Operative Management of Bennett Fractures and Thumb CMC Joint Trauma
Key Takeaway
The thumb carpometacarpal joint is critical for hand function. Bennett fractures, characterized by intraarticular displacement of the first metacarpal base, compromise this stability. Deforming forces from the abductor pollicis longus necessitate precise reduction. While closed reduction and percutaneous pinning remain the gold standard for reducible fractures, open reduction is mandated for persistent articular incongruity exceeding 2 millimeters to prevent post-traumatic arthrosis and preserve pinch strength.
Comprehensive Introduction and Patho-Epidemiology
The trapeziometacarpal or carpometacarpal (CMC) joint of the thumb is the biomechanical cornerstone of the human hand, providing the unique capacity for opposition and prehension. Traumatic disruption of this articulation, particularly through an intra-articular fracture of the first metacarpal base, represents a critical threat to hand function. In 1882, the eminent Irish surgeon Edward Hallaran Bennett first meticulously described the classic intra-articular fracture-dislocation that now bears his name. The Bennett fracture is fundamentally defined as a two-part fracture-dislocation of the first metacarpal base, characterized by a highly predictable and consistent pattern of displacement driven by unopposed dynamic muscular forces.
The patho-epidemiology of Bennett fractures reveals a strong predilection for young, active male patients, typically occurring in the second to fourth decades of life. The classic mechanism of injury involves a high-energy axial load applied to a partially flexed and adducted thumb metacarpal. This force vector is frequently encountered during fist fights (punching with an improperly clenched fist), athletic endeavors such as rugby or martial arts, and high-velocity motor vehicle or motorcycle collisions. When the axial load is transmitted through the metacarpal shaft, the volar-ulnar aspect of the metacarpal base is sheared off against the unyielding articular surface of the trapezium, initiating the fracture-dislocation cascade.
Understanding the exact mechanism of injury is paramount for both diagnosis and operative planning. Because the fracture is generated by an axial load combined with adduction, the resulting fracture morphology consistently leaves a small, captive volar-ulnar lip fragment anatomically reduced, while the remainder of the metacarpal shaft is displaced. If left untreated or inadequately reduced, this precise pathoanatomy invariably leads to a cascade of functional deficits. These include severe limitation of motion, chronic debilitating pain, and a profound weakness in both pinch and grip strength due to the altered kinematics of the thumb ray.
Furthermore, the epidemiological shift towards higher-energy trauma has increased the incidence of complex Bennett-variant fractures, where the injury is not an isolated event but part of a broader spectrum of severe hand trauma. In these scenarios, the primary intra-articular fracture may be accompanied by severe soft tissue degloving, intrinsic muscle crush injuries, and compartment syndrome. Consequently, the modern orthopedic surgeon must be equipped to handle not only the isolated, closed Bennett fracture but also the catastrophic, open hand injury where the thumb CMC joint is fundamentally compromised.
Detailed Surgical Anatomy and Biomechanics
The integrity of the thumb CMC joint is arguably more critical to the overall function of the hand than any other single articulation. Functioning as a highly mobile, biconcave-biconvex saddle joint, it facilitates a complex range of motion across multiple planes. This geometric configuration allows for flexion, extension, abduction, adduction, and the essential composite motion of opposition. The inherent bony architecture of the trapeziometacarpal joint provides relatively little intrinsic stability; therefore, the joint relies heavily on a robust capsuloligamentous complex to maintain congruency during the tremendous forces generated by pinch and grip.
Stability is primarily conferred by the anterior oblique ligament (AOL)—often referred to as the volar oblique ligament or the "beak" ligament—and the dorsoradial ligament (DRL). The AOL originates from the palmar tubercle of the trapezium and inserts onto the volar-ulnar beak of the first metacarpal base. It acts as the primary restraint against dorsal and radial subluxation of the metacarpal base during active pinch. Recent biomechanical studies also highlight the critical importance of the DRL, which functions as the primary restraint to dorsal dislocation when the thumb is in pronation. In a Bennett fracture, the AOL remains firmly attached to the volar-ulnar fracture fragment, tethering it to the trapezium and maintaining its anatomical position, while the capsular attachments to the rest of the metacarpal are disrupted.
