Masterclass in Open Reduction of Hand Dislocations: MCP and CMC Joints

Key Takeaway
Complex dislocations of the metacarpophalangeal (MCP) and carpometacarpal (CMC) joints often resist closed reduction due to soft tissue interposition. The Kaplan volar approach systematically releases the constricting anatomical "noose" around the metacarpal head. For CMC fracture-dislocations, precise restoration of articular congruity via percutaneous pinning or open reduction is paramount to preserve grip strength and prevent post-traumatic arthrosis.
Comprehensive Introduction and Patho-Epidemiology
The intricate biomechanics of the human hand rely on the precise anatomical alignment and unyielding stability of the metacarpophalangeal (MCP) and carpometacarpal (CMC) joints. These articulations serve as the foundational pillars for both power grip and fine motor dexterity. While many dislocations within the hand and wrist can be managed expeditiously with prompt closed reduction in the emergency department, specific high-energy injury patterns are notoriously irreducible. This irreducibility is almost exclusively dictated by complex soft tissue interposition, where the surrounding ligamentous and tendinous structures form an unyielding mechanical block. In these specific clinical scenarios, repeated and forceful attempts at closed reduction are not only futile but actively deleterious. Such misguided efforts risk catastrophic iatrogenic articular cartilage shear damage, exacerbation of soft tissue trauma, and devastating neurovascular compromise.
Epidemiologically, complex dislocations of the MCP joint most frequently involve the index finger, followed closely by the small finger. The central digits (long and ring fingers) are largely protected from such extreme displacement by the deep transverse metacarpal ligaments tethering them robustly on both sides. These injuries typically occur secondary to high-energy forced hyperextension, often sustained during athletic competition, motor vehicle collisions, or falls from a significant height. The hyperextension force violently ruptures the proximal membranous attachment of the volar plate, allowing the rigid distal cartilaginous portion to subluxate dorsally and become incarcerated above the metacarpal head. The failure to recognize this specific pathoanatomy often leads to delayed surgical intervention, significantly compromising the ultimate functional outcome.
Conversely, dislocations and fracture-dislocations of the carpometacarpal joints—particularly involving the highly mobile fourth and fifth rays—are predominantly the result of high-energy axial loading applied to a clenched fist. The classic mechanism is a forceful punch against a rigid object. Because the fourth and fifth CMC joints possess a native mobility of approximately 15 to 30 degrees of flexion and extension (compared to the essentially rigid second and third CMC joints), they are uniquely susceptible to dorsal subluxation and shearing fractures under axial loads. Furthermore, these injuries are frequently missed on initial presentation. The extensive overlapping osseous anatomy of the carpus on standard anteroposterior radiographs easily obscures subtle dorsal subluxations, leading to a high rate of delayed diagnosis. Unrecognized CMC fracture-dislocations invariably progress to painful malunions, profound grip weakness, and rapid post-traumatic osteoarthritis, necessitating complex salvage procedures.
This comprehensive masterclass details the advanced surgical management of irreducible hand dislocations. It focuses heavily on the classic Kaplan volar approach for complex MCP joint dislocations—a fundamental anatomical dissection every hand surgeon must master—and the systematic management of unstable CMC fracture-dislocations. Mastery of these techniques, coupled with a profound understanding of the underlying biomechanics, is an absolute prerequisite for orthopedic residents, hand surgery fellows, and practicing consultants aiming to restore optimal hand function in the setting of severe trauma.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the regional anatomy is the cornerstone of successfully managing complex hand dislocations. The metacarpophalangeal joint is a diarthrodial condyloid joint, uniquely stabilized by a complex arrangement of static and dynamic restraints. The metacarpal head possesses a distinct "cam" morphology; it is narrower dorsally and wider volarly. Consequently, the collateral ligaments are lax in extension (allowing abduction and adduction) and maximally taut in flexion (providing rigid lateral stability for power grip). The volar plate is a thick, fibrocartilaginous structure that prevents hyperextension. Its distal attachment to the proximal phalanx is thick and unyielding, while its proximal attachment to the metacarpal neck is membranous and relatively weak. This anatomical discrepancy explains why hyperextension injuries invariably cause proximal avulsion of the volar plate, allowing it to interpose between the joint surfaces.
