Masterclass in Complex Elbow Trauma: Radial Head and Olecranon Fracture-Dislocations

Key Takeaway
The management of radial head and olecranon fractures associated with elbow dislocations requires a profound understanding of elbow biomechanics. This guide details evidence-based surgical protocols, including radial head arthroplasty, coronoid reconstruction, and advanced plate-and-screw fixation for complex ulnohumeral instability. Emphasizing anatomical restoration and early mobilization, these techniques are critical for mitigating post-traumatic stiffness and achieving optimal functional outcomes in complex elbow trauma.
RADIAL HEAD AND NECK FRACTURES ASSOCIATED WITH ELBOW DISLOCATION
The management of radial head and neck fractures in the setting of an acute elbow dislocation remains one of the most challenging paradigms in orthopedic traumatology. The radial head is a critical secondary stabilizer of the elbow joint, functioning synergistically with the coronoid process to resist posterior translation and valgus stress. When the primary ligamentous restraints (the medial and lateral collateral ligaments) are disrupted during a dislocation, the osseous architecture of the radial head becomes the primary buttress against joint subluxation.
Biomechanics and Surgical Decision-Making
Treatment of these complex injuries is historically controversial, but modern biomechanical understanding dictates a strict adherence to restoring joint stability. Open Reduction and Internal Fixation (ORIF) of radial head fractures is always preferable to excision if the radial head is anatomically salvageable (typically defined as fewer than three articular fragments without severe metaphyseal comminution).
If the radial head is deemed unsalvageable and must be excised, the surgeon must acutely address the resulting valgus and posterolateral rotatory instability. In this scenario, the medial collateral ligament (MCL) and the flexor-pronator mass must be meticulously repaired.
Surgical Pearl: The "Back-Table" Reconstruction
If radial head excision is necessary, the excised fragments must be reconstructed on the sterile back table. This is a critical step to ensure that no osteochondral fragments are retained within the joint space, which could lead to mechanical blocking, third-body wear, or post-traumatic osteoarthritis.
Historically, Broberg and Morrey recommended early, complete excision of the radial head for type III (comminuted) fractures, followed by immobilization for no longer than 4 weeks. However, in the setting of a concomitant elbow dislocation, simple excision often leads to catastrophic instability. Today, the use of a metallic radial head implant (arthroplasty) is strongly considered—and often mandated—if instability persists after the MCL and flexor-pronator mass have been repaired. The prosthesis acts as a crucial temporary or permanent spacer to maintain the lateral column length and provide a valgus buttress.
Postoperative Protocol for Radial Head Injuries
The ultimate goal of surgical intervention is a concentrically reduced, stable elbow. If necessary, all capsuloligamentous structures should be repaired to achieve this. Postoperatively, if residual instability is a concern, the elbow should be immobilized in 90 degrees or more of flexion for 3 to 4 weeks. The patient must be followed closely with serial radiographs to monitor for insidious redislocation or subluxation.
FRACTURES AND FRACTURE-DISLOCATIONS OF THE OLECRANON
Olecranon fractures disrupt the extensor mechanism of the elbow and compromise the primary ulnohumeral articulation. These injuries occur via two primary mechanisms:
1. Direct Trauma: A direct blow or fall onto the tip of the flexed elbow, typically resulting in comminuted fracture patterns.
2. Indirect Trauma: A fall onto a partially flexed elbow where the massive eccentric contraction of the triceps muscle avulses the olecranon, often resulting in transverse or oblique fracture patterns.
The Schatzker Classification
Schatzker classified olecranon fractures based on the fracture pattern and the mechanical considerations required for internal fixation. Understanding this classification is paramount for selecting the appropriate osteosynthesis construct.
Transverse Fracture Pattern:
Transverse-Impacted Fracture Pattern:

Oblique Fracture Pattern:

