Masterclass in Upper Extremity Amputations: Elbow Disarticulation and Transhumeral Techniques
Key Takeaway
Elbow disarticulation offers superior prosthetic suspension and transmits humeral rotation effectively, making it biomechanically preferable to transhumeral amputation. When transhumeral amputation is required, preserving maximal humeral length is critical, though bone sectioning must remain at least 3.8 cm proximal to the joint line to accommodate an internal prosthetic elbow-lock mechanism. This guide details the precise surgical techniques, flap designs, and neurovascular management for optimal functional outcomes.
INTRODUCTION TO UPPER EXTREMITY AMPUTATIONS
Amputations of the upper extremity, particularly at or proximal to the elbow, represent profound functional and psychological life-altering events for the patient. The primary goal of the orthopedic surgeon is to construct a residual limb that is painless, highly functional, and optimally designed for modern prosthetic interfaces.
Historically, elbow disarticulation was viewed with skepticism due to the bulky nature of the distal humeral condyles, which complicated the fitting of traditional prosthetic sockets. However, with the advent of advanced materials, silicone liners, and modern socket designs, the paradigm has shifted. Today, elbow disarticulation is widely recognized as biomechanically superior to transhumeral (above-elbow) amputations.
This comprehensive guide details the indications, biomechanical rationale, and step-by-step surgical techniques for both elbow disarticulation and transhumeral amputations, providing the practicing consultant and orthopedic fellow with an evidence-based framework for achieving optimal surgical outcomes.
BIOMECHANICS AND PROSTHETIC CONSIDERATIONS
The Superiority of Elbow Disarticulation
The elbow joint provides an exceptional level for amputation due to the unique osteology of the distal humerus. The broad flare of the medial and lateral humeral epicondyles allows the prosthetic socket to achieve a firm, self-suspending grasp.
More importantly, this condylar flare permits the direct transmission of humeral rotation to the prosthesis. In a transhumeral amputation, the cylindrical shape of the residual humeral diaphysis cannot transmit rotational forces effectively, necessitating the inclusion of a prosthetic "elbow turntable" to substitute for internal and external rotation. By preserving the distal humerus, the patient retains a significantly more natural and intuitive control over the terminal device.
Transhumeral Prosthetic Requirements
When an amputation must be performed proximal to the elbow joint (transhumeral), the surgeon must account for the mechanical requirements of the prosthetic elbow joint. A transhumeral prosthesis requires an internal elbow-lock mechanism to stabilize the joint in varying degrees of flexion and extension.
Surgical Warning: The internal elbow-lock mechanism extends approximately 3.8 cm distally from the end of the prosthetic socket. To ensure the prosthetic elbow aligns cosmetically and functionally with the contralateral anatomic elbow, the surgeon must section the humerus at least 3.8 cm proximal to the elbow joint line. Failure to do so results in an asymmetric, elongated prosthetic arm.
ELBOW DISARTICULATION: SURGICAL TECHNIQUE
Indications and Preoperative Planning
Elbow disarticulation is indicated for severe trauma, unsalvageable infections (e.g., necrotizing fasciitis), or malignant tumors of the forearm where adequate oncologic margins can be achieved without sacrificing the distal humerus. Preoperative planning should include a thorough neurovascular assessment and optimization of the patient's nutritional status to ensure flap viability and wound healing.
Patient Positioning and Preparation
The patient is placed in the supine position with the affected arm extended on a radiolucent hand table. A sterile tourniquet is applied high on the brachium. The entire upper extremity is prepped and draped in a standard sterile fashion, allowing free manipulation of the arm during the procedure.
Step-by-Step Surgical Approach (Technique 13-5)
1. Flap Design and Incision
Meticulous flap design is critical to ensure a tension-free closure with the suture line positioned away from weight-bearing or high-friction areas.
* Posterior Flap: Begin proximally at the level of the medial and lateral humeral epicondyles. Extend the incision distally to a point approximately 2.5 cm distal to the tip of the olecranon.
* Anterior Flap: From the epicondyles, extend the anterior flap distally to a point just distal to the insertion of the biceps tendon on the radial tuberosity.
* Note: While equal anterior and posterior flaps are standard, atypical flaps may be fashioned based on the availability of viable soft tissue, particularly in trauma settings.
2. Anterior Dissection and Neurovascular Management
Reflect the skin and fasciocutaneous flaps proximally to the level of the humeral epicondyles. Begin the deep dissection on the medial aspect of the elbow.
* Identify and divide the lacertus fibrosus (bicipital aponeurosis).