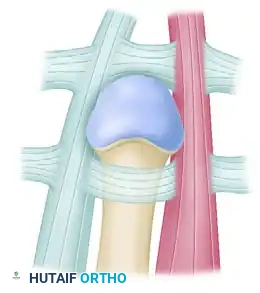
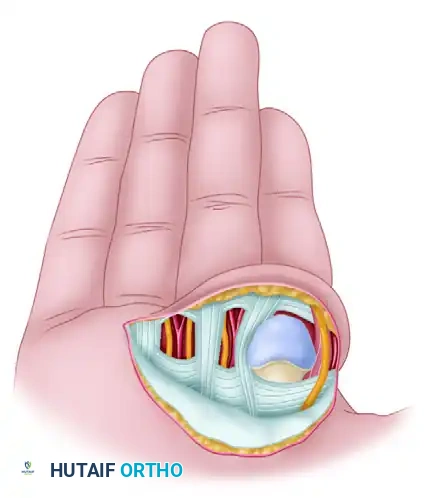
In a complex, irreducible dorsal dislocation of the index MCP joint, the metacarpal head is driven volarly through the weakest point of the joint capsule and becomes incarcerated in an unyielding anatomical "noose." Understanding the four distinct structures comprising this noose is critical for surgical decompression:
1. Volar Plate: Avulsed proximally, it is displaced dorsally over the metacarpal head, acting as a direct mechanical block to reduction.
2. Natatory Ligament: This distal fascial band tightens distally across the volar aspect of the metacarpal neck.
3. Superficial Transverse Metacarpal Ligament: This structure constricts the metacarpal neck proximally.
4. Lumbrical Muscle and Flexor Tendons: The lumbrical muscle displaces radially, and the flexor tendons (FDS and FDP) displace ulnarly. Together, they tightly flank the metacarpal neck, acting as the lateral and medial limbs of the constricting noose.
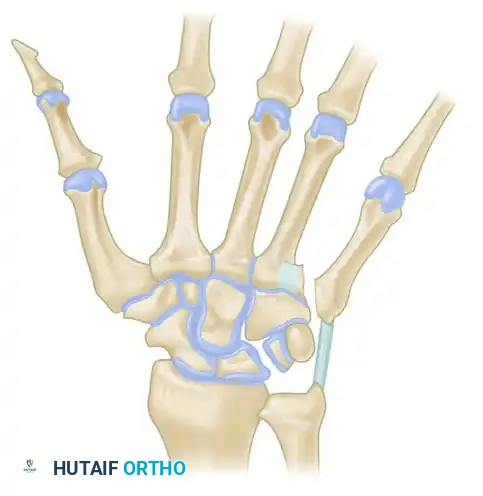
Moving proximally to the carpometacarpal joints, the biomechanical landscape shifts dramatically. The CMC articulations form a complex transverse and longitudinal arch system. The second and third metacarpals articulate rigidly with the trapezoid and capitate, respectively, forming the stable central pillar of the hand. In stark contrast, the fourth and fifth metacarpals articulate with the hamate and possess significant AP mobility. This mobility is essential for "cupping" the hand and maintaining a strong power grip. The dorsal CMC ligaments are inherently weaker than their robust volar counterparts; thus, axial loading forces typically drive the metacarpal bases dorsally.
A specific and highly unstable variant of the CMC fracture-dislocation involves the intra-articular fracture of the base of the fifth metacarpal, biomechanically analogous to the Bennett fracture of the thumb. In this injury pattern, the strong volar ligaments retain a small anteromedial articular fragment in its anatomical position against the hamate. However, the Extensor Carpi Ulnaris (ECU) tendon, which inserts robustly on the dorsoulnar base of the fifth metacarpal, exerts a powerful, unrelenting proximal and dorsal pull on the main metacarpal shaft. This dynamic deforming force results in proximal migration, shortening of the metacarpal, and persistent dorsal subluxation. Without rigid internal fixation, the continuous pull of the ECU guarantees the failure of any closed reduction attempt, making surgical stabilization mandatory.