The pathoanatomy and subsequent displacement of a Bennett fracture are dictated entirely by unopposed deforming muscular forces acting on the destabilized metacarpal shaft. The main shaft of the first metacarpal is forcefully displaced proximally, dorsally, and radially by the robust pull of the abductor pollicis longus (APL), which inserts at the dorsal-radial base of the metacarpal. Simultaneously, the adductor pollicis (AP) exerts a powerful deforming force on the distal aspect of the metacarpal, pulling the shaft into adduction and supination. This dual-force vector effectively pivots the metacarpal shaft around the intact volar fragment, creating the classic clinical deformity of a shortened, adducted thumb with a prominent dorsal mass at the base.
Secondary kinematic collapse patterns frequently follow the dorsal displacement of the thumb basal joint. The most notable of these is the metacarpophalangeal (MCP) joint hyperextension deformity. This "zigzag" collapse occurs because the proximal migration of the metacarpal alters the resting tension of the extrinsic tendons (specifically the extensor pollicis longus and brevis), severely weakening pinch and grip strength. Reestablishing absolute stability, restoring the precise length of the first ray, and achieving articular congruency at the trapeziometacarpal joint are paramount to reversing these deforming vectors and restoring normal hand kinematics.
Exhaustive Indications and Contraindications
The management of Bennett fractures is governed by the absolute necessity to restore articular congruency and joint stability. Considerable historical controversy has surrounded the acceptable limits of articular displacement. While anatomical reduction remains the universal gold standard, biomechanical and long-term clinical studies suggest that minor articular incongruity (1 to 2 mm) may be tolerated, provided that solid bony union and absolute joint stability are achieved. However, persistent subluxation or step-offs greater than 2 mm significantly increase focal contact pressures across the saddle joint, rapidly accelerating the onset of post-traumatic osteoarthritis. Therefore, precise indications for operative intervention must be strictly adhered to.
Indications for Operative Intervention
Operative management is universally indicated for any Bennett fracture demonstrating joint subluxation, regardless of the size of the fracture fragment. Furthermore, any articular step-off or gap exceeding 1 to 2 mm on true orthogonal radiographs mandates surgical reduction. Closed reduction and percutaneous pinning (CRPP) is indicated for acute fractures (typically less than 10-14 days old) where anatomical reduction can be achieved and maintained via closed maneuvers. Open reduction and internal fixation (ORIF) is strictly indicated in the following scenarios: failure to achieve or maintain a closed reduction, presentation of a delayed or neglected fracture (greater than 2-3 weeks old), interposition of soft tissue (typically the capsule or APL tendon) blocking reduction, or the presence of a large volar-ulnar fragment that is amenable to interfragmentary lag screw fixation.
Contraindications to Operative Intervention
Absolute contraindications to operative management are exceedingly rare but include active, uncontrolled local soft tissue infection or osteomyelitis. Relative contraindications encompass severe, life-threatening polytrauma where the patient is medically unstable for prolonged anesthesia, though rapid percutaneous pinning may still be performed as a damage-control measure. Additionally, non-ambulatory patients with profoundly low functional demands, severe baseline dementia, or pre-existing end-stage trapeziometacarpal osteoarthritis may be candidates for non-operative management (e.g., cast immobilization) or primary salvage procedures, as the rigorous postoperative rehabilitation required for ORIF may not be feasible or beneficial.
Summary Table of Indications and Contraindications
| Clinical Scenario | Operative Indication | Primary Surgical Modality | Contraindications / Special Considerations |
|---|---|---|---|
| Acute, < 2mm step-off, stable | Relative (often non-operative) | Spica Casting / CRPP if unstable | Non-compliant patient (requires strict casting) |
| Acute, > 2mm step-off, subluxed | Absolute | CRPP (if reducible) or ORIF | Active overlying cellulitis |
| Large volar fragment (>33% of base) | Absolute | ORIF with Lag Screws | Severe comminution precluding screw purchase |
| Delayed presentation (> 3 weeks) | Absolute | ORIF with joint debridement | Pre-existing severe CMC osteoarthritis |
| Polytrauma / Crush Injury | Absolute (Damage Control) | Spanning K-wires / Ex-Fix | Medically unstable for prolonged surgery |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning begins with obtaining high-quality, specialized radiographic imaging. Standard posteroanterior and lateral views of the hand are insufficient for evaluating the thumb CMC joint due to the unique 30-degree pronated and abducted orientation of the first metacarpal relative to the rest of the palm. A "True AP" of the thumb CMC joint, also known as the Robert's view, is mandatory. This is obtained by maximally pronating the patient's arm and placing the dorsum of the thumb firmly against the radiographic cassette, with the X-ray beam directed anteroposteriorly through the CMC joint. A true lateral view is equally critical and is obtained by pronating the hand 30 degrees from the standard lateral position.
