Comprehensive Management of Charcot Arthropathy: Operative and Nonoperative Strategies

Key Takeaway
Charcot arthropathy management requires a multidisciplinary approach. Nonoperative treatment centers on total contact casting and protected weight-bearing to achieve consolidation. Operative intervention, indicated in approximately 25% of cases, focuses on deformity correction, stabilization, and ulcer prevention. Surgical strategies range from exostectomy and Achilles tendon lengthening to complex midfoot arthrodesis and tibiotalocalcaneal fusion, aiming to create a stable, plantigrade, and braceable foot while avoiding amputation.
Introduction to Charcot Arthropathy Management
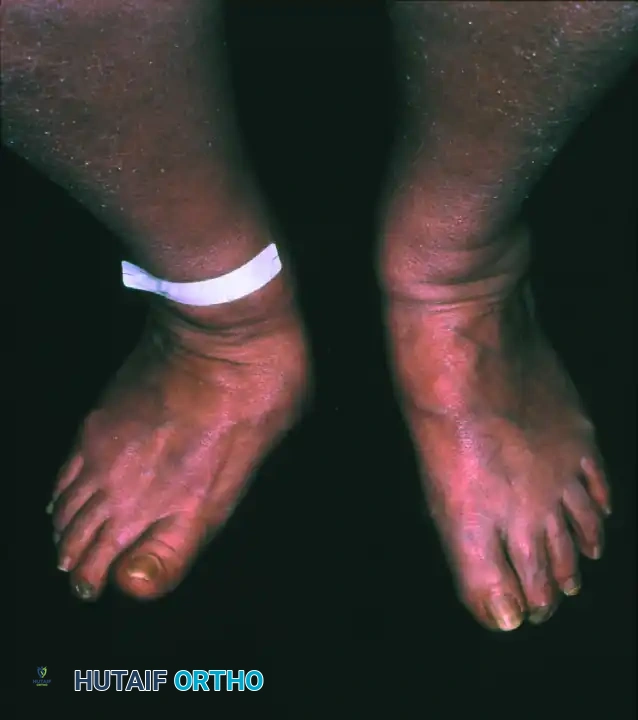
The management of Charcot neuroarthropathy represents one of the most formidable challenges in orthopedic foot and ankle surgery. Characterized by progressive joint destruction, subluxation, fragmentation, and eventual deformity in a neuropathic patient, the condition demands a rigorous, stage-specific therapeutic approach. The overarching goal of treatment—whether nonoperative or operative—is to achieve a stable, plantigrade, and braceable foot, thereby preventing ulceration, deep infection, and the ultimate endpoint of major lower extremity amputation.
Treatment algorithms are heavily dictated by the Eichenholtz stage of the disease (Stage I: Development/Fragmentation; Stage II: Coalescence; Stage III: Consolidation/Reconstruction), the anatomic location of the deformity (Brodsky or Sanders-Frykberg classifications), and the presence of complicating factors such as osteomyelitis or severe soft-tissue compromise.


Nonoperative Management Strategies
Nonoperative management remains the gold standard for acute Charcot arthropathy (Eichenholtz Stage I) and is successful in the majority of patients when initiated promptly. The primary objective during the acute fragmentation phase is to arrest the inflammatory cycle, prevent further mechanical destruction of osteopenic bone, and protect the soft-tissue envelope.
Total Contact Casting (TCC)
Total contact casting with protected weight-bearing is the cornerstone of conservative treatment. The biomechanical principle of the TCC is to redistribute plantar pressures away from bony prominences (such as a collapsed cuboid or medial cuneiform) by transferring load to the lower leg and maximizing the contact area across the entire plantar surface of the foot.
- Application and Monitoring: Initially, the TCC must be changed weekly. This frequent interval is critical to accommodate the rapid decrease in acute edema; a loose-fitting cast allows shear forces that can precipitate iatrogenic ulceration.
- Duration: The course of casting typically spans several months (often 3 to 6 months, or longer). The duration can be minimized by strict patient compliance with protected weight-bearing protocols.
- Progression: Weight-bearing status can be cautiously advanced within the TCC only when clinical signs of instability and inflammation (erythema, calor, edema) subside, and radiographic evidence of bony consolidation (Eichenholtz Stage II/III) becomes apparent.
- Post-Casting Orthotics: Following successful consolidation, patients must be transitioned to lifelong protection using custom orthotics, extra-depth therapeutic footwear, or a Charcot Restraint Orthotic Walker (CROW) boot.
Clinical Pearl: The transition from a TCC to permanent footwear is a high-risk period for disease flare-ups or new ulcerations. If a flare-up occurs, characterized by a return of localized warmth or swelling, immediate reversion to short-term total contact casting is indicated to quiet the inflammatory response.
Pharmacological Interventions
While the mechanical offloading provided by TCC is paramount, pharmacological adjuncts have been investigated to modulate the aggressive osteoclastic activity seen in acute Charcot arthropathy.
* Bisphosphonates: Intravenous or oral bisphosphonates (e.g., pamidronate, alendronate) may reduce bone turnover and have been associated with improvements in pain relief and reductions in local temperature.
* Calcitonin: Intranasal calcitonin has also demonstrated efficacy in decreasing markers of bone turnover.
* Current Consensus: Despite their theoretical benefits, these pharmacological agents are rarely used as standalone treatments and remain off-label adjuncts in standard orthopedic practice.


