixator between the thumb and index metacarpals in a quadrilateral frame configuration. This specific geometry provides multiplanar stability. Schanz pins are inserted percutaneously under fluoroscopic guidance, ensuring they are placed safely away from the fracture hematoma and the radial sensory nerve branches.
Step 2: Surgical Approach
Perform an open reduction through a radial palmar approach. The incision is made along the glabrous border of the thenar eminence, curving proximally toward the flexor carpi radialis (FCR) tendon.
* Carefully identify and protect the superficial branches of the radial nerve.
* Elevate the thenar musculature (abductor pollicis brevis and opponens pollicis) from its carpal origin to expose the thumb carpometacarpal joint capsule.
Step 3: Articular Reduction and Fixation
With the external fixator placed in slight distraction to utilize ligamentotaxis, perform a capsulotomy to visualize the joint surface.
* Gently elevate and align the displaced, depressed osteochondral joint fragments.
* Use the opposite, intact joint surface of the trapezium as a template for anatomical reduction.
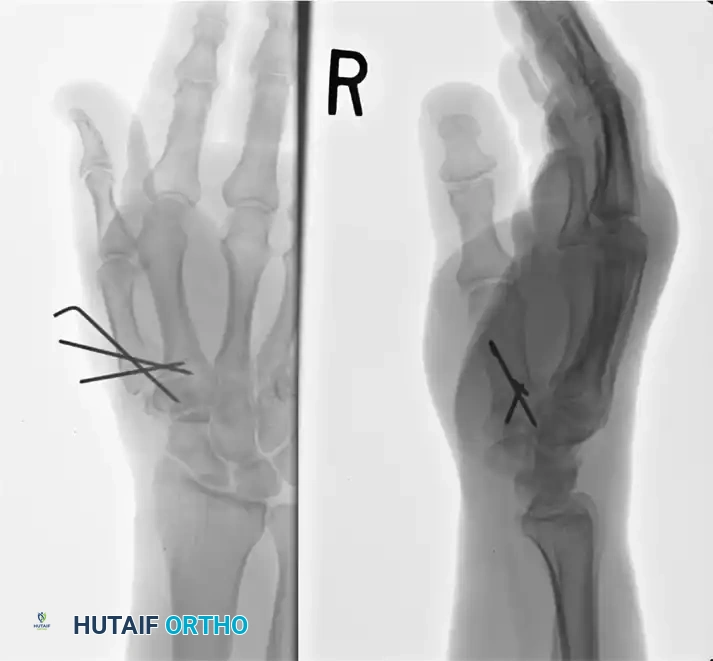
* Depending on the specific fracture configuration, secure the articular fragments using an interfragmentary screw (1.0 mm to 1.5 mm), fine Kirschner wires (0.8 mm to 1.0 mm), or a combination of both.
Step 4: Deformity Correction and Bone Grafting
Once the articular block is reconstructed, loosen the external fixation frame and adjust it to a position where the flexion deformity of the thumb metacarpal (distal to the fracture) is completely eliminated.
Surgical Warning: Correcting the flexion deformity often creates a significant defect of bone substance on the volar aspect of the proximal metaphyseal-diaphyseal junction.
To minimize subsequent settling of the fracture and hardware failure, this volar defect frequently requires structural bone grafting. Cancellous autograft from the distal radius or iliac crest should be packed tightly into the defect before final tightening of the external fixator.
Surgical Technique 2: Miniplate Osteosynthesis for T-Type Rolando Fractures
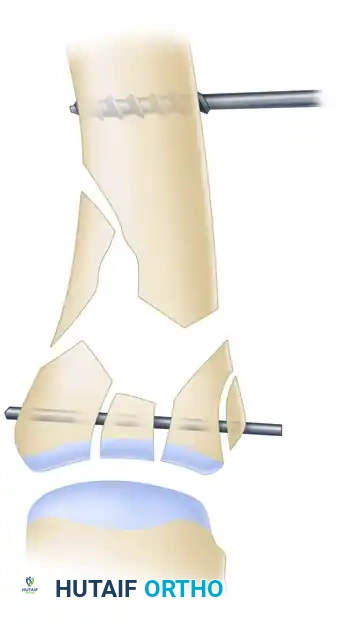
The T-type or Y-type Rolando fracture is a classic three-part intra-articular fracture at the base of the first metacarpal. When the fragments are large enough to accept screws, open reduction and internal fixation with a mini-fragment T-plate or condylar plate provides superior biomechanical stability.
