Comprehensive Management of Elbow Instability and Ulnar Collateral Ligament Reconstruction

Key Takeaway
The management of elbow instability requires a nuanced understanding of joint biomechanics and ligamentous anatomy. While stable acute dislocations often respond to early functional rehabilitation, chronic attritional injuries—particularly ulnar collateral ligament insufficiency in overhead athletes—frequently necessitate surgical reconstruction. This guide details evidence-based nonoperative protocols, arthroscopic evaluation techniques, and advanced surgical interventions, including the classic Jobe technique and the modern docking procedure for UCL reconstruction.
INTRODUCTION TO ELBOW INSTABILITY
The elbow is a highly constrained hinge joint relying on a complex interplay of osseous congruity and capsuloligamentous integrity for stability. The primary static stabilizers are the ulnohumeral articulation, the anterior bundle of the medial ulnar collateral ligament (UCL), and the lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL). Disruption of these structures, whether through acute traumatic dislocation or chronic microtraumatic attenuation in overhead athletes, leads to profound functional impairment.
Management algorithms are dictated by the chronicity of the injury, the specific anatomic structures compromised, and the functional demands of the patient. This comprehensive guide delineates the evidence-based protocols for nonoperative management, the role of diagnostic and therapeutic arthroscopy, and the precise surgical techniques required for ligamentous reconstruction.
NONOPERATIVE MANAGEMENT OF ACUTE DISLOCATIONS
Acute complete simple elbow dislocations (those without associated fractures of the radial head or coronoid process) are categorized as either stable or unstable following closed reduction. The cornerstone of nonoperative management is balancing the restoration of joint stability with the prevention of debilitating flexion contractures.
Stable Reductions
For elbows deemed stable through a full arc of motion post-reduction, early active range of motion (ROM) is indicated. Prolonged immobilization in stable joints is strictly contraindicated, as the elbow capsule is highly prone to rapid and severe arthrofibrosis. Patients are typically placed in a sling for comfort for 3 to 5 days, followed by supervised, gravity-assisted active ROM exercises.
Unstable Reductions
For unstable elbows, kinematic bracing is required to protect the healing capsuloligamentous structures while permitting safe arcs of motion. An articulated elbow splint or brace is utilized to control the ROM:
* Week 1: Extension is blocked at 45 degrees.
* Week 2: The extension block is advanced to 30 degrees.
* Week 3 and Beyond: Full motion is gradually permitted as dynamic stability improves.
Clinical Pearl: If a flexion contracture of more than 30 degrees persists after 6 weeks of functional rehabilitation, a dynamic or static progressive extension splint (e.g., turnbuckle orthosis) should be initiated to mechanically creep the anterior capsule and improve terminal extension.
Forearm Positioning Based on Injury Pattern
The position of the forearm during immobilization profoundly affects the tension on the collateral ligaments.
* Medial Disruption (Incomplete Injuries): If the injury pattern predominantly involves disruption of the medial side of the elbow (UCL), the forearm should be placed in supination. Supination tightens the lateral ligamentous complex and the common extensor origin, effectively closing the medial joint space and resting the healing UCL.
* Lateral Disruption: Conversely, lateral injuries (LUCL disruption leading to posterolateral rotatory instability) are treated by placing the forearm in pronation with the elbow flexed to 90 degrees for 1 to 2 weeks. Pronation tensions the medial soft tissues and the flexor-pronator mass, compressing the radiocapitellar joint and stabilizing the lateral side. This is followed by the use of a hinged elbow brace.
DIAGNOSTIC AND THERAPEUTIC ARTHROSCOPY
Arthroscopy of the elbow has evolved into an invaluable adjunct for both diagnosing subtle instability and managing concomitant intra-articular pathology. It is particularly useful in the overhead athlete presenting with medial elbow pain of ambiguous etiology.
Indications and Findings
Arthroscopy can definitively confirm the presence of medial instability, identify and extract loose bodies, and facilitate the resection of posteromedial olecranon osteophytes (valgus extension overload syndrome). Medial instability is frequently associated with secondary intra-articular derangements, including:
* Chondromalacia of the radiocapitellar joint (due to excessive lateral compressive forces during valgus stress).
* Synovitis of the medial capsule.
* Formation of posteromedial olecranon osteophytes (due to abnormal abutment of the olecranon in the olecranon fossa during the acceleration phase of throwing).
Arthroscopic Valgus Stress Test
Andrews et al. described a dynamic valgus stress test performed arthroscopically with the patient under general anesthesia.
1. The arthroscope is introduced via the standard anterolateral portal to visualize the medial ulnohumeral compartment.
2. The elbow is flexed to between 70 and 90 degrees to unlock the olecranon from its fossa, isolating the anterior bundle of the UCL.