Operative Management: Principles and Indications
Surgery is required in approximately 25% of patients with Charcot arthropathy. Operative intervention in this population is fundamentally considered limb salvage surgery.
Indications for Surgery
- Severe Instability: Instability that cannot be controlled with immobilization, leading to impending or recurrent ulceration.
- Recurrent Ulceration: Severe, rigid deformity in the consolidated phase (Stage III) that causes recalcitrant plantar ulceration despite optimal orthotic management.
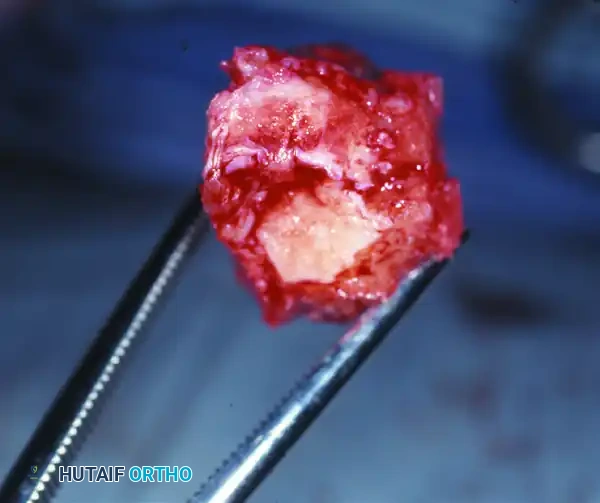
- Deep Infection/Osteomyelitis: Ulcers probing to bone or frank osteomyelitis requiring surgical debridement.
- Acute Dislocation: Select cases of acute, highly unstable fracture-dislocations where conservative management guarantees a non-braceable deformity.
Timing of Surgical Intervention
Historically, surgery was strictly deferred until the coalescence or consolidation phases (Eichenholtz II or III). Operating during the acute fragmentation phase (Stage I) is notoriously difficult due to profound hyperemia, massive edema, and severely osteopenic bone that provides poor purchase for internal fixation.
However, a paradigm shift has occurred. With the advent of stronger fixation techniques ("superconstructs") and advanced external fixation, a more aggressive approach is now possible. Surgery during the fragmentation phase may be necessary and justified for severe, unbraceable instability, acute dislocation with soft-tissue compromise, or concurrent deep infection.
Preoperative Optimization
Before any surgical intervention, a comprehensive medical workup is mandatory.
* Vascular Assessment: A formal vascular surgery consultation is critical. Non-invasive arterial studies (ABI, TBI, Doppler waveforms) must confirm adequate perfusion for wound healing. If ischemia is present, revascularization must precede orthopedic reconstruction.
* Metabolic Control: Optimization of glycemic control (HbA1c), renal function, and nutritional status (albumin, prealbumin) is essential to mitigate the high risk of postoperative complications.



Surgical Procedures and Techniques
The surgical armamentarium for Charcot arthropathy includes exostectomy, open reduction and internal fixation (ORIF), complex arthrodesis, external fixation, and amputation.
Exostectomy (Ostectomy)
Exostectomy is indicated for stable, consolidated deformities (typically midfoot rocker-bottom deformities) where a focal bony prominence causes recurrent ulceration, provided that the removal of this bone will not destabilize the foot.
Surgical Technique:
1. Incision Planning: Incisions should be meticulously planned away from the ulcer bed whenever possible. If the ulcer is excised, the incision may incorporate the ulcer margin, but primary closure without tension is paramount.
2. Soft Tissue Handling: The incision must be full-thickness straight down to the bone. Undermining of the superficial soft tissue must be strictly avoided to preserve the fragile vascular supply to the skin flaps.
3. Bone Resection: The bony prominence (often the plantar aspect of the medial cuneiform or cuboid) is exposed circumferentially. Appropriate removal of bone is performed using an oscillating saw or osteotomes.
4. Tendon Management: Important tendinous attachments (e.g., tibialis anterior or peroneus longus) must be protected or reattached using suture anchors if their insertion is compromised during resection.
5. Equinus Correction: An Achilles tendon lengthening (ATL) or gastrocnemius recession is almost always necessary, as equinus contracture is a primary driver of forefoot and midfoot plantar pressures.
6. Closure: The wound is closed with large, non-absorbable sutures in a single layer, ensuring the obliteration of any dead space.