Exhaustive Indications and Contraindications
The decision-making algorithm for the operative management of hand dislocations requires a meticulous assessment of the injury timeline, the specific anatomical structures involved, and the patient's physiological demands. Surgical intervention is not universally required for all dislocations, but failure to recognize the absolute indications for open reduction or rigid fixation will lead to catastrophic functional deficits. The following table delineates the strict indications and contraindications for the surgical techniques discussed in this masterclass.
| Clinical Parameter | Absolute Indications for Surgery | Relative Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| MCP Joint Dislocations | Irreducible complex dislocation with volar plate interposition; Open dislocation requiring formal debridement; Concomitant displaced intra-articular fracture. | Delayed presentation (>3 weeks) with severe stiffness; Subacute dislocations failing closed reduction under adequate anesthesia. | Active, uncontrolled local soft tissue infection (for internal fixation); Medically unstable polytrauma patient. | Severe preexisting osteoarthritis of the affected MCP joint (consider arthroplasty/arthrodesis instead); Non-compliant patient. |
| CMC Fracture-Dislocations | Unstable reduction of 4th/5th CMC joints; "Bennett-like" 5th metacarpal base fractures with ECU pull; Open fracture-dislocations; Polytrauma requiring immediate hand mobilization. | >1-2mm articular step-off in the hamatometacarpal joint; Delayed presentation (1-4 weeks) with early consolidation in a subluxated position. | Active osteomyelitis of the carpus or metacarpals; Critical ischemia of the hand requiring vascular repair prior to skeletal fixation. | Advanced age with extremely low functional demands; Severe baseline dementia precluding postoperative splint compliance. |
| Chronic Malunions | Painful, malunited 5th CMC fracture with profound grip weakness and dorsal bossing; Post-traumatic arthrosis failing conservative management (steroid injections, splinting). | Cosmetic deformity of the dorsal hand causing profound psychological distress; Impingement of extensor tendons over the malunited dorsal boss. | Painless malunion with acceptable grip strength and no functional limitations; Active local infection. | Heavy laborers requiring absolute power grip (arthrodesis may be preferred over resection arthroplasty in this specific cohort). |
When evaluating a complex MCP dislocation, the presence of a "dimple sign" on the volar aspect of the hand is a pathognomonic clinical indicator of an irreducible dislocation. This dimpling occurs because the palmar fascia is tethered by the displaced metacarpal head. In such cases, further attempts at closed reduction are strictly contraindicated, as they will merely tighten the anatomical noose and increase the risk of crushing the digital neurovascular bundles against the metacarpal condyles.
For CMC injuries, the threshold for surgical intervention is exceedingly low. The deforming forces of the intrinsic muscles and the ECU tendon make non-operative management of anything but a perfectly stable, anatomically reduced joint highly perilous. If a closed reduction of a fourth or fifth CMC dislocation slips even a millimeter on serial post-reduction radiographs, the surgeon must immediately pivot to percutaneous pinning or open reduction and internal fixation (ORIF). Relying on cast immobilization alone to counteract the powerful pull of the ECU is a historical fallacy that modern hand surgeons must abandon.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the vital bridge between a correct diagnosis and a flawless surgical execution. For both MCP and CMC dislocations, the clinical evaluation must begin with a rigorous assessment of the neurovascular status. In complex MCP dislocations, the digital nerves are stretched tautly over the prominent, volarly displaced metacarpal head. The surgeon must document two-point discrimination pre-operatively, as iatrogenic nerve injury during the surgical approach is the most feared complication.
Imaging is the cornerstone of pre-operative templating. For suspected CMC dislocations, standard posteroanterior (PA) and lateral radiographs are often insufficient due to the overlapping shadows of the trapezoid, capitate, and hamate.