Step 1: Fracture Exposure and Assessment
Following a similar radial palmar or dorsal approach (depending on the primary displacement), the fracture site is exposed. The classic T-type fracture pattern presents with a split in the articular surface and a transverse metaphyseal component.

Understanding the spatial relationship of the fragments is critical. The articular surface is typically split into volar and dorsal fragments, both of which are separated from the metacarpal shaft.
Step 2: Provisional Reduction
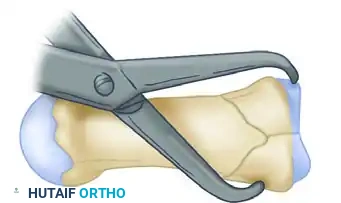
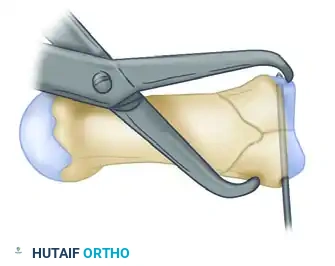
Longitudinal traction is applied to the thumb to overcome the deforming forces of the APL and adductor pollicis. A specialized reduction clamp is carefully applied across the articular fragments to restore the joint surface anatomically.
Once the articular block is reduced, it is provisionally stabilized using a fine Kirschner wire driven transversely across the fragments. This converts the complex three-part fracture into a simpler two-part fracture (the reconstructed articular base and the metacarpal shaft).
Step 3: Plate Positioning
Select an appropriately sized mini-fragment plate (typically a 1.5 mm or 2.0 mm T-plate). The plate is contoured to match the flare of the proximal metacarpal base. It is positioned over the reduced fracture, and a provisional K-wire may be used through the plate to hold it in place.
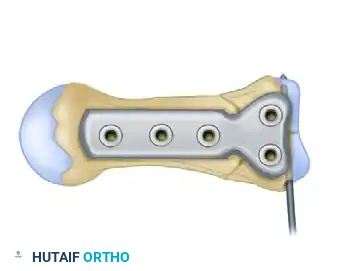
Step 4: Proximal Fixation and Compression
Drill the two proximal holes into the reconstructed articular block. To achieve dynamic compression across the transverse metaphyseal fracture line, offset drilling is utilized.
As the two proximal screws are inserted and tightened, the plate shifts slightly, compressing the proximal articular fragments tightly against the distal metacarpal shaft. This compression is vital for primary bone healing and construct rigidity.

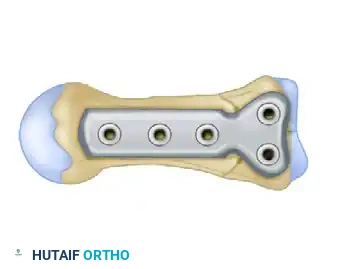
Step 5: Final Diaphyseal Fixation
With the articular block securely compressed to the shaft, the remaining distal holes along the metacarpal diaphysis are drilled, measured, and filled with appropriate cortical screws.

Fluoroscopy is used to confirm absolute anatomical reduction of the joint surface, correct screw length (avoiding penetration into the CMC joint or soft tissue tethering), and overall alignment.
Surgical Technique 3: Thumb Carpometacarpal Joint Dislocation
Pure dislocation of the thumb carpometacarpal joint is a remarkably rare injury, lacking the bony avulsion seen in Bennett fractures. Almost all reported cases in the literature are dorsal dislocations, driven by axial loading on a flexed thumb.
Acute Management (< 3 Weeks)
When a pure CMC dislocation occurs without fracture and is recognized early (within the first 3 weeks), immediate intervention is required.
* Closed Reduction: The dislocation should be reduced under adequate anesthesia using longitudinal traction, palmar pressure on the metacarpal base, and slight pronation.
* Immobilization: If the joint is perfectly stable post-reduction, cast immobilization in a thumb spica cast for 4 to 6 weeks is sufficient to allow capsuloligamentous healing and prevent recurrence.
Pitfall: Careful assessment of joint stability immediately after reduction is mandatory. Do not assume a reduced joint is a stable joint. The APL will continuously attempt to subluxate the metacarpal dorsally.
- Surgical Intervention for Instability: If the joint is unstable after closed reduction, operative intervention is required. Open reduction and percutaneous pinning (using one or two K-wires driven from the metacarpal into the trapezium) combined with direct primary repair of the torn dorsoradial ligament is necessary to ensure long-term joint stability. Immobilization for 6 weeks is indicated after the repair.