In cases of suspected severe comminution (transitioning toward a Rolando fracture pattern) or when the exact size of the volar-ulnar fragment is ambiguous, a pre-operative computed tomography (CT) scan with 3D reconstructions is highly recommended. The CT scan allows the surgeon to precisely quantify the articular step-off, assess the bone stock of the volar fragment for potential lag screw fixation, and identify any occult impaction of the central articular surface. Templating should be performed to anticipate the size and trajectory of fixation hardware. The surgeon must ensure the availability of 0.045-inch and 0.062-inch Kirschner wires, as well as a comprehensive mini-fragment set containing 1.5 mm and 2.0 mm cortical screws.
Patient positioning is standardized for both CRPP and ORIF. The patient is placed supine on the operating table with the affected extremity extended onto a radiolucent hand table. A well-padded upper arm tourniquet is applied to ensure a bloodless surgical field, which is absolutely critical for the meticulous dissection required during an open approach. The C-arm fluoroscopy unit is typically positioned parallel to the surgeon, entering from the head or the foot of the hand table, allowing for unobstructed, dynamic multi-planar imaging throughout the procedure.
Preparation of the surgical site must be expansive, extending from the fingertips to the proximal forearm, to allow for potential extensile exposures or the harvesting of bone graft if necessary. The surgeon should be seated comfortably, with the assistant positioned opposite. Prior to inflation of the tourniquet, a formal time-out is conducted, and prophylactic intravenous antibiotics are administered. The initial fluoroscopic assessment is performed before the skin incision to confirm the fracture pattern under anesthesia and to test the reducibility of the fracture via closed manipulation, which dictates the immediate surgical algorithm.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of Bennett fractures demands a systematic approach to counteract the inherent deforming forces. The procedure typically begins with an attempt at closed reduction and percutaneous pinning (CRPP). If anatomical reduction is unachievable or unmaintainable, the surgeon must seamlessly transition to open reduction and internal fixation (ORIF). Furthermore, in the setting of complex, high-energy hand trauma, the principles of damage control and aggressive soft tissue management must be integrated into the fixation strategy.
Closed Reduction and Percutaneous Pinning (CRPP)
The reduction maneuver, as popularized by Wagner, must systematically reverse the specific deforming muscular forces. First, the surgeon applies strong, sustained longitudinal axial traction to the thumb ray to overcome the proximal pull of the abductor pollicis longus (APL). Second, the thumb is brought into palmar abduction to correct the adduction deformity caused by the adductor pollicis. Third, the metacarpal shaft is pronated to correct the supination deformity. Finally, while maintaining these positions, firm, direct pressure is applied over the dorsal-radial aspect of the first metacarpal base, effectively pushing the displaced shaft volarly and ulnarly to reduce it to the captive volar-ulnar fragment.
Once the reduction is confirmed as anatomical via multi-planar fluoroscopy (utilizing the true AP and lateral views), percutaneous fixation is achieved using smooth Kirschner wires. The primary K-wire (typically 0.045-inch) is driven from the dorsal-radial aspect of the first metacarpal base, directed proximally and ulnarly, crossing the CMC joint, and purchasing the dense cortical bone of the trapezium. Care must be taken to avoid over-penetration into the scaphoid or the flexor carpi radialis tendon sheath. To neutralize the adduction forces and provide essential rotational stability, a second K-wire is frequently placed transversely from the first metacarpal shaft directly into the second metacarpal. The pins are subsequently cut outside the skin and bent to facilitate removal in the clinic.