A true lateral radiograph is absolutely mandatory. On a perfectly positioned true lateral, the shafts of the second through fifth metacarpals should align parallel to one another. Any dorsal divergence or "fanning" of the fourth or fifth metacarpal shafts relative to the stable third metacarpal is highly indicative of a CMC dislocation. Furthermore, a 30-degree pronated oblique view is specifically designed to profile the fourth and fifth CMC joints, throwing them clear of the central carpal overlap. If plain radiographs remain equivocal in the face of profound dorsoulnar hand swelling, a fine-cut computed tomography (CT) scan with 3D reconstructions is the gold standard. The CT scan allows the surgeon to map the exact location of articular comminution and accurately template the trajectory for K-wire or screw fixation.

Patient positioning and operating room setup must be standardized to ensure efficiency and safety. The procedure is typically performed under regional anesthesia (axillary or supraclavicular brachial plexus block), which provides excellent intraoperative muscle relaxation and prolonged postoperative analgesia. General anesthesia is reserved for polytrauma patients or those with contraindications to regional blocks. The patient is positioned supine with the operative extremity extended on a radiolucent hand table.
A well-padded pneumatic tourniquet is applied to the proximal arm and typically inflated to 250 mmHg (or 100 mmHg above systolic blood pressure) after exsanguination with an Esmarch bandage. A mini C-arm fluoroscopy unit is brought in perpendicular to the hand table. The surgeon should sit comfortably at the axilla, with the assistant positioned across the table. Prior to incision, all necessary hardware—including 0.045-inch and 0.062-inch Kirschner wires, a mini-fragment screw set (1.5mm and 2.0mm), and wire drivers—must be immediately available on the sterile back table. This level of preparation ensures that the surgeon can seamlessly transition from a planned closed reduction and percutaneous pinning (CRPP) to an open reduction if the joint proves irreducible.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires an uncompromising adherence to anatomical planes and rigid fixation principles. We will divide this section into the management of complex MCP dislocations via the Kaplan volar approach, and the stabilization of CMC fracture-dislocations.
Part I: The Kaplan Volar Approach for Complex MCP Dislocations
Emanuel Kaplan originally described the volar approach to systematically release the constricting elements of the anatomical noose. While a dorsal approach is advocated by some modern surgeons (to completely avoid neurovascular injury and to easily split the volar plate longitudinally), the Kaplan volar approach remains a fundamental, master-level technique that directly addresses the primary volar pathology.
Step 1: Incision and Critical Neurovascular Exposure
Begin the incision in the distal palmar crease, extending it obliquely into the thenar crease at the radial base of the index finger. This creates an extensile exposure over the prominent metacarpal head. Dissect bluntly through the subcutaneous tissues using fine tenotomy scissors. Surgical Warning: The digital neurovascular bundles are displaced superficially and stretched tightly over the prominent metacarpal head by the violent displacement of the injury. They are highly susceptible to iatrogenic transection during the initial skin incision. Identify the radial and ulnar digital nerves immediately, meticulously mobilize them, and retract them gently with vessel loops to ensure their absolute protection throughout the procedure.
Step 2: Systematic Release of the Constricting Bands
To achieve reduction without forceful, cartilage-damaging leverage, the constricting bands must be systematically divided in a precise sequence:
* First Release (Natatory Ligament): Identify the taut, transverse fibers of the natatory ligament running distally across the metacarpal neck. Divide these fibers completely using a #15 blade.
* Second Release (Superficial Transverse Metacarpal Ligament): Make a longitudinal incision through the transverse fibers of the superficial transverse metacarpal ligament. This incision should extend to the ulnar side of the first lumbrical muscle, effectively releasing the proximal constriction below the metacarpal head.
* Third Release (Volar Plate): This is the most critical step. The cartilaginous volar plate is interposed between the proximal phalanx and the metacarpal head. You must incise the free edge of the torn ligament longitudinally, down to the junction of the periosteum with the proximal phalanx. Clinical Pearl: The incision must penetrate the entire thickness of the plate; superficial division is often insufficient to break the suction seal and mechanical block.