Comminuted Fracture Pattern:
Oblique-Distal Fracture Pattern:
Fracture-Dislocation Pattern:
Tension Band Wiring: Historical Context and Pitfalls
Historically, the tension band wiring technique was the workhorse for simple, transverse olecranon fractures. The biomechanical principle relies on converting the tensile forces of the triceps on the posterior cortex into compressive forces across the articular surface at the sigmoid notch.
However, this procedure is fraught with complications. The most common complication is symptomatic hardware (prominent K-wires backing out), which requires a secondary operation for removal in up to 80% of patients. Furthermore, poorer outcomes have been consistently noted in patients with concomitant elbow instability, coronoid fractures, or radial head fractures.
Surgical Warning: Neurovascular Injury
When utilizing Kirschner wires to anchor the tension band, there is a distinct risk of injury to the neurovascular structures in the anterior forearm if the wires overpenetrate the anterior ulnar cortex. Transcortical placement (engaging the anterior cortex) rather than purely intramedullary placement increases stability but requires precise depth control.
Due to the high complication and reoperation rates, tension band wiring is now infrequently used for displaced olecranon fractures, reserved primarily for patients with exceptionally poor soft tissue envelopes where hardware prominence must be minimized.
Plate-and-Screw Fixation: The Modern Gold Standard
Plate fixation is the contemporary treatment of choice, offering superior biomechanical stability. It is specifically indicated for fractures with comminution, distal extensions (Monteggia variants), and complex fracture-dislocations.
Typically applied in a neutralization mode, the plating technique allows for independent lag screw fixation of the olecranon and/or coronoid fragments to anatomically reconstruct the proximal ulna. The plate then spans the construct, providing the rigid stability necessary to initiate an early range-of-motion program.
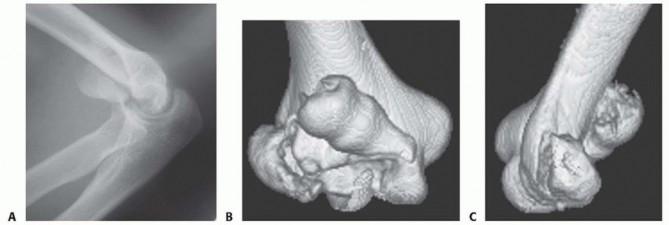
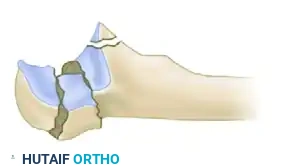
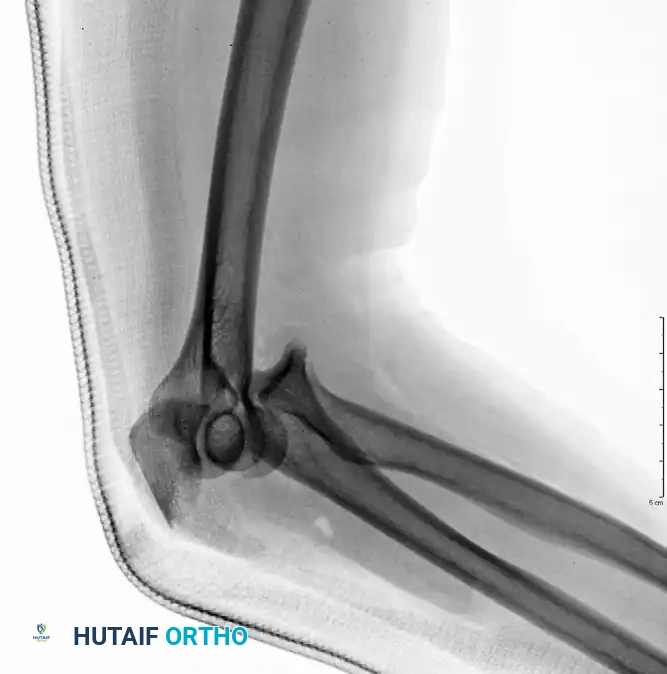
Preoperative Injury - Olecranon Fracture-Dislocation:

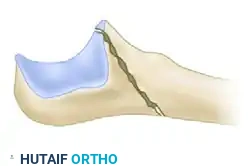
Fixation with Lag Screw and Plate (AP View):

