Mastering Radiology Interactive: Ace Perilunate Dislocation Cases

Key Takeaway
Here are the crucial details you must know about Mastering Radiology Interactive: Ace Perilunate Dislocation Cases. Mastering radiology interactive modules offer dynamic learning on complex carpal injuries like perilunate dislocations. These involve dorsal dislocation of the capitate, often due to axial wrist loading. Modules classify injuries (e.g., lesser arc) and explain management approaches, enhancing diagnostic and treatment skills for medical professionals through interactive questions and visual aids.
A 35-year-old male presents to the A&E following a high-energy fall onto his outstretched hand. He is in significant pain with a gross deformity of the wrist. Here is his initial AP radiograph.
Question: Please describe the radiographic findings shown in this AP view.
Candidate: The radiograph shows a loss of the normal carpal arcs (Gilula's lines). There is a transverse fracture of the scaphoid and the lunate appears triangular/wedged, suggesting a perilunate injury pattern.
Describing only the most obvious fracture while failing to comment on the carpal alignment or the specific shape of the lunate (the "triangular" sign), which is the hallmark of carpal dissociation.
Systematically address the Gilula lines, confirming they are disrupted at the midcarpal and radiocarpal joints. Identify the "trans-scaphoid" component of the injury. Highlight the triangular shape of the lunate, which indicates rotational instability. Mention the need to correlate with the lateral view to confirm the dorsal vs. volar nature of the displacement.
Following your assessment of the AP view, you examine the lateral view of the same patient.
Question: Describe the lateral radiograph and identify the specific pathology.
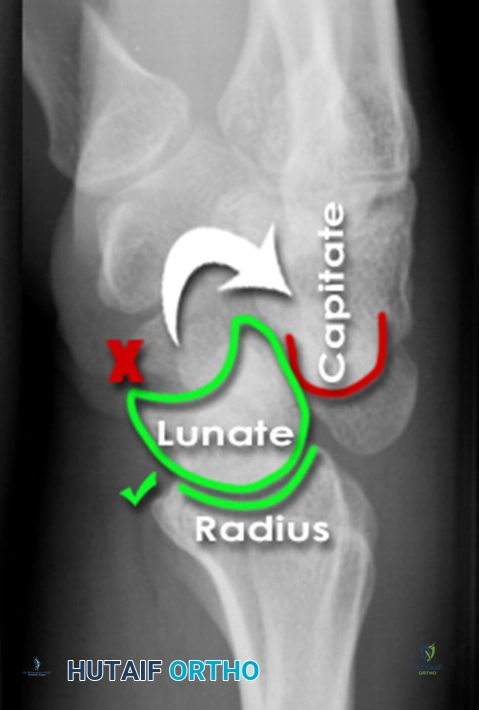
Candidate: The lateral view shows the capitate is dislocated dorsally relative to the lunate. The lunate remains within the lunate fossa of the distal radius. This is a dorsal perilunate dislocation.
Confusing a "perilunate dislocation" (where the lunate stays in the fossa) with a "lunate dislocation" (where the lunate is displaced volarly, the "spilled teacup sign").
Identify the relationship between the distal radius, lunate, and capitate. State clearly: "The lunate maintains its position in the lunate fossa, while the capitate is displaced dorsally. This confirms a dorsal perilunate dislocation." Mention that you would now assess the median nerve status immediately.
The patient has paresthesias in the median nerve distribution. You are in the emergency department.

Question: Outline your immediate management plan.
Candidate: I would attempt an immediate closed reduction under adequate sedation, followed by an urgent CT scan to assess the fracture pattern. If the median nerve symptoms persist, I would proceed to open reduction and carpal tunnel release.
Failing to mention the high risk of median nerve injury or omitting the need for a formal carpal tunnel release in the setting of neurological deficit.
Structure your answer: 1) Document neurovascular status. 2) Attempt closed reduction under procedural sedation to decompress the median nerve. 3) Obtain urgent CT wrist for surgical planning. 4) State that these injuries are usually unstable and mandate operative intervention (ORIF) with ligamentous repair/reconstruction, as closed treatment is rarely successful long-term.
