Comprehensive Surgical Management of Arthritic Hand Disorders: Osteoarthritis, Rheumatoid, and Psoriatic Pathologies

Key Takeaway
Osteoarthritis is the most prevalent arthritic hand disorder, frequently affecting the trapeziometacarpal and interphalangeal joints. Surgical management requires a deep understanding of joint biomechanics, ligamentous integrity, and progressive deformity patterns. This guide details the pathophysiology, radiographic hallmarks, and step-by-step operative interventions for osteoarthritis, rheumatoid arthritis, and psoriatic arthritis of the hand, providing orthopedic surgeons with evidence-based protocols for arthroplasty, arthrodesis, and soft-tissue reconstruction to restore optimal hand function.
OSTEOARTHRITIS OF THE HAND
Osteoarthritis (OA) represents the most common arthritic disorder affecting the hand and wrist. The condition may present unilaterally, but it occurs with equal frequency in the minor (non-dominant) hand as in the dominant hand, suggesting a strong genetic and systemic biomechanical predisposition rather than pure mechanical wear-and-tear. While OA can occasionally be associated with tendon ruptures and stenosing tenosynovitis (triggering of digits), these soft-tissue complications are markedly less frequent than in rheumatoid arthritis.
The trapeziometacarpal (carpometacarpal or CMC) joint of the thumb is the most frequently surgically treated osteoarthritic joint in the upper extremity. It predominantly affects postmenopausal women and often presents as isolated single-joint involvement before progressing to pan-trapezial disease.
Clinical and Radiographic Presentation
Osteoarthritic degeneration is characterized by progressive cartilage fragmentation, subchondral sclerosis, and marginal osteophyte formation. These osteophytes present clinically as palpable, often painful nodules at the interphalangeal joints:
* Heberden Nodes: Osteophytic outgrowths at the distal interphalangeal (DIP) joints.
* Bouchard Nodes: Osteophytic outgrowths at the proximal interphalangeal (PIP) joints.
Mucoid cysts (ganglion cysts arising from the arthritic joint) frequently form at the dorsal joint margins of the DIP joint, often causing secondary nail bed deformities due to pressure on the germinal matrix. Radiographically, spur formation, joint space narrowing, and subchondral cysts are hallmarks. Unlike rheumatoid disease, limited motion and angular deformity occur without frank multidirectional dislocation, though dorsal subluxation of the distal phalanx is common.
FIGURE 73-4 Osteoarthritic hands with Heberden (distal interphalangeal) and Bouchard (proximal interphalangeal) nodes on both index fingers and thumbs. Note angular changes at distal joints as a result of loss of joint cartilage and instability.
Surgical Management: Trapeziometacarpal Arthroplasty
When conservative measures (splinting, NSAIDs, corticosteroid injections) fail, surgical intervention is indicated. The Ligament Reconstruction and Tendon Interposition (LRTI) utilizing the flexor carpi radialis (FCR) is a gold-standard procedure for Eaton-Littler Stage III and IV CMC osteoarthritis.
Surgical Steps for LRTI:
1. Positioning and Approach: The patient is positioned supine with the arm on a hand table. A regional block or general anesthesia is utilized with an upper arm tourniquet. A Wagner or modified dorsal-radial incision is made over the CMC joint.
2. Nerve Protection: Branches of the superficial radial nerve and lateral antebrachial cutaneous nerve must be meticulously identified and retracted.
3. Trapeziectomy: The capsule is incised longitudinally. The trapezium is fragmented using an osteotome or rongeur and excised piecemeal to avoid injury to the underlying FCR tendon.
4. Tendon Harvest: The FCR tendon is harvested through step-ladder incisions in the volar forearm, leaving its distal insertion at the base of the second metacarpal intact.
5. Ligament Reconstruction: A drill hole is created in the dorsal-radial base of the first metacarpal. The FCR tendon is passed through this tunnel from volar to dorsal, tensioned to reduce the metacarpal base, and sutured to the periosteum to reconstruct the volar beak ligament.
6. Interposition: The remaining FCR tendon is folded into an "anchovy" and sutured into the trapeziectomy void to prevent proximal migration of the first metacarpal.
7. Closure and Postoperative Protocol: The capsule is repaired, and the thumb is immobilized in a thumb spica cast for 4 weeks, followed by progressive range-of-motion (ROM) exercises under the guidance of a certified hand therapist.
Surgical Warning: Failure to adequately clear the medial osteophytes of the trapezium can lead to impingement against the index metacarpal, resulting in persistent postoperative pain. Ensure complete pan-trapezial clearance.
RHEUMATOID ARTHRITIS: BIOMECHANICS AND DEFORMITY
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by aggressive synovial hypertrophy (pannus). This erosive synovitis destroys articular cartilage, attenuates capsuloligamentous structures, and infiltrates tendon sheaths, leading to profound biomechanical imbalances and characteristic hand deformities.
