Axial Fixation of Calcaneal Fractures: The Essex-Lopresti Technique
Key Takeaway
The Essex-Lopresti axial fixation technique is a minimally invasive approach for displaced tongue-type calcaneal fractures. By utilizing a heavy Steinmann pin to manipulate and elevate the depressed posterior facet, surgeons can restore calcaneal height and morphology while minimizing soft tissue complications. This guide details the precise biomechanical maneuvers, step-by-step surgical execution, and postoperative protocols necessary to achieve optimal functional outcomes in percutaneous calcaneal fracture management.
INTRODUCTION TO AXIAL FIXATION OF CALCANEAL FRACTURES
The management of displaced intra-articular calcaneal fractures remains one of the most challenging domains in orthopedic trauma surgery. Historically, the extensile lateral approach for Open Reduction and Internal Fixation (ORIF) has been the gold standard; however, this approach is fraught with significant wound complications, particularly in patients with compromised soft tissue envelopes, diabetes mellitus, or a history of tobacco use.
To mitigate these devastating soft tissue complications, closed reduction and percutaneous fixation techniques have experienced a major resurgence. The cornerstone of this minimally invasive philosophy is the Essex-Lopresti Axial Fixation Technique. Originally described in 1952, this elegant biomechanical maneuver leverages the unique pathoanatomy of the "tongue-type" calcaneal fracture. By utilizing a heavy Steinmann pin as a joystick, the surgeon can indirectly reduce the posterior facet, restore calcaneal height, and correct varus deformity without violating the fragile lateral soft tissue envelope.
This comprehensive guide details the indications, biomechanical rationale, step-by-step surgical execution, and postoperative rehabilitation protocols for the axial fixation of calcaneal fractures, integrating modern percutaneous advancements and arthroscopic adjuncts.
SURGICAL PATHOANATOMY AND BIOMECHANICS
To successfully execute the Essex-Lopresti maneuver, the surgeon must possess a profound understanding of calcaneal fracture pathoanatomy. Calcaneal fractures are driven by axial loading forces (e.g., falls from a height, motor vehicle collisions) that drive the lateral process of the talus into the calcaneus.
The Primary and Secondary Fracture Lines
- The Primary Fracture Line: An oblique shear fracture that runs from the crucial angle of Gissane plantarly and medially, dividing the calcaneus into an anteromedial fragment (sustentaculum tali, which remains anatomically tethered to the talus via the deltoid and talocalcaneal ligaments) and a posterolateral fragment (the tuberosity).
- The Secondary Fracture Line: The trajectory of this line dictates the fracture pattern:
- Tongue-Type Fracture: The secondary line exits posteriorly through the calcaneal tuberosity. The posterior facet remains attached to the tuberosity fragment. The Achilles tendon inserts onto this fragment, and its unopposed pull causes the anterior aspect of the posterior facet to depress into the cancellous body, while the posterior tuberosity displaces superiorly.
- Joint-Depression Fracture: The secondary line exits just posterior to the posterior facet. The facet is driven deep into the calcaneal body as a free fragment, completely detached from the tuberosity.
Biomechanical Pearl: The Essex-Lopresti maneuver is specifically designed for tongue-type fractures. Because the posterior facet remains attached to the tuberosity, manipulating the tuberosity with a Steinmann pin directly controls and elevates the depressed articular surface. This maneuver is generally ineffective for pure joint-depression fractures, as the tuberosity is disconnected from the impacted articular fragment.
INDICATIONS AND PATIENT SELECTION
Patient selection is paramount. While percutaneous techniques minimize wound complications, they demand rigorous anatomical knowledge to achieve an acceptable articular reduction.
Primary Indications
- Displaced Tongue-Type Fractures: Particularly Sanders Type II fractures where the posterior facet is attached to the tuberosity.
- Compromised Soft Tissue Envelopes: Severe fracture blisters, massive edema, or impending compartment syndrome where an extensile lateral incision is contraindicated.
- High-Risk Patient Profiles: Heavy smokers, poorly controlled diabetics, and patients with peripheral vascular disease.
- Polytrauma Patients: Damage control orthopedics requiring rapid, minimally invasive stabilization.
Contraindications
- Sanders Type III or IV Fractures: Highly comminuted fractures with multiple articular fragments cannot be adequately reduced via closed indirect maneuvers.
- Deeply Impacted Joint-Depression Fractures: If the posterior facet is severely impacted and detached from the tuberosity, a percutaneous pin will not elevate the articular surface.
- Delayed Presentation: Fractures that are more than 10–14 days old become "sticky." Early consolidation of the cancellous bone makes closed manipulation nearly impossible.
Surgical Warning: It is highly recommended to perform this surgery as soon as feasible after the injury. If the fracture becomes "sticky," indirect reduction will fail. The patient must be preoperatively counseled on the potential need to convert to an open procedure if closed reduction is unachievable.
PREOPERATIVE PLANNING
Imaging Modalities
- Standard Radiographs: Lateral, axial (Harris), and anteroposterior (AP) views of the foot. The lateral view assesses Böhler’s angle (normally 20°–40°) and the crucial angle of Gissane (normally 100°–130°).