* Free the origin of the flexor-pronator muscle mass from the medial humeral epicondyle and reflect it distally. This exposes the primary neurovascular bundle lying medial to the biceps tendon.
* Isolate the brachial artery and venae comitantes proximal to the joint line. Doubly ligate them with non-absorbable sutures (e.g., silk or prolene) and divide them.
3. Nerve Management (Traction Neurectomy)
Proper nerve management is paramount to prevent debilitating symptomatic neuromas.
* Median Nerve: Gently draw the median nerve distally, apply gentle traction, and divide it sharply with a scalpel so that it retracts at least 2.5 cm proximal to the joint line into the deep muscle belly.
* Ulnar Nerve: Identify the ulnar nerve in the cubital tunnel posterior to the medial epicondyle. Free it from its groove, apply traction, and transect it sharply to allow proximal retraction.
* Radial Nerve: Identify the radial nerve in the interval between the brachialis and brachioradialis. Isolate it, draw it distally, and section it far proximally.
Clinical Pearl: Consider Targeted Muscle Reinnervation (TMR) at this stage. Transferring the transected ends of the median, ulnar, and radial nerves into adjacent redundant motor nerve branches (e.g., branches to the brachialis or flexor mass) significantly reduces the incidence of phantom limb pain and symptomatic neuromas.
4. Musculotendinous Detachment and Disarticulation
* Release the insertion of the biceps tendon from the radial tuberosity.
* Release the insertion of the brachialis tendon from the coronoid process of the ulna.
* Approximately 6.3 cm distal to the joint line, divide the extensor musculature arising from the lateral epicondyle transversely. Reflect this muscle mass proximally.
* Divide the posterior fascia and the triceps tendon near its insertion on the tip of the olecranon.
* Incise the anterior joint capsule, divide the collateral ligaments, and complete the disarticulation to remove the forearm.
5. Myodesis, Myoplasty, and Closure
* Articular Surface: Leave the articular cartilage of the distal humerus intact. Stripping the cartilage exposes subchondral bone, which increases the risk of heterotopic ossification and creates a rough surface that may irritate the distal stump.
* Myoplasty: Bring the triceps tendon anteriorly and suture it directly to the tendons of the brachialis and biceps muscles.
* Fashion a thin flap from the extensor muscle mass attached to the lateral epicondyle. Carry this flap medially and suture it to the remnants of the flexor muscles at the medial epicondyle.
* Ensure all bony prominences (epicondyles) are well-padded by passing additional sutures through the periosteum and the muscle flap.
* Insert a closed-suction drain deep to the fascial layer.
* Trim the skin flaps for a snug, tension-free closure. Approximate the edges using interrupted non-absorbable sutures.
TRANSHUMERAL (ARM) AMPUTATIONS
Definition and Levels
Transhumeral amputation is defined as an amputation at any level from the supracondylar region of the humerus distally, to the level of the axillary fold proximally.
* Amputations distal to the supracondylar region (e.g., transcondylar) function prosthetically as elbow disarticulations.
* Amputations proximal to the axillary fold function prosthetically as shoulder disarticulations.
Surgical Principles and Pediatric Considerations
As with all amputations, preserving maximum bone length is the cardinal rule, provided the 3.8 cm clearance for the prosthetic elbow-lock mechanism is respected. Even in very proximal amputations near the axillary fold, preserving the humeral head is highly valuable. It retains the normal cosmetic contour of the shoulder and provides a bony anchor that improves the stability of a shoulder disarticulation prosthesis.
Pediatric Pitfall - Osseous Overgrowth: In children younger than 12 years, diaphyseal amputations carry a high risk of terminal osseous overgrowth. This is not due to physeal growth, but rather appositional bone formation at the transected distal end of the humerus, which can pierce the skin.
To mitigate pediatric overgrowth, disarticulation is always preferred. If a transhumeral amputation is unavoidable, a capping graft of the humeral bone end is strongly recommended. Techniques include using synthetic caps, iliac crest grafts, or utilizing the amputated distal humerus (epiphyseal transfer) as an autologous capping graft. Close clinical follow-up is mandatory, as stump revisions are frequently required in the growing child.