Thumb Deformities in Rheumatoid Arthritis
Rheumatoid thumb deformities are classified by Nalebuff into several types, driven by the primary site of synovitis and subsequent ligamentous failure.
Type I Deformity (Boutonnière):
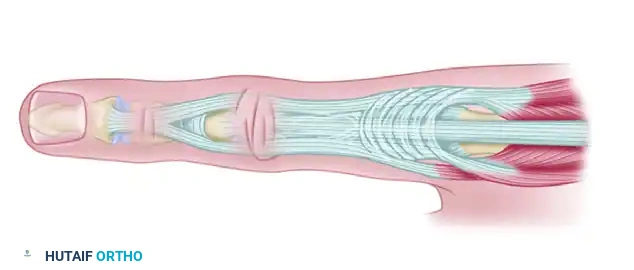
This is the most common RA thumb deformity. Synovitis at the metacarpophalangeal (MCP) joint attenuates the extensor pollicis brevis (EPB) insertion and the dorsal capsule. This allows the proximal phalanx to subluxate volarly, resulting in fixed MCP joint flexion. Consequently, the extensor pollicis longus (EPL) tendon subluxates ulnarly and volarly, increasing its extension moment on the interphalangeal (IP) joint, leading to IP hyperextension.

FIGURE 73-2 Thumb with fixed rheumatoid boutonnière deformity with metacarpophalangeal flexion and interphalangeal hyperextension (type I deformity).
Type III Deformity (Swan-Neck):
When synovitis begins primarily in the thumb CMC joint, the dorsal capsule is destroyed, leading to dorsal and radial subluxation of the metacarpal base. To compensate for the adducted first metacarpal, the patient hyperextends the MCP joint. This leads to a secondary flexion deformity at the IP joint, creating the classic swan-neck appearance.
Gamekeeper Thumb (Rheumatoid Variant):
Synovitic destruction of the capsuloligamentous supports on the ulnar side of the MCP joint results in profound laxity of the ulnar collateral ligament (UCL). This creates severe pinch instability, mimicking a traumatic Gamekeeper's or Skier's thumb.
Clinical Pearl: In RA thumb reconstruction, addressing the primary site of pathology is critical. For a Type I deformity, MCP arthrodesis combined with IP joint release is often the most reliable procedure to restore a stable pinch post.
Finger and Wrist Deformities
Involvement of the finger MCP joints often results in laxity of the capsuloligamentous structures, particularly the volar plate. This leads to hyperextension of the MCP joint and interphalangeal hyperflexion.
In severe, progressive erosive rheumatoid disease (arthritis mutilans), profound osteolysis of the phalanges and metacarpals occurs. The bones telescope into one another, creating redundant, wrinkled skin folds. This end-stage presentation is known as the “main en lorgnette” or opera glass hand.
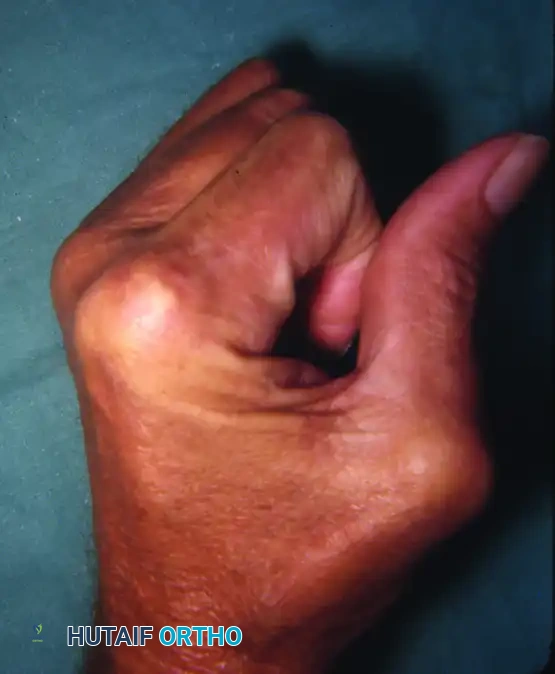
FIGURE 73-3 “Main en lorgnette” (opera glass hand). Late changes in progressive rheumatoid arthritis.
Wrist Pathomechanics:
Rheumatoid synovitis has a devastating effect on the wrist, which serves as the foundation for hand function.
* Carpal Instability: Synovitis disrupts the intercarpal ligaments, most notably the radioscaphocapitate ligament. This leads to rotatory subluxation of the scaphoid and subsequent destructive changes throughout the entire carpus.
* Ulnar Translocation: As the radiocarpal ligaments fail, the natural ulnar slope of the distal radius drives the entire carpus into ulnar translocation.