Open Reduction and Internal Fixation (ORIF)
Should closed reduction leave an articular step-off greater than 2 mm, ORIF is strictly indicated. The Wagner surgical approach is utilized. A curved or L-shaped incision is made along the glabrous border of the thenar eminence, curving dorsally over the CMC joint. Superficial dissection requires meticulous identification and protection of the sensory branches of the superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve (LABCN). Retraction of these nerves must be gentle to prevent debilitating postoperative neuromas.
Deep dissection involves elevating the thenar musculature (specifically the abductor pollicis brevis and the opponens pollicis) subperiosteally from the first metacarpal shaft and reflecting them volarly. A longitudinal or T-shaped capsulotomy of the CMC joint is then performed to expose the articular surface and the fracture hematoma. The fracture site is thoroughly debrided of hematoma, small osteochondral debris, and any interposed capsular tissue. The metacarpal shaft is anatomically reduced to the volar-ulnar fragment under direct visualization using a pointed reduction forceps. If the volar fragment is sufficiently large (typically greater than one-third of the articular surface), definitive fixation is achieved using one or two 1.5 mm or 2.0 mm mini-fragment lag screws. If the fragment is too small or comminuted for screw purchase, multiple parallel K-wires are utilized to secure the reduction. The capsule is then meticulously repaired to restore the integrity of the dorsoradial ligament.
Management of Complex Combined Hand Trauma
In high-energy crush injuries, a Bennett fracture frequently presents as part of a catastrophic spectrum of hand trauma, including multiple concomitant metacarpal fractures, severe soft tissue degloving, and profound muscle devitalization. In these scenarios, the principles of damage control orthopedics take absolute precedence. Surgical debridement must be aggressive, systematic, and thorough to prevent deep space infections, myonecrosis, and subsequent osteomyelitis.

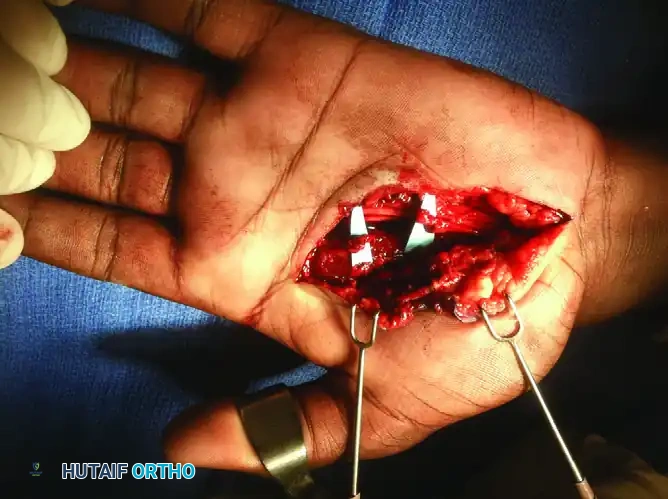
Initial exposure of a complex dorsal hand injury requires wide extension of the surgical incisions to fully assess the zone of injury. As demonstrated in the image above, retractors are strategically placed to evaluate the integrity of the extensor apparatus, the dorsal capsular structures, and the underlying intrinsic musculature. The true extent of the skeletal and soft tissue disruption is often vastly underappreciated on pre-operative imaging.
During the exploration of these high-energy crush injuries, devitalized muscle tissue must be meticulously identified and excised. The image above demonstrates the critical surgical débridement of devitalized second and third dorsal interossei. The "4 C's" of muscle viability (color, consistency, contractility, and capacity to bleed) must be rigorously applied. Failure to adequately debride necrotic intrinsic muscle bellies will inevitably lead to severe ischemic contractures (the dreaded intrinsic-plus hand deformity) or catastrophic deep infections.
Once the soft tissue bed has been adequately debrided, irrigated, and stabilized, rigid skeletal fixation is applied. In complex, highly comminuted fractures where traditional plate or lag screw fixation is impossible due to bone loss or severe fragmentation, large-diameter Kirschner wires provide excellent, versatile, and rapid stabilization.


The radiographs above demonstrate the final fixation of complex metacarpal trauma utilizing large Kirschner wires. This intramedullary or trans-articular pinning technique is a highly effective damage-control strategy. It maintains longitudinal alignment, restores the functional length of the ray, and prevents the collapse of the vital metacarpal arch while the severe soft tissue injury heals. Once the soft tissue envelope is secure, definitive reconstruction or bone grafting can be staged appropriately.
