Comprehensive Surgical Management of Throwing Injuries of the Elbow
Key Takeaway
Throwing injuries of the elbow encompass a complex spectrum of pathology driven by repetitive valgus extension overload. This includes medial ulnar collateral ligament (UCL) insufficiency, lateral radiocapitellar compression, and posterior shear forces leading to posteromedial impingement. Accurate diagnosis relies on dynamic clinical examination and MR arthrography. Surgical management often involves arthroscopic debridement, osteophyte resection, or osteochondral grafting, followed by a meticulously phased rehabilitation protocol to restore the athlete's throwing mechanics and joint stability.
INTRODUCTION TO THROWING INJURIES OF THE ELBOW
The overhead throwing motion places extraordinary biomechanical demands on the elbow joint, generating extreme valgus torque, rapid extension, and immense compressive forces. During the late cocking and early acceleration phases of throwing, the elbow is subjected to a constellation of forces collectively known as Valgus Extension Overload (VEO). This biomechanical cascade results in a predictable triad of pathoanatomy: medial tension, lateral compression, and posterior shear.
Injuries to the elbow from throwing include compression and shear injuries to the radiocapitellar joint on the lateral side of the elbow, incompetence and disruption of the ulnar collateral ligament (UCL) on the medial side, and posteromedial impingement with osteophyte formation, as classically described by Cain et al.
Loose bodies are a frequent concomitant finding and may be located anteriorly or posteriorly. Small loose bodies are particularly prone to hiding along the posterior radiocapitellar joint and the trochlear articulation.
Clinical Evaluation and Imaging
When an overhead athlete presents with elbow pain that does not respond to rest, mechanical modification, and symptomatic treatment, advanced imaging is strictly indicated.
- Magnetic Resonance Imaging (MRI): Standard MRI is highly sensitive for detecting bone marrow edema, stress reactions, and gross ligamentous disruptions.
- MR Arthrography (MRA): The intra-articular injection of a gadolinium contrast agent is the gold standard to fully evaluate partial, undersurface tears of the ulnar collateral ligament (the "T-sign").
- Age-Specific Radiographic Findings:
- Young Athletes (Skeletally Immature): Radiographs of the elbow may reveal osteochondritis dissecans (OCD) of the capitellum, Panner's disease, or physeal nonunion/apophysitis of the olecranon.
- Older Athletes (Skeletally Mature): Stress fractures of the olecranon or mature posteromedial osteophytes may be found on standard radiographs or MRI.
Arthroscopy is definitively indicated when a pathological process is identified on MRI, or when debilitating pain and the inability to throw persist despite exhaustive conservative measures.
Clinical Pearl: Always evaluate the entire kinetic chain in a throwing athlete. Deficits in core stability, hip rotation, or scapular dyskinesia often force the elbow to absorb compensatory loads, leading to primary elbow pathology.
ARTHROSCOPIC EVALUATION OF ULNAR COLLATERAL LIGAMENT FUNCTION
The anterior bundle of the medial ulnar collateral ligament (AMCL) is the primary restraint to valgus stress at the elbow between 20 and 120 degrees of flexion. While gross instability can often be diagnosed clinically via the moving valgus stress test or milking maneuver, subtle or partial tears require dynamic arthroscopic evaluation.
Dynamic Arthroscopic Stress Testing
The functional integrity of the anterior bundle of the UCL can be meticulously evaluated during diagnostic arthroscopy. The procedure is performed with the patient in either the lateral decubitus or prone position, depending on surgeon preference, utilizing standard fluid suspension.
- Portal Placement: The arthroscope is introduced through the standard anterolateral portal to visualize the anterior compartment, specifically focusing on the medial ulnohumeral articulation.
- Positioning for Stress: Traction on the extremity is released. The forearm is fully supinated, and the elbow is flexed to exactly 70 degrees. This position unlocks the olecranon from its fossa and isolates the AMCL.
- Application of Valgus Stress: A controlled valgus stress is applied to the joint by the surgeon or an assistant while directly observing the ulnohumeral articulation.
- Interpretation of Opening:
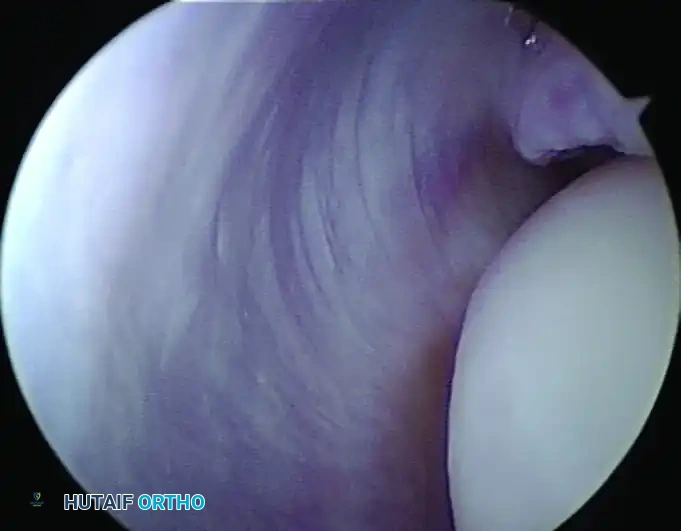
- Normal Anatomy: Normally, the ulnohumeral joint opens less than 1 mm with applied valgus stress.
- Pathologic Instability: An opening of more than 1 to 2 mm, according to the criteria established by Andrews and Baumgarten, indicates functional instability of the UCL.
Arthroscopic examination showing medial instability to stress examination at 70 degrees of flexion. Note the pathologic 2-mm opening between the coronoid and the trochlea, indicative of UCL incompetence.