* Caput Ulnae Syndrome: The stabilizing ligaments of the distal radioulnar joint (DRUJ) are destroyed. This leads to dorsal dislocation of the ulnar head, supination of the carpus, and volar subluxation of the extensor carpi ulnaris (ECU) tendon. The prominent, eroded ulnar head acts as a saw against the extensor tendons, frequently leading to attritional ruptures (Vaughan-Jackson syndrome), beginning with the extensor digiti minimi (EDM) and progressing radially.
Surgical Management of the Rheumatoid Hand
Surgical intervention in RA is prophylactic (tenosynovectomy), reconstructive (tendon transfers, arthroplasty), or salvage (arthrodesis).
- Dorsal Tenosynovectomy and Darrach Procedure: For caput ulnae syndrome with impending tendon rupture, a dorsal approach is utilized. The extensor retinaculum is divided (often preserving a portion to relocate the ECU). A thorough tenosynovectomy is performed. The distal ulna is resected (Darrach procedure) or fused to the radius with a distal ulnar pseudarthrosis (Sauvé-Kapandji procedure) to eliminate the bony prominence.
- MCP Joint Arthroplasty: For severe ulnar drift and volar subluxation of the fingers, silicone implant arthroplasty (Swanson implants) remains a highly effective procedure to restore alignment and functional arc of motion, though grip strength remains limited.
PSORIATIC ARTHRITIS OF THE HAND
Psoriatic arthritis is a distinct inflammatory arthropathy. Approximately 15% to 20% of patients develop the typical psoriatic skin rash after the onset of arthritis, making early diagnosis challenging.
Clinical Presentation
Unlike the symmetrical presentation of rheumatoid arthritis, almost 95% of patients with psoriatic arthritis exhibit asymmetrical peripheral joint involvement.
* Dactylitis: Severe tenosynovitis and joint inflammation lead to fusiform swelling of the entire digit, commonly referred to as a "sausage digit."
* Nail Changes: Uniquely, the nails may separate from the nail bed (onycholysis) and exhibit a white, flaking discoloration near their distal borders. They may also be heavily ridged. Fingernail pitting is the most common manifestation, present in approximately 15% of patients with joint involvement.
Radiographic Hallmarks
Psoriatic arthritis presents with a unique combination of bone proliferation and severe osteolysis:
* Acro-osteolysis: Erosion and resorption of the terminal phalangeal tufts.
* Pencil-in-Cup Deformity: Severe osteolysis tapers the proximal ends of the phalanges and metacarpals (the "pencil"), while the distal articular surface of the adjacent bone undergoes proliferative expansion and cupping (the "cup").
* Joint Tropism: There is a strong predilection for the interphalangeal joints (DIP and PIP), often with relative sparing of the metacarpophalangeal (MCP) joints—a direct contrast to rheumatoid arthritis. Severe destruction frequently leads to spontaneous ankylosis of isolated small joints.
Classification and Surgical Considerations
Kapasi, Ruby, and Calney classified psoriatic arthritis patients into three distinct groups based on the temporal relationship between arthritis onset and skin lesions:
* Type 1 Disease: Early onset of joint involvement with late development of skin lesions. Arthritic involvement in this group is generally mild.
* Type 2 Disease: Late joint involvement following early skin changes. This group typically suffers from more severe, destructive arthritis.
* Type 3 Disease: Simultaneous onset of joint and skin involvement. The severity of arthritic destruction in this cohort is highly unpredictable.
Surgical Management Protocols:
Contractures of the proximal interphalangeal (PIP) joints are common and severely debilitating. Due to the destructive nature of the disease and poor bone stock, these most often require surgical treatment via arthrodesis rather than arthroplasty.
Steps for PIP Arthrodesis:
1. A dorsal longitudinal or V-shaped incision is made over the PIP joint.
2. The extensor mechanism is split longitudinally.
3. The collateral ligaments are excised, and the joint is fully exposed.
4. The articular surfaces are resected using a microsaw or rongeur to create flat, cancellous bone surfaces. The angle of fusion is tailored to the digit (e.g., 25° for the index finger, increasing to 40-50° for the small finger to optimize grip).
5. Fixation is achieved using crossed Kirschner wires, a tension band construct, or a dedicated intramedullary compression screw.
Surgical Warning - Infection Risk: While fusion or arthroplasty may significantly improve hand function, the risk of deep postoperative infection is notably higher following implant arthroplasty in psoriatic patients compared to those with rheumatoid disease, largely due to skin flora colonization in psoriatic plaques.
To mitigate this risk, it is highly recommended to schedule elective surgical procedures during the summer months. During this season, increased ultraviolet light exposure typically causes psoriatic skin lesions to regress, reducing their size and bacterial load, thereby minimizing the risk of perioperative surgical site infections.
You Might Also Like