Surgical Warning: Performing an exostectomy on a foot that is not fully consolidated (still in Eichenholtz Stage I or early II) can precipitate catastrophic destabilization of the midfoot, leading to rapid collapse and failure.
Midfoot and Hindfoot Arthrodesis
Arthrodesis is indicated for severe deformity correction and instability. Because of the osteopenic nature of Charcot bone, poor healing potential, and patient non-compliance with weight-bearing restrictions, standard orthopedic fixation is often insufficient.
Principles of Charcot "Superconstructs":
* Fusion must extend beyond the zone of injury to include normal, healthy bone.
* Bone resection must be adequate to correct the deformity without placing the soft-tissue envelope under tension.
* The strongest possible fixation devices must be utilized.
* Hardware should be applied to the tension side of the deformity to maximize biomechanical stability.
Midfoot Arthrodesis (Type 1 Charcot):
* Deformity Correction: Resection of biplanar wedges of bone is often necessary to restore a plantigrade alignment. Bone grafting (autograft, allograft, or bone marrow aspirate concentrate) may be required to fill structural gaps.
* Fixation Strategy: A combination of robust plates and screws is utilized. Placing a plate on the plantar surface of the midfoot bones takes advantage of the tension band principle, providing vastly superior biomechanical stability against the deforming forces of weight-bearing.
* Beaming: Internal fixation frequently includes "beaming" the medial and lateral columns. A medial column screw (typically an 8.0-mm or 7.3-mm solid or cannulated screw) is driven from the posterior aspect of the talus, across the navicular and cuneiform, and into the first metatarsal.
* Adjuncts: Platelet-rich concentrate and bone marrow aspirate are increasingly used to augment the fusion mass.
Hindfoot Arthrodesis (Type 2 Charcot):
* Triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is the workhorse procedure.
* Large diameter screws (6.5 to 7.3 mm) are mandatory for adequate purchase in the hindfoot.
Ankle Charcot and Tibiotalocalcaneal (TTC) Arthrodesis
Charcot arthropathy of the ankle is highly unstable and rapidly destructive, often leading to a non-braceable varus or valgus collapse.
* TTC Fusion: Tibiotalocalcaneal arthrodesis utilizing a retrograde intramedullary nail is the procedure of choice to control severe instability. The IM nail provides load-sharing biomechanics superior to plate fixation in this setting.
* Talectomy: In cases of severe talar avascular necrosis, fragmentation, or profound deformity, a primary talectomy may be required prior to arthrodesis (tibiocalcaneal fusion). However, it must be noted that if talectomy is required, the postoperative complication rate, including limb length discrepancy and nonunion, is significantly higher.
External Fixation Techniques
For patients with severe midfoot or ankle Charcot arthropathy complicated by active osteomyelitis or massive soft-tissue defects, internal fixation is contraindicated.
* Hybrid/Circular External Fixation: Thin-wire circular fixators (e.g., Ilizarov frames) are invaluable for limb salvage in these poor surgical candidates.
* Technique: Infected and nonviable tissue is aggressively debrided. The joints are prepared for arthrodesis, and the frame is applied to compress the fusion sites and stabilize the limb.
* Wound Management: Open wounds can be managed concurrently with negative pressure wound therapy (NPWT) through the frame, often avoiding the need for complex free flap coverage. Frames are typically maintained for 8 to 12 weeks, followed by transition to total contact casting.
Amputation: The Last Resort
Amputation remains a necessary last resort. It is indicated in the presence of:
1. Overwhelming, life-threatening severe infection (e.g., ascending gas gangrene or necrotizing fasciitis).
2. Severe, unbraceable instability that has failed multiple reconstructive attempts.
3. Massive loss of bone stock that precludes any form of adequate fixation or functional reconstruction.


Pitfall: Delaying amputation in a patient with profound systemic sepsis or unsalvageable vascular ischemia in a futile attempt at limb salvage significantly increases mortality risk.
Postoperative Protocols and Complication Management
The postoperative management of the Charcot patient is as critical as the surgical execution.
- Immobilization: Postoperative immobilization must be significantly longer than in non-neuropathic patients. A minimum of 3 months of strict non-weight-bearing is standard, often extending to 6 months depending on radiographic progression.
- Nonunion: There is a notoriously high nonunion rate for arthrodesis in patients with Charcot arthropathy. However, due to the underlying sensory neuropathy, these nonunions are frequently asymptomatic. If clinical stability is maintained and the foot remains plantigrade, a stable fibrous nonunion may not require revision surgery. The adjunctive use of external bone stimulators can be helpful in promoting consolidation.
- Long-term Surveillance: Continued, lifelong vigilance for ulcers must be maintained. Residual deformity or minor bony prominences keep the overlying skin at perpetual risk for breakdown. Constant upkeep, modification, and compliance with appropriate custom orthotics and bracing are mandatory to ensure long-term limb survival.
You Might Also Like