The Undersurface Tear Pitfall
It is critical to recognize that incomplete undersurface tears of the ulnar collateral ligament, as extensively described by Timmerman and Andrews, may not open to valgus stress during arthroscopy. The superficial fibers remain intact, masking the deep fiber failure. In these cases, localized ligamentous or capsular damage, hemorrhage, or a positive "drive-through" sign in the area of the UCL may be the only visual clues.
Treatment of UCL insufficiency depends heavily on the chronicity of the symptoms, the specific anatomical damage, and the future athletic goals of the patient. Management ranges from biologic augmentation (PRP) to formal UCL reconstruction (Tommy John surgery).
POSTERIOR ELBOW IMPINGEMENT (VALGUS EXTENSION OVERLOAD)
Posterior elbow impingement is the direct result of the posterior shear forces generated during the deceleration phase of throwing. The olecranon tip is forcefully wedged into the posteromedial olecranon fossa, leading to chondromalacia, loose body formation, and the development of posteromedial osteophytes.
Arthroscopic Management of Posteromedial Osteophytes
When a radiograph or MRI demonstrates a posteromedial osteophyte causing mechanical impingement, arthroscopic removal is highly effective.
- Diagnostic Sweep: Careful, full evaluation of the anterior and posterior compartments of the elbow is indicated as previously noted, ensuring all loose bodies are identified and extracted.
- Portal Utilization: The posterior compartment is accessed utilizing a posterolateral viewing portal and a direct posterior (or strictly posterior) working portal.
- Osteophyte Resection: A motorized burr is introduced to resect the impinging posteromedial osteophyte.
Surgical Warning: The 3-Millimeter Rule
When resecting the olecranon osteophyte, strict adherence to biomechanical limits is mandatory. Studies by Kamineni et al. have definitively shown that it is safe to remove the osteophyte and no more than 3 mm of native bone at the tip of the olecranon.
The Danger of Over-Resection:
More aggressive removal of the tip of the olecranon destroys the critical bony buttress that resists valgus stress in terminal extension. This iatrogenic alteration results in exponentially increased stress being transferred to the ulnar collateral ligament, creating the potential for catastrophic ligamentous rupture and further instability problems.
MANAGEMENT OF OSTEOCHONDRAL DEFECTS (OCD)
The lateral compression forces inherent in the throwing motion frequently lead to osteochondral lesions of the capitellum, particularly in adolescent athletes whose articular cartilage and subchondral bone are still maturing.
Surgical Strategies for Capitellar OCD
The surgical approach is dictated by the size, stability, and grade of the lesion.
- Debridement and Microfracture: For smaller, contained lesions (Grade I or II) where the subchondral bone plate is intact, arthroscopic debridement of unstable cartilage followed by microfracture of the base stimulates fibrocartilage healing.
- Osteochondral Autograft Transfer System (OATS): In cases presenting with a wide osteochondral defect, microfracture is insufficient, as only part of the articular surface can be restored with this technique. For large, unstable Grade III lesions, appropriate osteochondral grafts (typically harvested from the non-weight-bearing periphery of the ipsilateral knee) are transferred for the purpose of stabilizing the lesion and restoring the hyaline cartilage contour of the radiocapitellar joint.
POSTEROLATERAL SYNOVIAL PLICA SYNDROME
Posterolateral elbow pain in the throwing athlete is not exclusively caused by osseous or cartilaginous pathology. Persistent pain, catching, and a mechanical "popping" sensation with terminal extension may be caused by osteochondritis dissecans, radiocapitellar chondromalacia, or synovial plica syndrome.
The radiocapitellar plica is a normal anatomic meniscus-like fold of synovium. However, repetitive microtrauma from throwing can cause this plica to become fibrotic, hypertrophic, and inflamed. As the elbow extends, the thickened plica snaps over the radial head, causing localized pain and mechanical symptoms.
If conservative management fails, arthroscopic excision of the hypertrophic plica using a motorized shaver or radiofrequency wand through the anterolateral and direct lateral portals yields excellent clinical outcomes, provided that concomitant lateral compartment pathology (such as OCD) has been ruled out or addressed.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The postoperative rehabilitation following arthroscopic intervention for throwing injuries must be meticulously phased to protect healing tissues while preventing arthrofibrosis. The following protocol applies to isolated arthroscopic debridement, osteophyte excision, and loose body removal (excluding formal UCL reconstruction or large OATS procedures, which require more conservative timelines).
Phase I: Immediate Postoperative (Weeks 0-2)
- After surgery, a well-padded posterior cast or rigid soft splint is applied with the elbow at 90 degrees of flexion.
- The splint is worn continuously for 2 weeks to allow for acute soft tissue healing and to minimize hemarthrosis.
- Active range of motion (ROM) of the wrist, hand, and shoulder is encouraged immediately to maintain distal perfusion and proximal muscle tone.
Phase II: Intermediate ROM and Strengthening (Weeks 3-8)
- Range-of-motion exercises for the elbow are formally started at 3 weeks.
- Emphasis is placed on restoring full terminal extension, which is often the most difficult arc of motion to regain following posterior compartment surgery.
- Submaximal isometric strengthening of the biceps, triceps, and forearm musculature is initiated.
Phase III: Return to Throwing Progression (Months 2-6)
- 2 Months Postoperatively: Patients are allowed to begin an interval throwing program, starting strictly with underhand tossing at short distances (30-45 feet).
- 3 Months Postoperatively: Gentle overhand throwing is allowed, focusing on proper mechanics rather than velocity. The athlete must remain pain-free during this phase.
- 6 Months Postoperatively: Full throwing from the mound at maximum velocity is permitted, provided the athlete has regained full, painless ROM, symmetric strength, and demonstrates flawless kinetic chain mechanics.
You Might Also Like