Complications, Incidence Rates, and Salvage Management
Despite meticulous pre-operative planning and flawless surgical execution, complications can and do arise in the operative management of Bennett fractures. The surgeon must be profoundly aware of these potential pitfalls, actively work to mitigate their occurrence, and possess the surgical armamentarium required to manage them effectively should they arise. Complications range from minor soft tissue issues to devastating joint destruction requiring complex salvage arthroplasty.
Loss of reduction is a frustrating early complication, most commonly occurring within the first two to three weeks postoperatively. This typically results from inadequate initial fixation—such as utilizing Kirschner wires that are too small in diameter (e.g., 0.035-inch) to withstand the robust deforming forces of the APL and AP—or from a failure to achieve true anatomical reduction initially. Frequent, high-quality radiographic follow-up during the first three weeks is mandatory to detect early displacement. If loss of reduction is identified early, immediate revision surgery (often requiring an open approach) is indicated.
Post-traumatic osteoarthritis (OA) is the most frequent and functionally limiting long-term complication. While minor articular incongruities (1-2 mm) may be tolerated in lower-demand patients, significant step-offs or persistent joint subluxation lead to rapid, asymmetric cartilage wear. Symptomatic post-traumatic OA presents with chronic pain at the base of the thumb, weakness in pinch grip, and a positive grind test. When conservative measures (NSAIDs, splinting, intra-articular corticosteroid injections) fail, salvage procedures are required. The primary salvage options include trapeziometacarpal arthrodesis (preferred in young, heavy manual laborers) or ligament reconstruction and tendon interposition (LRTI) arthroplasty (preferred in older or lower-demand patients seeking motion preservation).
Sensory nerve injury is a highly morbid complication that can overshadow a perfect radiographic result. The superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve (LABCN) are highly susceptible to iatrogenic injury during both percutaneous pinning and open approaches. Injury can result from direct laceration, traction neuropraxia, or entrapment within the scar tissue. Neuromas in this region are profoundly debilitating, often leading to complex regional pain syndrome (CRPS). Prevention is paramount: blunt dissection down to the bone, the use of soft tissue protectors during drilling, and meticulous retraction techniques are essential.
Summary Table of Complications and Salvage Strategies
| Complication | Estimated Incidence | Primary Etiology | Management / Salvage Strategy |
|---|---|---|---|
| Loss of Reduction | 5% - 10% | Inadequate pin size, poor initial reduction | Early revision ORIF, larger K-wires |
| Post-Traumatic OA | 15% - 25% | Articular step-off > 2mm, persistent subluxation | LRTI Arthroplasty or CMC Arthrodesis |
| Superficial Pin Infection | 10% - 15% | Poor local hygiene, prolonged pin retention | Oral antibiotics, aggressive local pin care |
| Deep Joint Infection | < 1% | Unrecognized open injury, systemic bacteremia | I&D, hardware removal, IV antibiotics |
| Sensory Neuroma (SRN) | 2% - 5% | Iatrogenic injury during drilling or dissection | Neuroma excision, nerve burying into muscle |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of Bennett fractures is a complex endeavor that requires a delicate, highly coordinated balance between protecting the fragile articular reduction and preventing debilitating, long-term stiffness of the thumb ray. The rehabilitation protocol must be phased, structured, and closely monitored by both the operating surgeon and a certified hand therapist (CHT). The timeline is dictated by the method of fixation, the quality of the bone, and the radiographic progression of fracture consolidation.
Phase 1: Immobilization Phase (Weeks 0-4)
Immediately following the surgical procedure, the patient is placed in a bulky, well-padded, rigid thumb spica splint in the operating room. This initial splint provides critical soft tissue rest, minimizes dead space, and controls postoperative edema. At the 10 to 14-day postoperative mark, the patient returns to the clinic for suture removal and a thorough wound check. If the soft tissues are healing appropriately, the patient is transitioned to a custom-molded, short-arm fiberglass thumb spica cast. Crucially, the interphalangeal (IP) joint of the thumb may be left free to allow for active flexion and extension, which prevents extensor pollicis longus (EPL) tendon adhesions, provided the specific fracture pattern and fixation construct allow for it. During this entire phase, strict elevation and aggressive active range of motion (AROM) of all uninvolved digits, the elbow, and the shoulder are heavily encouraged to mitigate edema and reduce the risk of complex regional pain syndrome (CRPS).