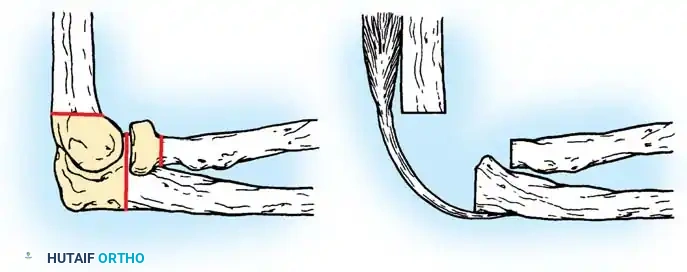
Supracondylar Amputation (Technique 13-6)
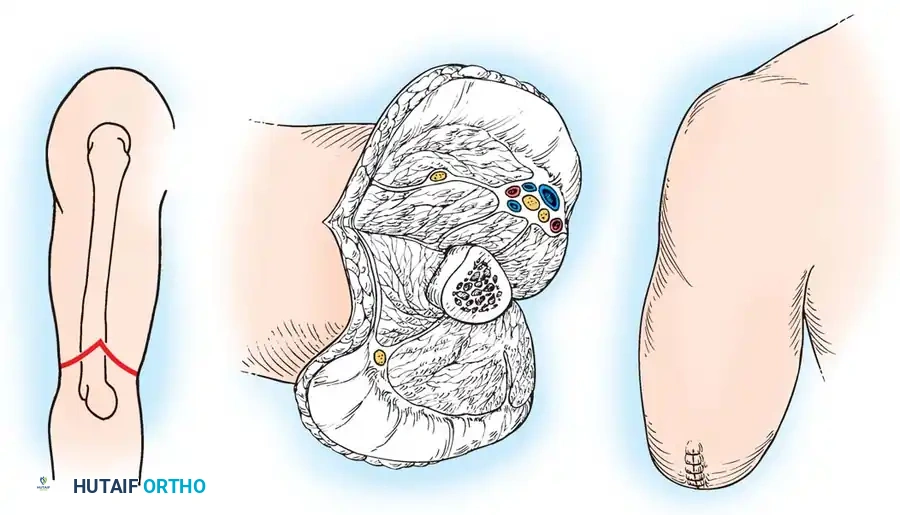
Fig. 13-4: Amputation through the arm at the supracondylar level. (A) Skin incision and bone level. (B) Anterior muscles are divided transversely, triceps and fascial flap is constructed, and bone is sectioned. (C) Completed amputation.
1. Flap Design
Begin proximally at the intended level of bone section. Fashion equal anterior and posterior skin flaps. The length of each flap should be exactly one-half the diameter of the arm at the level of the bone cut (Fig. 13-4A).
2. Neurovascular Management
* Identify the brachial artery and vein just proximal to the level of bone section. Doubly ligate and divide them.
* Identify the median, ulnar, and radial nerves. Apply traction and transect them at a higher level so their proximal ends retract well proximal to the end of the stump, deep into the muscle bellies.
3. Muscle and Bone Sectioning
* Divide the muscles of the anterior compartment (biceps, brachialis) 1.3 cm distal to the level of the intended bone section. This allows the muscle bellies to retract flush with the bone end.
* Free the insertion of the triceps tendon from the olecranon, preserving the triceps fascia and muscle as a long, robust posterior flap. Reflect this flap proximally.
* Incise the periosteum of the humerus circumferentially at a level at least 3.8 cm proximal to the elbow joint line.
* Divide the humerus at this level using an oscillating saw.
* Use a bone rasp to smoothly round the distal end of the humerus, beveling the cortices to prevent soft tissue irritation (Fig. 13-4B).
4. Closure
* Trim the triceps tendon to form a smooth, long flap. Carry it anteriorly across the end of the bone and suture it to the fascia overlying the anterior muscles (myoplasty).
* Insert a closed-suction drain deep to the triceps flap.
* Close the deep fascia with fine absorbable sutures, and approximate the skin flaps with interrupted non-absorbable sutures (Fig. 13-4C).
Proximal Transhumeral Amputation (Technique 13-7)
For amputations proximal to the supracondylar area, the technique is modified slightly to account for the increasing muscle mass and changing cross-sectional anatomy of the arm.
1. Flap Design
Fashion equal anterior and posterior skin flaps beginning at the intended level of bone section. Because the soft tissue envelope is thicker proximally, the length of each flap should be slightly greater than one-half the diameter of the arm at that level to ensure tension-free closure over the bulky muscle.
2. Neurovascular Management
* Isolate, doubly ligate, and divide the brachial artery and vein just proximal to the bone section level.
* Identify the major nerves (median, ulnar, radial, and musculocutaneous). Gently pull them distally and divide them sharply at a more proximal level to ensure deep retraction.
3. Muscle and Bone Sectioning
* Section the anterior compartment muscles 1.3 cm distal to the level of bone section so they retract flush with the bone.
* Divide the triceps muscle 3.8 to 5 cm distal to the level of bone section. Retract its proximal end proximally.
* Incise the periosteum circumferentially and divide the humerus with a saw.
* Meticulously round the end of the bone with a rasp.