Step 3: Joint Reduction and Closure
Once the three primary releases are performed, the anatomical noose is completely decompressed. Apply gentle longitudinal traction and direct volar pressure to the dorsal aspect of the proximal phalanx. The proximal phalangeal base should glide smoothly back into its normal anatomical position over the metacarpal head. Once reduced, the flexor tendons, the divided volar plate, and the neurovascular bundles will spontaneously restore to their normal anatomical resting positions. Irrigate the joint copiously to remove any intra-articular hematoma or debris. Close the skin wound in a routine manner with non-absorbable sutures. Crucial Rule: Do not attempt to primarily repair the volar plate. The extensive scarring that ensues will inevitably lead to severe, intractable flexion contractures of the MCP joint.
Part II: Management of 4th and 5th CMC Fracture-Dislocations
The primary goal of treating CMC injuries is the absolute anatomical restoration of the articular surface to preserve grip strength and prevent rapid post-traumatic osteoarthritis.
Closed Reduction and Percutaneous Pinning (CRPP)
Many acute CMC dislocations can initially be reduced closed. Reduction is achieved via sustained longitudinal traction combined with direct, forceful volar pressure over the dorsally displaced metacarpal bases.

However, due to the deforming pull of the ECU tendon, these reductions are notoriously unstable. If the reduction is tenuous or if an intra-articular fracture is present, percutaneous pinning is strictly required.



Under live fluoroscopic guidance, confirm anatomical alignment. Drive two 0.045-inch or 0.062-inch Kirschner wires percutaneously. The optimal biomechanical construct involves driving one wire transversely from the fifth metacarpal shaft into the stable fourth metacarpal shaft, and a second wire obliquely from the fifth metacarpal base directly into the hamate or capitate. This divergent wire construct neutralizes both the proximal pull of the ECU and the dorsal subluxation forces.



Open Reduction and Internal Fixation (ORIF) for the "Bennett-Like" Variant
If the intra-articular fragment of the fifth metacarpal base is large and displaced, closed reduction will fail. Make a dorsal longitudinal incision over the fifth CMC joint. Carefully identify and retract the dorsal sensory branch of the ulnar nerve. Mobilize the ECU tendon to visualize the joint capsule. Perform a longitudinal arthrotomy. Anatomically reduce the main metacarpal shaft to the volar-ulnar articular fragment held by the strong volar ligaments. Temporarily pin the reduction with a 0.035-inch K-wire. Fix the fracture using a 1.5mm or 2.0mm mini-fragment lag screw, ensuring the screw head is countersunk to prevent extensor tendon irritation. If the fragment is highly comminuted, bridge plating or multiple K-wires are utilized as a neutralization construct.
Part III: Resection Arthroplasty for Malunited CMC Fractures
Failure to recognize or adequately stabilize a fifth CMC fracture-dislocation leads to a painful malunion characterized by a prominent dorsal bossing and severe grip weakness. In chronic cases with established post-traumatic arthrosis, resection arthroplasty is the preferred salvage procedure over corrective osteotomy.

Expose the fifth CMC joint via a dorsal longitudinal incision. Resect the malunited, arthritic base of the fifth metacarpal using an oscillating saw, removing approximately 5-7mm of bone to ensure no impingement against the hamate during power grip. The Crucial Step: The ECU tendon, which is often contracted, must be meticulously identified and securely reattached to the remaining fifth metacarpal shaft or transferred to the fourth metacarpal base. Failure to re-tension the ECU will result in a profound loss of ulnar deviation power and destabilize the entire ulnar border of the hand. Interposition of local soft tissue (such as a distally based slip of the ECU or local capsular tissue) is frequently utilized to fill the dead space and provide a biologic buffer against the hamate.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the open reduction of hand dislocations can be profound. The surgeon must be acutely aware of these risks, actively counsel the patient pre-operatively, and possess the technical repertoire to manage them when they arise.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| Iatrogenic Digital Nerve Injury | 2% - 5% (Kaplan Approach) | Superficial displacement of the nerve over the prominent metacarpal head; Blind subcutaneous dissection. | Prevention: Meticulous blunt dissection; early identification and vessel loop retraction. Salvage: Immediate microsurgical epineural repair using 8-0 or 9-0 nylon. |
| Post-Operative Joint Stiffness | 15% - 25% | Prolonged immobilization (>3 weeks); Extensive capsular scarring; Failure to initiate early active ROM. | Prevention: Limit immobilization to 1 week for MCP joints; use dynamic splinting. Salvage: Aggressive hand therapy; formal open surgical capsulotomy/tenolysis if refractory after 6 months. |
| Pin Tract Infection (CRPP) | 5% - 10% | Exposed K-wires; Poor patient hygiene; Prolonged pin retention (>6 weeks). | Prevention: Bury K-wires beneath the skin if possible; meticulous weekly pin care with chlorhexidine. Salvage: Immediate pin removal if deep infection is suspected; oral or IV antibiotics covering staphylococcal species. |
| Loss of Reduction / Hardware Failure | 3% - 8% | Inadequate K-wire spread; Failure to capture the stable carpus (hamate/capitate); Non-compliance with splinting. | Prevention: Use divergent K-wire constructs; utilize 0.062-inch wires in heavy laborers; strict cast immobilization. Salvage: Revision ORIF with bridge plating; progression to CMC arthrodesis if cartilage is severely damaged. |
| Post-Traumatic Osteoarthritis | 20% - 40% (Long-term) | Initial articular cartilage shear injury; Inadequate restoration of joint congruity (>1mm step-off). | Prevention: Anatomic reduction of all intra-articular fractures; avoid repeated forceful closed reductions. Salvage: CMC resection arthroplasty (with ECU tenodesis) or formal CMC arthrodesis for high-demand laborers. |
The most devastating acute complication during the Kaplan approach is the iatrogenic transection of the radial digital nerve to the index finger. Because the metacarpal head is driven volarly, it acts like a tent pole, pushing the neurovascular bundle immediately deep to the dermis. If a scalpel is used aggressively to divide the palmar fascia, the nerve is highly vulnerable. If transected, the surgeon must immediately convert to a microsurgical repair.
In the management of CMC injuries, loss of reduction is a frequent complication when surgeons rely solely on transverse intermetacarpal pinning. The powerful proximal pull of the ECU tendon can cause the fifth metacarpal to migrate proximally, effectively "windshield-wipering" the transverse K-wires through the cancellous bone. To prevent this, at least one robust K-wire must be driven longitudinally or obliquely across the CMC joint directly into the rigid carpus (hamate or capitate) to neutralize the longitudinal forces.
Phased Post-Operative Rehabilitation Protocols
The surgical intervention is merely the first step in restoring hand function; the postoperative rehabilitation protocol is equally critical. The delicate balance between protecting the surgical repair and preventing debilitating stiffness requires a highly coordinated effort between the orthopedic surgeon, the certified hand therapist (CHT), and the patient.
Phase I: Acute Protection and Edema Control (Weeks 0-2)
* For MCP Open Reductions: The hand is placed in a custom-molded dorsal blocking splint immediately post-operatively. The splint maintains the wrist in 20 degrees of extension and the MCP joints in 30 to 40 degrees of flexion. This position prevents hyperextension (which would stress the healing volar structures) while keeping the collateral ligaments stretched to prevent contracture. Crucially, the interphalangeal (IP) joints are left entirely free. The patient is instructed to perform immediate, aggressive active range of motion (ROM) of the IP joints to prevent flexor and extensor mechanism adhesions. Edema control via elevation and compressive wrapping is paramount.
* For CMC Pinning/ORIF: The hand is immobilized in a bulky, rigid short-arm cast or a custom orthosis incorporating the fourth and fifth digits in an intrinsic-plus position (MCPs flexed 70 degrees, IP joints extended). Absolute immobilization of the wrist and CMC joints is required to protect the K-wires and allow early osseous and ligamentous consolidation.
Phase II: Controlled Mobilization (Weeks 2-6)
* For MCP Open Reductions: At 1 to 2 weeks, the dorsal blocking splint is converted to a removable orthosis. Supervised active ROM of the MCP joint is initiated within the safe zone of flexion. If