Chronic or Recurrent Management (> 3 Weeks)
If the reduction is delayed beyond 3 weeks, the native ligaments are typically retracted and scarred, making primary repair impossible. In these delayed presentations, or in cases of idiopathic/traumatic recurrent thumb CMC joint dislocation or subluxation, ligament reconstruction is advised.
Intermetacarpal Ligament Reconstruction:
This procedure utilizes a slip of the flexor carpi radialis (FCR) or abductor pollicis longus (APL) tendon to reconstruct the stabilizing ligaments (often mimicking the VOL or creating a tether between the first and second metacarpals).
* Indications: The operation is most helpful when the joint is demonstrably unstable and painful, and crucially, when degeneration of its articular surfaces is minimal.
* Contraindications: This procedure should not be done solely to relieve symptoms or subluxations of this joint resulting from advanced osteoarthritis. In the presence of significant degenerative changes, a trapeziectomy with ligament reconstruction and tendon interposition (LRTI) or CMC arthrodesis is the appropriate surgical pathway.
Postoperative Care and Rehabilitation Protocols
The success of thumb CMC joint surgery relies heavily on strict adherence to postoperative rehabilitation protocols. Premature mobilization can lead to hardware failure or loss of reduction, while prolonged immobilization results in debilitating stiffness.
Protocol Following External Fixation (Buchler Technique)
- Immediate Post-op: The hand is elevated to minimize edema. Pin site care is initiated using chlorhexidine or saline solutions to prevent superficial pin tract infections.
- Duration of Fixation: The external fixation frame is left in place for an average of 6 weeks (range, 5 to 12 weeks), depending on the severity of comminution and radiographic evidence of bridging callus.
- Monitoring: Interval radiographs should be obtained at 2, 4, and 6 weeks to assess the healing process and ensure the joint space is maintained without settling.
- Removal and Rehabilitation: After the fixator has been removed in the clinic, active and active-assisted range-of-motion (ROM) exercises are begun immediately under the guidance of a certified hand therapist.
- Splinting: A custom-molded, removable thermoplastic thumb spica splint is worn between exercise sessions and at night for an additional 6 to 12 weeks to protect the healing bone and ligaments.
Protocol Following Miniplate Osteosynthesis
- Immobilization: A volar resting splint or thumb spica splint is applied postoperatively.
- Early Motion: Because plate osteosynthesis provides rigid internal fixation, early protected active ROM of the interphalangeal and metacarpophalangeal joints can begin within the first week. Gentle CMC motion is typically initiated at 2 to 3 weeks, provided radiographic alignment is maintained.
- Strengthening: Pinch and grip strengthening are delayed until clinical and radiographic union is confirmed, usually around 8 to 10 weeks postoperatively.
Complications and Management
- Post-Traumatic Osteoarthritis: The most common long-term complication of intra-articular thumb base fractures. Even with anatomical reduction, the initial cartilage impact can lead to chondrocyte death. If symptomatic arthritis develops, salvage procedures such as CMC arthrodesis or trapeziectomy may be required.
- Hardware Prominence and Tendon Irritation: Miniplates on the dorsal or radial aspect of the metacarpal can irritate the extensor pollicis brevis or APL tendons. Hardware removal may be indicated after complete fracture consolidation (typically after 6-12 months).
- Pin Tract Infections: Common with the Buchler external fixation technique. Most resolve with oral antibiotics and aggressive local pin care. Deep infections requiring premature frame removal are rare but devastating.
- Loss of Reduction/Settling: Often seen if volar bone grafting was omitted during the correction of a flexion deformity in comminuted fractures. Requires close radiographic monitoring during the first 4 weeks.
Conclusion
The management of thumb carpometacarpal joint injuries demands a nuanced understanding of hand biomechanics and a versatile surgical armamentarium. Whether utilizing the Buchler external fixation technique for highly comminuted fractures, rigid miniplate osteosynthesis for T-type Rolando fractures, or precise ligamentous reconstruction for chronic dislocations, the overarching goal remains the same: restoration of articular congruity and joint stability. Through meticulous surgical execution and structured postoperative rehabilitation, surgeons can reliably restore the critical pinch and grasp functions of the thumb, minimizing the risk of long-term disability.
You Might Also Like