4. Closure
* Bevel the bulky triceps muscle to form a thin, pliable flap. Carry this flap over the end of the bone and suture it securely to the anterior muscle fascia.
* Place a closed-suction drain deep to the flap.
* Close the fascia with interrupted absorbable sutures. Trim the skin flaps for a snug, anatomic closure, and approximate the edges with interrupted non-absorbable sutures.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Immediate postoperative care focuses on edema control, pain management, and protection of the surgical site.
1. Dressings: A rigid or semi-rigid dressing is highly recommended to control edema, protect the stump from inadvertent trauma, and prevent knee/elbow flexion contractures.
2. Drain Management: Suction drains are typically removed within 24 to 48 hours once output is minimal.
3. Rehabilitation: Early mobilization of the shoulder joint is critical to prevent adhesive capsulitis. Physical therapy should commence on postoperative day one.
4. Prosthetic Fitting: Once the surgical wound is fully healed and stump volume has stabilized (typically 4 to 6 weeks), the patient is referred to a prosthetist for casting and fitting of a preparatory prosthesis. Early prosthetic fitting is associated with higher long-term acceptance rates and improved psychological outcomes.
📚 Medical References
- Elbow disarticulation and transhumeral amputation: prosthetic management. In Smith DG, Michael JW, Bowker JH, eds: Atlas of amputations and limb defi ciencies, Rosemont, Ill, 2004, American Academy of Orthopaedic Surgeons. Heger H, Millstein S, Hunter GA: Electrically powered prosthesis for the adult with an upper limb amputation, J Bone Joint Surg 67B:278, 1985.
- Hovius SER, Hofman A, van Urk H, et al: Acute management of traumatic forequarter amputations, J Trauma 31:1415, 1991.
- Kour AK, Pho RWH: Combined free fl ap, Ilizarov lengthening, and prosthetic fi tting in the reconstruction of a proximal forearm amputation—a case report, Ann Acad Med Singapore 24:135, 1995.
- Kritter AE: The bilateral upper extremity amputee, Orthop Clin North Am 3:419, 1972.
- Kuhn JA, Wagman LD, Lorant JA, et al: Radical forequarter amputation with hemithoracectomy and free extended forearm fl ap: technical and physiologic considerations, Ann Surg Oncol 1:353, 1994.
- Lagaard SW, McElfresh EC, Premer RF: Gangrene of the upper extremity in diabetic patients, J Bone Joint Surg 71A:257, 1989.
- Levine EA, Warso MA, McCoy DM, et al: Forequarter amputation for soft tissue tumors, Am Surg 60:367, 1994.
- Littlewood H: Amputations at the shoulder and at the hip, BMJ 1:381, 1922.
- Lundborg G, Rosén B: Sensory substitution in prosthetics, Hand Clin 17:481, 2001.
- Merimsky O, Kollender Y, Inbar M, et al: Palliative major amputation and quality of life in cancer patients, Acta Oncol 36:151, 1997.
- Michaels F, De Smet L: Osseous overgrowth in congenital amputations of the upper limb: report of 3 cases treated with autologous stump plasty, Acta Orthop Belg 67:452 2001.
- Miguelez JM, Miguelez MD, Alley RD: Amputations about the shoulder: prosthetic management. In Smith DG, Michael JW, Bowker JH, eds: Atlas of amputations and limb defi ciencies, Rosemont, Ill, 2004, American Academy of Orthopaedic Surgeons. Parker PA, Scott RN: Myoelectric control of prostheses, Crit Rev Biomed Eng 13:283, 1986.
- Pillet J: The aesthetic hand prosthesis, Orthop Clin North Am 12:961, 1981.
- Pinzur MS, Angelats J, Light TR, et al: Functional outcome following traumatic upper limb amputation and prosthetic limb fi tting, J Hand Surg 19A:836, 1994.
- Scott RN: Feedback in myoelectric prostheses, Clin Orthop Relat Res 256:58, 1990.
- Slocum DB: An atlas of amputations , St Louis, 1949, Mosby. Smith DG: Amputations about the shoulder: surgical management. In Smith DG, Michael JW, Bowker JH, eds: Atlas of amputations and limb defi ciencies, Rosemont, Ill, 2004, American Academy of Orthopaedic Surgeons. Stricker SJ: Ilizarov lengthening of a posttraumatic below elbow amputation stump, Clin Orthop Relat Res 306:124, 1994.
- Sturup J, Thyregod HC, Jensen JS, et al: Traumatic amputation of the upper limb: the use of body-powered prosthesis and employment consequences, Prosthet Orthot Int 12:50, 1988.
You Might Also Like