3. A valgus stress is manually applied to the elbow.
4. The opening between the medial aspect of the ulna and the trochlea is directly visualized and measured.
Surgical Warning: An opening of more than 1 to 2 mm during the arthroscopic valgus stress test is a definitive indicator of medial ligamentous incompetence. This "drive-through" sign confirms the need for surgical stabilization if the patient is symptomatic.
SURGICAL TREATMENT OF ELBOW INSTABILITY
Acute Simple Dislocations
Surgical intervention is generally not indicated for acute simple elbow dislocations unless the dislocation is irreducible or instability recurs despite appropriate immobilization and bracing. In such refractory cases, meticulous clinical examination and MRI evaluation are mandatory to delineate the soft tissue and bony anatomy, identifying all compromised structures.
Surgical intervention must be directed toward the side of greatest instability—most commonly the lateral side (LUCL). In cases of global, multidirectional instability, both the lateral and medial sides may require simultaneous repair. The surgical objectives include:
* Direct repair of the torn capsule.
* Primary ligamentous reconstruction or repair using suture anchors.
* Reattachment of the avulsed common extensor or flexor-pronator tendon origins.
Chronic Attritional Ligamentous Disruption
Surgical reconstruction for chronic, attritional ligamentous disruption—particularly of the UCL in overhead athletes—is vastly more common than primary reconstruction for acute dislocations.
Indications for UCL Reconstruction
- An acute, complete rupture of the UCL in a competitive throwing athlete who wishes to return to high-level play.
- Chronic medial elbow pain or symptomatic valgus instability that fails to improve after a minimum of 4 to 6 weeks of strictly supervised conservative treatment.
Conservative Management Protocol
Before considering reconstruction, a robust conservative trial is mandatory. This consists of:
* Relative rest with cessation of throwing.
* Forearm and shoulder girdle strengthening exercises.
* Maintenance of core, lower extremity, and cardiovascular conditioning (the "kinetic chain").
* Routine use of NSAIDs and modalities.
* Initiation of a structured, short-toss interval throwing program at 4 to 6 weeks.
Recurrence of medial pain that prevents the skillful progression of the monitored throwing program is the hallmark of persistent ligamentous incompetence and an indication for surgery.
FIGURE 47-52: Anteroposterior radiograph showing calcification of a chronically deficient ulnar collateral ligament, a common finding in chronic valgus extension overload.
ULNAR COLLATERAL LIGAMENT (UCL) RECONSTRUCTION
Preoperative Planning and Graft Selection
The gold standard for UCL reconstruction utilizes an autogenous tendon graft. The palmaris longus (PL) tendon is the graft of choice due to its ideal length, diameter, and minimal donor site morbidity.
Surgical Pitfall: The palmaris longus tendon is congenitally absent in 15% to 20% of the population. Furthermore, when present unilaterally, it may possess an anomalous distal muscle belly, rendering the tendinous portion too short for a standard figure-of-eight reconstruction. The surgeon must routinely assess for PL presence preoperatively and always consent the patient for a gracilis tendon or plantaris tendon harvest as a backup.
The Classic Jobe Technique (1986)
Frank Jobe originally described the revolutionary technique for UCL reconstruction in 1986.
1. Approach: A medial incision is made, and the flexor-pronator mass is completely detached from the medial epicondyle to expose the native, attenuated UCL.
2. Tunnel Preparation: Open-ended bone tunnels are drilled in the sublime tubercle of the ulna and the medial humeral epicondyle.
3. Graft Passage: The palmaris longus graft is passed through the tunnels in a figure-of-eight configuration to recreate the anterior bundle of the UCL.
4. Nerve Management: The ulnar nerve is routinely transposed anteriorly and placed in a submuscular bed beneath the flexor mass to prevent postoperative neuritis.
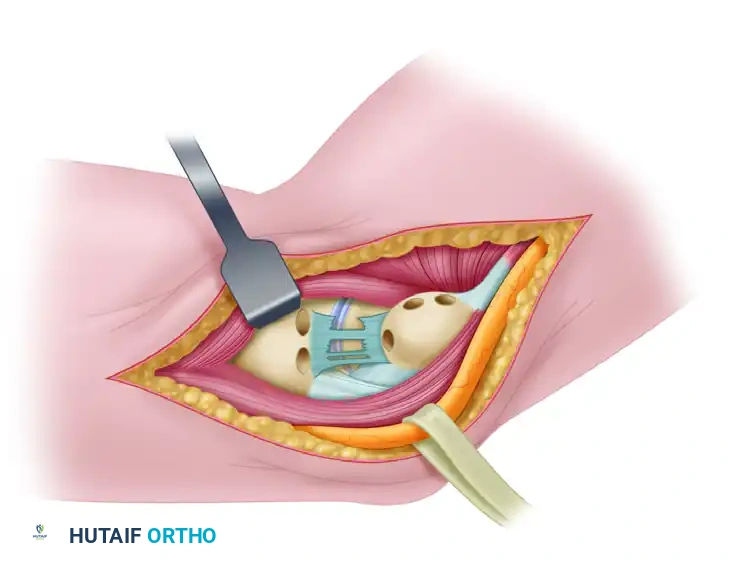
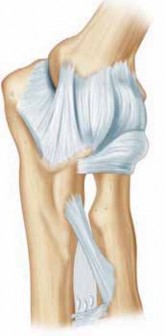
FIGURE 47-51: Jobe ulnar collateral ligament reconstruction. Medial aspect of right elbow before reconstruction showing remnant of ulnar collateral ligament and proper placement of bone tunnels in ulna and medial humeral condyle. Holes are drilled in ulna 5 mm from joint. Ulnar tunnel and closed-end tunnel in medial epicondyle are centered over bony attachments of ligament.