- Computed Tomography (CT): A non-contrast CT scan with fine cuts (1-2mm) and 3D reconstructions is mandatory. Coronal views evaluate the posterior facet and sustentaculum tali (Sanders classification), while axial views assess the calcaneocuboid joint and lateral wall blowout.
Operating Room Setup
- Anesthesia: General anesthesia or regional anesthesia (spinal/popliteal block) with deep sedation. Complete muscle relaxation is critical to overcome the deforming force of the gastrocnemius-soleus complex.
- Positioning: The patient is placed strictly prone on a radiolucent operating table. Chest rolls and pelvic supports are utilized to ensure adequate ventilation.
- Fluoroscopy: The C-arm is positioned to allow unimpeded orthogonal views (Lateral, Harris axial, and Broden's views).
STEP-BY-STEP SURGICAL TECHNIQUE: ESSEX-LOPRESTI MANEUVER
1. Incision and Pin Trajectory
With the patient prone, the surgical site is prepped and draped in a standard sterile fashion.
* Identify the displaced tuberosity of the calcaneus.
* Make a small stab incision over the posterior aspect of the tuberosity, positioned just lateral to the attachment of the Achilles tendon. This lateralized entry point avoids the sural nerve and the central watershed area of the Achilles.
* Introduce a heavy Steinmann pin (usually 4.0 mm or 5.0 mm) or a Gissane spike into the tongue fragment.
* The trajectory should be longitudinal, angling slightly from posterior to anterior, and directed slightly toward the lateral side to capture the dense bone of the posterior facet fragment.
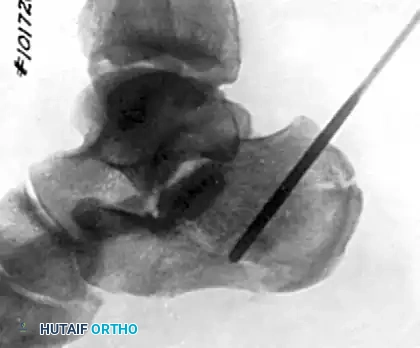
Figure 88-14A: Correct initial positioning and trajectory of the heavy Steinmann pin into the tongue fragment of the calcaneus.
2. The Reduction Maneuver
This is the critical biomechanical step of the procedure. The goal is to disimpact the posterior facet and restore Böhler’s angle.
* Flex the Knee: Flex the patient's knee to 90 degrees. This relaxes the gastrocnemius muscle, significantly reducing the tension on the Achilles tendon and freeing the tuberosity fragment.
* Elevate the Pin: Grasp the protruding Steinmann pin firmly and lift upward (towards the ceiling) until the knee clears the operating table. This powerful levering action elevates the tongue fragment from its depressed position within the calcaneal body.
* Control the Forefoot: With your opposite hand, hold the forefoot at the level of the midtarsal joints. Apply a plantarflexion force to the forefoot.
* Avoid Cavus: It is critical to avoid creating an iatrogenic cavus deformity by hyperflexing the forefoot during this maneuver. The combination of lifting the pin and plantarflexing the forefoot restores the longitudinal arch and calcaneal pitch.
3. Restoring Calcaneal Width and Lateral Wall Decompression
Calcaneal fractures inherently shorten and widen, leading to a "blowout" of the lateral wall. If left unreduced, this lateral bulging will impinge upon the peroneal tendons and the lateral malleolus.
* While maintaining the reduction with the pin, apply aggressive medial-lateral compression.
* Reduce the spreading of the calcaneus by applying sustained, forceful pressure on each side of the bone using the heels of your clasped hands.
* Clinical Imperative: It is absolutely vital to clear the inferior aspect of the lateral malleolus from contact with any bulging lateral wall bone fragments. Failure to do so will result in subfibular impingement, chronic peroneal tenosynovitis, and severe postoperative pain.
Surgical Pearl: Gently rock the calcaneus in a varus-valgus motion at this stage. This micro-motion helps to settle the smaller, comminuted cancellous fragments into their anatomical positions within the restored calcaneal shell.
4. Final Fixation and Radiographic Confirmation
Once the macroscopic morphology (height, width, length, and varus/valgus alignment) is restored, the reduction must be locked in place.
* Advance the heavy Steinmann pin or Gissane spike across the primary fracture line, driving it deep into the intact anterior fragment of the calcaneus (the sustentacular fragment). In some cases of severe instability, the pin may be advanced across the calcaneocuboid joint into the cuboid for temporary stabilization.
* Obtain final fluoroscopic images. A lateral view confirms the restoration of Böhler’s angle and calcaneal height. A Harris axial view confirms the correction of varus deformity and restoration of calcaneal width. Broden's views should be utilized to assess the congruity of the posterior facet.
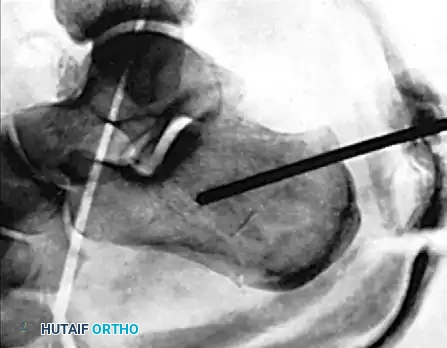
Figure 88-14B: Postoperative lateral radiograph demonstrating the Steinmann pin advanced across the fracture site, maintaining the restored Böhler’s angle. The pin is incorporated into the cast.
