Perilunate Dislocation & PLFD: Comprehensive Guide to Anatomy, Diagnosis & Management

Key Takeaway
Perilunate dislocations (PLDs) are severe, high-energy wrist injuries characterized by carpal disruption around the lunate. Critical due to potential long-term morbidity, their diagnosis involves understanding surgical anatomy and Mayfield's classification of progressive ligamentous failure. Immediate and definitive surgical management is paramount for optimizing functional recovery and preventing chronic instability or post-traumatic arthritis.
A 28-year-old male presents to the Emergency Department following a high-speed motorcycle collision. He has a deformed, swollen right wrist. He complains of tingling in his thumb and index finger. What are your immediate priorities, and what do you expect to see on the lateral radiograph?
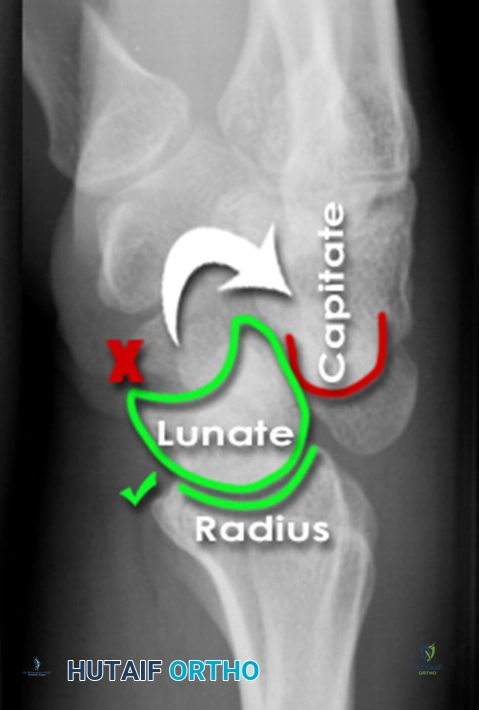
Candidate: I would perform a primary trauma survey to rule out life-threatening injuries. For the wrist, I would assess neurovascular status—specifically the median nerve, given the tingling. I would order plain radiographs. On a lateral view, I would look for a perilunate or lunate dislocation. In a perilunate dislocation, the lunate usually stays with the radius while the capitate is dorsally displaced. In a lunate dislocation, the lunate itself has volarly subluxated into the carpal tunnel.
Candidates often jump straight to discussing the classification or surgical approach without prioritizing the acute neurovascular status (carpal tunnel syndrome) or failing to mention that a high-energy mechanism requires exclusion of polytrauma (ATLS principles).
The perfect answer acknowledges: 1. ATLS/polytrauma clearance. 2. Urgent neurovascular assessment, specifically documenting median nerve sensory/motor deficits (acute carpal tunnel). 3. Radiographic analysis using "Gilula's Arcs." 4. Definitive differentiation: Perilunate (capitate dorsal to lunate) vs. Lunate (lunate rotated volarly/"spilled teacup").
You have diagnosed a Stage II Perilunate Dislocation. The patient is booked for theatre. Describe your surgical planning, specifically regarding the approach and the sequence of stabilization.
Candidate: I would plan for an open reduction. A combined dorsal and volar approach is usually required. I would use the dorsal approach to reduce the capitate onto the lunate and repair the scapholunate interosseous ligament. The volar approach allows for carpal tunnel release and fixation of the lunate if needed. I would stabilize with K-wires across the scapholunate and capitolunate joints.
Failing to mention the "Great Arc" injury. A candidate must address associated fractures (scaphoid/triquetrum/radial styloid). Simply saying "K-wires" is insufficient; the examiner wants to hear about anatomical reduction of the scaphoid and the sequence of ligamentous repair.
A high-scoring answer outlines a systemic approach: 1. Approach: Dorsal capsulotomy (protecting EPL). 2. Reduction: Correcting the "Great Arc" (fixating the scaphoid/radial styloid) followed by the "Lesser Arc" (ligamentous). 3. Fixation: SL, LC, and SC K-wires. 4. Volar: Indicated if median nerve decompression is required or if the lunate is irreducible. 5. Emphasize that anatomical reduction is the primary determinant of long-term prognosis.
Post-operatively, the patient is concerned about long-term function. How do you counsel them regarding the prognosis and potential complications?
Candidate: I would inform the patient that this is a severe injury. Despite surgery, they may face stiffness and a high risk of post-traumatic arthritis. I would explain that they will require long-term hand therapy and that there is a risk of persistent pain or median nerve issues.
Being overly optimistic. These are life-changing injuries. Candidates fail when they don't explicitly mention "Post-Traumatic Arthritis" (SLAC/SNAC wrist) or the likelihood that they will not regain pre-injury motion levels.
The gold standard provides a structured prognosis: 1. Short term: Need for dedicated hand therapy to combat stiffness. 2. Medium term: Risk of CRPS, persistent nerve symptoms, or non-union. 3. Long term: High likelihood (up to 100%) of post-traumatic arthritis (SLAC/SNAC), which may necessitate future salvage procedures such as four-corner fusion or proximal row carpectomy. Setting these expectations early is the sign of a senior surgeon.