Modifications to the Jobe Technique
Over the decades, several critical modifications have been developed to minimize surgical morbidity and improve biomechanical outcomes.
Jobe's Later Modifications
Jobe subsequently modified his own technique to minimize trauma to the flexor-pronator mass. Instead of detaching the muscle, a muscle-splitting approach through the common flexor mass is utilized. Additionally, a closed-ended tunnel is used in the medial epicondyle, and the ulnar nerve is only transposed if heavy perineural scar tissue is encountered or if the patient has preoperative ulnar neuritis.
The Andrews Modification
Andrews et al. further refined the approach by dissecting the muscle belly of the flexor carpi ulnaris (FCU) and retracting it anteriorly to expose the UCL, entirely avoiding detachment from the epicondyle. They maintained the use of open-ended tunnels but emphasized suturing the graft securely to the posterior epicondyle and imbricating the native collateral ligament over the graft. The ulnar nerve is transposed anteriorly and secured with fascial slings (subcutaneous transposition).
Outcomes using these techniques are excellent; Cain evaluated 743 athletes undergoing UCL reconstruction, noting that 83% returned to the same or a higher level of competition at less than 1 year postoperatively.
The Docking Procedure
The "Docking Procedure" represents a modern evolution in UCL reconstruction, designed to optimize graft tensioning and minimize bone removal. It has demonstrated exceptional clinical success, with reports indicating 39 of 40 elite athletes returning to their previous level of competition.
Key Benefits of the Docking Procedure:
1. Safe Zone Approach: Reconstruction is performed through a longitudinal split in the FCU muscle, minimizing disruption of the dynamic medial stabilizers.
2. Nerve Preservation: Avoidance of obligatory ulnar nerve transfer, reducing the risk of iatrogenic neuropathy.
3. Optimized Humeral Fixation: Placement of the tendon graft into a single, closed-end humeral tunnel (the "docking" site).
4. Reduced Bone Loss: Reduction in the number of humeral tunnels decreases the risk of epicondylar fracture.
5. Simplified Tensioning: The graft is tensioned by pulling the suture limbs through small exit puncture holes in the posterior humerus, allowing precise tensioning over the joint before tying.
Biomechanics of Fixation: Docking vs. Interference Screws
Recent interest has emerged regarding the use of bioabsorbable interference screws for graft fixation in the humeral and ulnar tunnels. However, rigorous biomechanical pull-out studies have consistently demonstrated that the traditional docking technique (suture fixation over a bone bridge) is biomechanically superior to interference screw fixation in cyclic loading and ultimate failure strength.
Clinical Pearl: Due to the documented potential for osteolysis, sterile sinus formation, and bone resorption around poly-L-lactic acid (PLLA) absorbable screws in the medial epicondyle, the use of interference screws for UCL reconstruction is generally not advocated. The docking technique remains the gold standard for reliable, biologic fixation.
POSTOPERATIVE REHABILITATION PROTOCOL
The success of a UCL reconstruction is inextricably linked to strict adherence to a phased rehabilitation protocol.
- Phase I (0-3 Weeks): The elbow is immobilized in a posterior splint at 90 degrees of flexion for 1 week. At week 2, a hinged brace is applied (locked from 30 to 90 degrees). Submaximal isometric exercises for the shoulder and wrist are initiated.
- Phase II (4-8 Weeks): The brace is gradually opened to allow full ROM by week 6. Isotonic strengthening of the flexor-pronator mass and shoulder girdle (especially the rotator cuff and scapular stabilizers) begins.
- Phase III (9-13 Weeks): Advanced strengthening and plyometric exercises are introduced. The athlete begins a two-hand plyometric chest pass and progresses to one-handed throws.
- Phase IV (14+ Weeks): An interval throwing program is initiated, starting with 45-foot flat-ground throws and progressing systematically. Return to competitive pitching typically occurs between 12 and 18 months postoperatively, depending on the athlete's mechanics, strength, and absence of symptoms.
You Might Also Like