Fixation with Lag Screw and Plate (Lateral View):
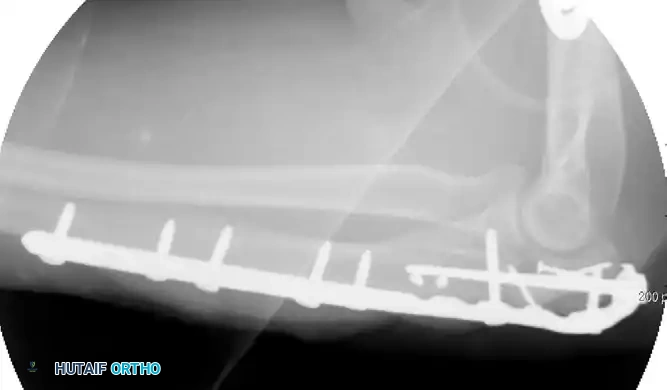
While early literature cited symptomatic hardware as a disadvantage of plating, modern implant designs have largely mitigated this issue. Newer precontoured plates are anatomically designed, lower in profile, and feature locking screw capabilities. They can also be contoured to match the proximal ulnar bow for extended fractures. Biomechanical testing confirms that these modern plates provide significantly greater compression than tension bands, yielding favorable results in over 80% of patients.
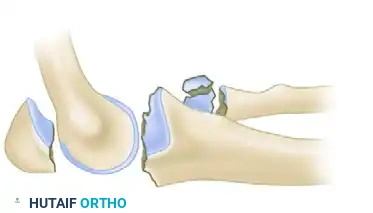
Complex Olecranon Fracture-Dislocation (Injury):
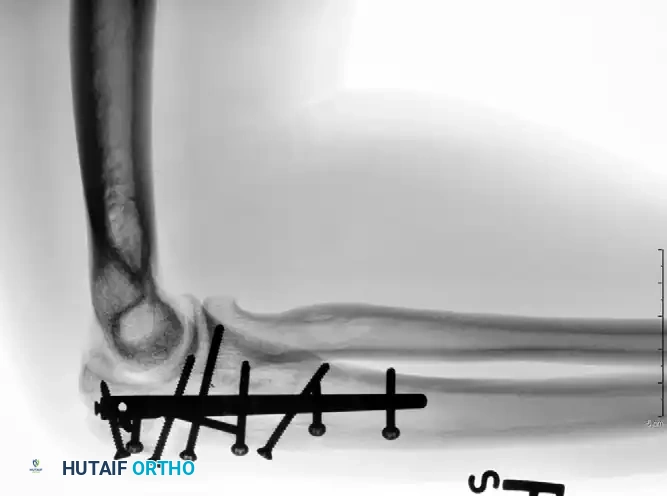
Fixation with Low-Profile Plate (AP View):

Fixation with Low-Profile Plate (Lateral View):

Clinical Pitfall: Wound Complications
Wound breakdown remains the most significant concern with plate fixation. The proximal ulna possesses a notoriously thin, compromised soft tissue envelope. Furthermore, the posterior skin is placed under immense tension during elbow flexion. Meticulous soft tissue handling and thick fasciocutaneous flaps are mandatory.
COMPLEX OLECRANON FRACTURE-DISLOCATIONS
Olecranon fracture-dislocations represent high-energy trauma and are broadly categorized into anterior and posterior dislocations.
Anterior (Transolecranon) Fracture-Dislocations
In an anterior transolecranon fracture-dislocation, the mechanism involves the distal humerus imploding through the olecranon. This results in an anterior ulnohumeral dislocation. Crucially, in a true transolecranon injury, the proximal radioulnar joint (PRUJ) remains anatomically preserved, and the collateral ligaments (MCL and LCL) are typically intact.
These injuries vary in complexity, often presenting with extensive comminution and coronoid involvement. The routine treatment protocol demands anatomical reconstruction of the greater sigmoid notch articular surface followed by rigid plate fixation. The coronoid must be reduced and stabilized with lag screws first, followed by provisional articular reduction, and finally, a robust plate spanning the entire zone of injury.
Preoperative Transolecranon Fracture-Dislocation:

Fixation with Lag Screws and Plate Spanning Entire Injury (AP View):
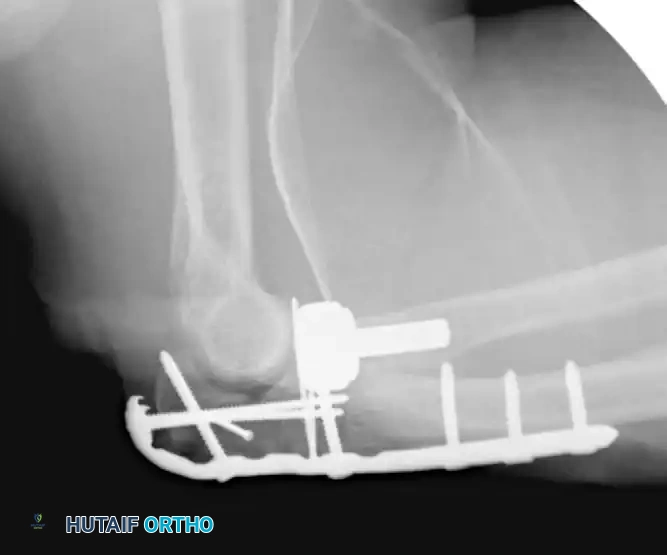
Fixation with Lag Screws and Plate Spanning Entire Injury (Lateral View):

Fixation with Lag Screws and Plate Spanning Entire Injury (Oblique View):

Posterior Fracture-Dislocations (Monteggia Variants)
Posterior dislocations involve both ulnohumeral and radioulnar disruption and are frequently considered variants of Bado type II Monteggia fracture-dislocations. These are highly unstable injuries, often presenting with concomitant coronoid fractures, radial head fractures, and lateral collateral ligament (LCL) avulsions—sharing significant biomechanical overlap with "terrible triad" injuries.
Successful management requires a highly structured, fragment-specific surgical protocol. Beingessner et al. outlined a definitive 6-step approach that yields consistently good outcomes:
- Radial Head Management: Repair or prosthetic replacement of the radial head to restore the anterior/valgus buttress.
- Ulnar Shaft Reduction: Anatomical reduction of the ulnar shaft, specifically addressing the anterior oblique cortical fragment if present.
- Coronoid Stabilization: Reduction and rigid stabilization of the coronoid process using either anterior-to-posterior screws or transosseous sutures.
- Olecranon Fixation: Reduction and fixation of the olecranon process to the ulnar shaft, followed by definitive plate fixation of the ulnar component.
- Ligamentous Repair (Distal): Repair of the osseous ulnar insertions of the medial collateral ligament and/or lateral collateral ligament.
- Ligamentous Repair (Proximal): Repair of the humeral origin of the lateral collateral ligament (usually via suture anchors).
INTRAMEDULLARY NAILING FOR PROXIMAL ULNA FRACTURES
Recently, there has been a resurgence of interest in the use of intramedullary (IM) nails for the treatment of proximal ulna and olecranon fractures. The biomechanical advantage of IM nailing lies in its load-sharing capacity and minimal soft tissue disruption, which is highly advantageous in patients with compromised posterior skin envelopes.
Rodriquez and Eglseder described a hybrid technique combining an intramedullary screw with a low-profile mini-fragment plate on the periphery, yielding results comparable to 3.5-mm limited-contact dynamic compression plates.
More advanced, dedicated implants have since been developed. Nijs et al. reported excellent outcomes using an olecranon osteotomy nail (OleON, Synthes). Furthermore, Edwards et al. demonstrated the efficacy of a multiplanar locking intramedullary nail (OlecraNail, Mylad Orthopaedic Solutions) for the treatment of proximal olecranon fractures, including those presenting with complex, multi-directional instability patterns.
Complex Fracture-Dislocation of the Elbow (Pre-op AP):

Complex Fracture-Dislocation of the Elbow (Pre-op Lateral):

Fixation with Multiplanar Locking Intramedullary Nail (Post-op AP):

Fixation with Multiplanar Locking Intramedullary Nail (Post-op Lateral):
Conclusion and Rehabilitation
The surgical management of radial head and olecranon fracture-dislocations is an exercise in meticulous anatomical restoration. Whether utilizing advanced precontoured plating systems, radial head arthroplasty, or multiplanar intramedullary nails, the ultimate objective remains the same: achieving a construct rigid enough to permit early, active range of motion. Prolonged immobilization beyond 3 to 4 weeks inevitably leads to profound joint stiffness, which is often more debilitating than the initial instability. A carefully supervised rehabilitation protocol, emphasizing early active extension and gravity-assisted flexion while protecting ligamentous repairs, is paramount to achieving an optimal functional outcome.
You Might Also Like