ADVANCED PERCUTANEOUS TECHNIQUES & ARTHROSCOPIC ASSISTANCE
While the classic Essex-Lopresti technique relies on fluoroscopy, modern orthopedic trauma surgery frequently integrates Subtalar Arthroscopy to guarantee articular congruity.
Arthroscopic Evaluation
The primary disadvantage of closed reduction is the potential for an inaccurate reduction of the posterior facet. A step-off of more than 1-2 mm in the subtalar joint rapidly leads to post-traumatic osteoarthritis.
* Standard anterolateral and posterolateral arthroscopic portals can be established.
* The arthroscope allows direct, magnified visualization of the posterior facet during the pin elevation maneuver.
* If the articular surface remains incongruent despite the Essex-Lopresti maneuver, a small periarticular elevator can be introduced percutaneously to fine-tune the articular fragments before advancing the axial fixation pin.
Supplemental Screw Fixation
In contemporary practice, the heavy Steinmann pin is often supplemented or replaced by percutaneous cannulated screws (6.5 mm or 7.3 mm). Once the reduction is achieved with the joystick pin, guide wires are passed from the posterior tuberosity into the anterior calcaneus, and fully threaded or partially threaded screws are deployed to provide rigid, compression-free stabilization.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for fracture consolidation with the prevention of soft tissue contractures.
Immediate Postoperative Phase (Weeks 0-6)
- The foot is meticulously padded with cast padding, paying special attention to the heel and bony prominences.
- A bulky, well-molded posterior splint or bivalved cast is applied.
- Pin Management: The protruding portion of the Steinmann pin or Gissane spike is bent and incorporated directly into the splint/cast to prevent migration and pin-tract infections.
- The patient is kept strictly non-weight-bearing. Elevation of the limb above the heart is mandatory for the first 48-72 hours to control edema.
- At 4 to 6 weeks, the initial cast is removed. The Steinmann pin is extracted in the clinic. A new, well-molded short leg cast is applied from the tibial tuberosity to the toes.
Intermediate Phase (Weeks 8-12)
- Radiographs are obtained at 8 to 10 weeks post-reduction.
- The surgeon must look for radiographic evidence of union and the reconstitution of the depressed cancellous bone beneath the elevated articular surface.
- If clinical and radiographic union is confirmed, the patient may begin progressive, partial weight-bearing in a controlled ankle motion (CAM) boot.
- Physical therapy is initiated, focusing on active and active-assisted range of motion of the ankle and subtalar joints.

Figure 88-14C: Lateral radiograph at 1-year follow-up demonstrating excellent consolidation, maintenance of calcaneal height, and a restored Böhler’s angle.

Figure 88-14D: Harris axial radiograph at 1-year follow-up showing restored calcaneal width and neutral heel alignment. The patient successfully returned to heavy manual labor.
COMPLICATIONS AND PITFALLS
Even with minimally invasive techniques, calcaneal fractures carry a high morbidity profile. Surgeons must be vigilant regarding the following complications:
- Inaccurate Articular Reduction: The most common pitfall of closed techniques. Failure to anatomically reduce the posterior facet will inevitably lead to severe subtalar post-traumatic arthritis, often necessitating a secondary subtalar arthrodesis.
- Peroneal Tendon Impingement: If the lateral wall blowout is not adequately compressed during the reduction maneuver, the widened calcaneus will impinge on the fibula. This results in chronic peroneal tenosynovitis, subluxation, and lateral-sided foot pain.
- Sural Nerve Injury: The sural nerve courses along the lateral aspect of the Achilles and lateral calcaneal wall. Percutaneous pin placement and lateral wall compression must be performed with anatomical awareness to avoid entrapment or transection.
- Pin Tract Infection: Protruding pins are susceptible to colonization. Meticulous pin care and incorporation into the cast are required. Deep infections, though rare compared to ORIF, can lead to devastating calcaneal osteomyelitis.
- Loss of Reduction: If the pin is removed prematurely (before 4-6 weeks) or if the patient bears weight non-compliantly, the powerful pull of the Achilles tendon will cause the tongue fragment to displace superiorly, resulting in a loss of Böhler’s angle and a severe flatfoot deformity.
CONCLUSION
The Essex-Lopresti axial fixation technique remains a highly effective, elegant solution for the management of displaced tongue-type calcaneal fractures. By respecting the precarious soft tissue envelope of the hindfoot and utilizing the biomechanical advantages of the intact Achilles-tuberosity-facet complex, orthopedic surgeons can achieve excellent functional outcomes. Mastery of this technique requires precise preoperative planning, meticulous intraoperative fluoroscopic evaluation, and strict adherence to postoperative rehabilitation protocols. When executed correctly, percutaneous axial fixation minimizes morbidity while maximizing the patient's return to pre-injury function.
You Might Also Like