Phase 2: Pin Removal and Mobilization (Weeks 4-6)
At approximately 4 to 6 weeks postoperatively, orthogonal radiographs (including the true AP and lateral views) are obtained out of the cast to assess for clinical and radiographic union. The surgeon looks for the obliteration of the fracture line and the presence of bridging trabecular callus. Once clinical union is confirmed (defined as a non-tender fracture site with radiographic healing), the percutaneous K-wires are removed in the outpatient clinic setting. Following pin removal, the patient is immediately fitted with a custom thermoplastic thumb spica splint by the hand therapist. This splint is worn continuously, removed only for specific, therapist-directed exercise sessions and hygiene. Active range of motion (AROM) of the thumb CMC and MCP joints is initiated. The focus is on restoring palmar abduction, radial abduction, and opposition. Passive range of motion (PROM) is strictly avoided during this phase to prevent stretching of the healing capsuloligamentous complex and potential secondary subluxation.
Phase 3: Strengthening and Maturation Phase (Weeks 6-12)
As the patient progresses into the 6 to 8-week window, and provided that AROM is improving without pain, passive range of motion (PROM) and gentle dynamic splinting may be cautiously introduced if significant stiffness persists. Progressive strengthening exercises are initiated at 8 weeks postoperatively. The therapy program shifts focus toward restoring the intricate mechanics of pinch (key pinch, tip-to-tip pinch) and global grip strength, utilizing graded putty, hand dynamometers, and functional task simulation. The thermoplastic splint is gradually weaned, initially transitioning to nighttime use only, and eventually discontinued entirely by week 10. Return to heavy manual labor, construction trades, or high-impact contact sports is typically restricted until 10 to 12 weeks postoperatively. This extended timeframe ensures complete, solid consolidation of the fracture and the full biological maturation of the capsuloligamentous repair, minimizing the risk of late displacement or catastrophic re-injury.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative management for Bennett fractures is deeply rooted in a rich history of landmark orthopedic literature. Edward Hallaran Bennett's original 1882 treatise laid the foundational anatomical understanding of the fracture-dislocation, recognizing the critical role of the intact volar-ulnar fragment. However, it was the pioneering work of Wagner in the mid-20th century that revolutionized treatment by introducing the technique of closed reduction and percutaneous pinning. Wagner's technique elegantly addressed the dynamic deforming forces, demonstrating that anatomical reduction could be maintained without the morbidity of an open capsulotomy in acute cases.
Modern biomechanical literature has heavily focused on the consequences of articular incongruity. Landmark cadaveric studies by Lutz et al. and Oosterbosch et al. utilized pressure-sensitive film to map the contact stresses across the trapeziometacarpal joint following simulated Bennett fractures. Their findings definitively proved that even minor articular step-offs (greater than 2 mm) drastically decrease the contact area and exponentially increase peak articular pressures. This biomechanical data forms the absolute basis for the modern clinical guideline: any articular displacement exceeding 2 mm is an absolute indication for operative reduction to prevent the rapid onset of post-traumatic osteoarthritis.
Long-term clinical outcome studies, such as those published by Livesley and Cannon, have compared the natural history of conservatively managed Bennett fractures against those treated with rigid operative fixation. These retrospective reviews consistently demonstrate that while non-operative management may yield acceptable results in low-demand patients with minimal displacement, operative restoration of the articular surface and joint stability is paramount for young, active patients. Patients treated with exact anatomical reduction (either via CRPP or ORIF) exhibit statistically significant improvements in long-term grip strength, pinch strength, and a marked reduction in the incidence of symptomatic radiographic arthritis at 10-year follow-up. Consequently, the prevailing clinical guidelines strongly advocate for an aggressive surgical approach in the active population, prioritizing absolute joint congruity and rigid stability to preserve the vital function of the thumb CMC joint.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide