Release of the Flexor-Pronator Origin: Comprehensive Surgical Technique and Biomechanics
Key Takeaway
The release of the flexor-pronator origin is a powerful surgical intervention designed to correct severe, fixed flexion deformities of the wrist and fingers, commonly seen in spastic conditions such as cerebral palsy. This procedure involves a controlled distal slide of the flexor-pronator muscle mass from the medial epicondyle, effectively lengthening the musculotendinous units to restore functional resting posture and facilitate hand hygiene.
INTRODUCTION AND HISTORICAL CONTEXT
The release of the flexor-pronator origin—often referred to as the flexor-pronator slide—is a formidable and highly effective surgical procedure designed to improve the appearance, hygiene, and, in carefully selected cases, the function of a hand afflicted by severe, fixed flexion deformities of the wrist and fingers. These profound contractures are most frequently encountered in patients with upper motor neuron lesions, such as cerebral palsy, traumatic brain injury, or severe post-stroke spasticity, as well as in cases of Volkmann’s ischemic contracture.
Historically, the concept of proximally releasing the flexor musculature to achieve distal lengthening was first described by Page in 1923. The technique was subsequently refined and popularized by Inglis and Cooper, and later by Williams and Haddad, who recognized the biomechanical advantages of a proximal slide over multiple distal tendon lengthenings. By releasing the muscle origin and allowing it to slide distally, the surgeon achieves a global lengthening of the flexor compartment while preserving the relative tension and gliding mechanics of the individual musculotendinous units.
INDICATIONS AND PATIENT SELECTION
The decision to perform a flexor-pronator release must be rooted in a meticulous preoperative clinical and biomechanical assessment. This procedure is a major anatomical rearrangement and is reserved for specific patterns of deformity.
Primary Indications
- Severe, Fixed Flexion Contractures: Patients presenting with rigid flexion deformities of the wrist and fingers that cannot be passively corrected to neutral.
- Hygiene and Skin Integrity: Non-functional hands where the primary goal is to open the palm to prevent maceration, fungal infections, and skin breakdown in the palmar creases.
- Ezaki’s Criteria: As recommended by Ezaki, a flexor-pronator slide is highly indicated if more than 45 degrees of wrist flexion is required to achieve full passive extension of the fingers. This demonstrates a profound shortening of the musculotendinous units that cannot be addressed by simple tendon lengthening.
Contraindications
- Dynamic Deformities: The procedure is strictly contraindicated in hands that can be corrected passively but assume a flexed position only during active grasp. For these dynamic deformities, less extensive operations, such as the transfer of the flexor carpi ulnaris (FCU) to a wrist extensor (e.g., extensor carpi radialis brevis), are far more appropriate and yield superior functional results.
- Athetosis or Dystonia: Patients with severe movement disorders may experience unpredictable results or reversal of deformity.
- Lack of Antagonist Function: If there is absolutely no extensor function (either active or reconstructable), releasing the flexors may simply result in a flail wrist unless accompanied by a wrist arthrodesis.
Clinical Pearl: Always perform a diagnostic nerve block (e.g., median and ulnar nerve block with lidocaine) or utilize botulinum toxin A injections preoperatively. This eliminates the dynamic spastic component, allowing the surgeon to accurately assess the true degree of fixed myostatic contracture.
SURGICAL ANATOMY AND BIOMECHANICS
Understanding the intricate anatomy of the medial elbow and volar forearm is paramount for safely executing the flexor-pronator slide.
The Flexor-Pronator Mass
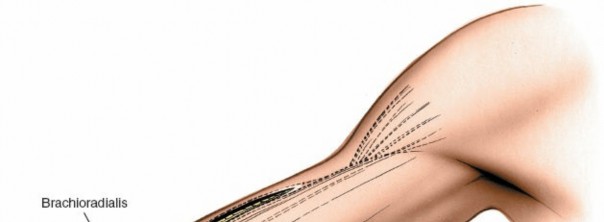
The superficial flexor compartment originates from the medial epicondyle of the humerus via the common flexor tendon. From lateral to medial, these muscles include the pronator teres (PT), flexor carpi radialis (FCR), palmaris longus (PL), flexor digitorum superficialis (FDS), and flexor carpi ulnaris (FCU). The deep compartment, consisting of the flexor digitorum profundus (FDP) and flexor pollicis longus (FPL), arises primarily from the volar aspects of the ulna, radius, and interosseous membrane.
Biomechanics of the "Slide"
By releasing the common flexor origin from the medial epicondyle and elevating the deep flexors from the ulna, the entire muscle mass is permitted to slide distally by 3 to 4 cm. Because the muscle bellies remain attached to their distal tendons, this proximal release effectively lengthens the musculotendinous units. A 3 cm distal slide at the elbow translates to approximately 3 cm of increased excursion at the wrist and fingers, dramatically improving the resting posture of the hand.
Neurovascular Considerations
- Ulnar Nerve: Courses posterior to the medial epicondyle through the cubital tunnel. It gives off critical motor branches to the FCU and the ulnar half of the FDP immediately distal to the epicondyle.
- Median Nerve: Passes between the humeral and ulnar heads of the pronator teres. It must be visualized and protected during the release of the pronator teres and FDS.
- Cutaneous Nerves: The medial antebrachial cutaneous (MABC) nerve and medial brachial cutaneous (MBC) nerve arborize in the superficial fascia over the medial elbow and must be preserved to prevent painful neuromas.
SURGICAL TECHNIQUE: INGLIS AND COOPER METHOD
The following is a highly detailed, step-by-step expansion of the Inglis and Cooper technique for the release of the flexor-pronator origin.
1. Positioning and Setup
- The patient is placed supine on the operating table with the affected upper extremity extended on a radiolucent hand table.
- A well-padded sterile tourniquet is applied high on the brachium.
- The arm is prepped and draped in standard sterile fashion. Exsanguination is performed using an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above systolic pressure).
2. Incision and Superficial Dissection
- Incision: Make a generous longitudinal incision over the anterior aspect of the medial epicondyle of the humerus. Begin the incision 5 cm proximal to the epicondyle and continue it distally to the midpoint of the forearm, following the subcutaneous border of the ulna.
- Cutaneous Nerves: Carefully dissect through the subcutaneous tissue. The medial antebrachial cutaneous (MABC) nerve is frequently encountered in the distal portion of the incision. The medial brachial cutaneous (MBC) nerve can be visualized posterior to the medial aspect of the epicondyle.
- Action: Gently mobilize and retract these cutaneous nerves using vessel loops to prevent traction injury or transection.
Surgical Warning: Transection of the MABC is a common pitfall in medial elbow approaches. A painful neuroma in this location can severely compromise postoperative rehabilitation and patient satisfaction.
3. Ulnar Nerve Neurolysis
- Identify the ulnar nerve proximal to the medial epicondyle in the distal arm.
- Incise the fascia of the cubital tunnel (Osborne’s ligament) and carefully elevate the ulnar nerve from its groove behind the epicondyle.
- Perform a meticulous neurolysis, freeing the nerve distally as it passes between the two heads of the FCU.
- Critical Step: Identify, meticulously free, and protect the motor branches of the ulnar nerve that innervate the FCU and the two ulnar heads of the FDP. These branches are delicate and tether the nerve to the muscle mass; they must be mobilized to allow the muscle to slide distally without causing a traction palsy.
4. Distal-to-Proximal Muscle Elevation
- To systematically release the origins of the FCU and FDP, begin distally at approximately the middle of the ulna.
- Incise the fascia along the subcutaneous border of the ulna. Using a periosteal elevator or electrocautery, elevate both the FCU and FDP muscles from the bone.
- As the elevation proceeds from ulnar to radial, the interosseous membrane will be visualized along the volar surface of the bone.
- Continue this subperiosteal elevation proximally along the ulna, advancing as far as the ulnar groove at the medial epicondyle.
- During this deep dissection, the interosseous membrane and the glistening fascia of the brachialis muscle will become clearly visible in the depths of the surgical wound.
5. Release of the Medial Epicondyle
- Temporarily replace the ulnar nerve into its groove to protect it from the anterior dissection.
- Identify the common flexor-pronator muscle mass at its origin on the medial epicondyle.
- Using a scalpel or heavy Mayo scissors, sharply divide the entire flexor-pronator muscle mass from the medial epicondyle.
- As the pronator teres is released, carefully identify the median nerve. The median nerve can be seen passing between the humeral and ulnar heads of the pronator teres. Ensure the nerve is completely free from fascial bands that might tether it during the distal slide.
6. Anterior Dissection and Lacertus Fibrosus
- Continue the dissection anteriorly over the flexor aspect of the elbow.
- Identify and divide the lacertus fibrosus (bicipital aponeurosis). This structure often acts as a secondary tether; its release is mandatory to allow full distal excursion of the flexor mass.
- Release any remaining fibrous attachments of the flexor muscle origin from the anterior joint capsule of the elbow.
7. Addressing Elbow Flexion Contractures
- Assess the elbow for residual flexion contracture. In many spastic patients, a concomitant elbow flexion contracture is present.
- If the elbow cannot be fully extended passively at this stage, incise the fascia of the brachialis muscle transversely. Take care not to injure the underlying brachial artery or median nerve.
- Fractional lengthening of the biceps tendon may be considered if severe contracture persists, though fascial release is often sufficient.
8. Ulnar Nerve Transposition and Muscle Slide
- Because the flexor muscle mass will now slide distally, leaving the ulnar nerve in its anatomical groove would subject it to severe traction and potential kinking against the medial epicondyle.
- Therefore, transplant the ulnar nerve anterior to the medial epicondyle into a well-vascularized subcutaneous bed. Secure the subcutaneous tissue loosely to the medial epicondyle to create a sling, preventing the nerve from subluxating back into the groove.
- At this juncture, observe the flexor-pronator muscle mass. It should have displaced 3 to 4 cm distal to its original anatomical location. The wrist and fingers should now passively extend with significantly less resistance.
9. Hemostasis and Closure
- Deflate the tourniquet and achieve meticulous hemostasis. The extensive raw surface area generated by the muscle slide is prone to hematoma formation.
- Place a closed-suction drain in the deep space if oozing is significant.
- Close the subcutaneous tissues and skin in layers.
10. Immobilization
- Apply a well-padded, long-arm cast or rigid plaster splints.
- Positioning: The forearm must be held in full supination. The wrist and fingers should be positioned in neutral extension (or maximum allowable extension without causing vascular compromise to the digits).
Pitfall: Do not force the wrist and fingers into extreme hyperextension during casting. The acute lengthening of the neurovascular bundles can lead to neurapraxia or vascular compromise. Neutral position is the safest and most effective posture for the initial healing phase.
POSTOPERATIVE CARE AND REHABILITATION
The success of a flexor-pronator slide relies as much on rigorous postoperative management as it does on surgical execution. The tendency for spastic muscles to re-contract is high, necessitating prolonged splinting.
Phase I: Initial Healing (Weeks 0 - 3)
- The patient remains in the initial long-arm cast or rigid splint applied in the operating room.
- Elevation of the extremity is critical to manage edema.
- At 3 weeks postoperatively, the cast or splints are removed, and skin sutures are extracted.
Phase II: Continuous Splinting (Weeks 3 - 12)
- A custom-fabricated, thermoplastic extension hand and wrist splint is applied by an occupational therapist.
- This splint must hold the wrist in neutral to slight extension, with the metacarpophalangeal (MCP) and interphalangeal (IP) joints in extension.
- The splint is worn constantly (24 hours a day) for 3 months, removed only for supervised hygiene and gentle passive range-of-motion (ROM) exercises.
Phase III: Night Splinting and Maturation (Months 3 - 6+)
- After 3 months of continuous wear, the splinting regimen is reduced to nighttime wear only for an additional 3 months.
- During the day, the patient engages in active and active-assisted ROM exercises, focusing on strengthening the antagonist extensor musculature.
- Pediatric Consideration: In growing children with cerebral palsy, the risk of recurrent contracture due to bone growth outpacing spastic muscle growth is significant. Therefore, night splinting should be maintained indefinitely, ideally until skeletal maturity is reached.
COMPLICATIONS AND MANAGEMENT
While highly effective, the flexor-pronator slide carries specific risks due to the extensive dissection required.
- Ulnar Nerve Palsy: The most common neurological complication. It usually results from inadequate mobilization of the motor branches or failure to properly transpose the nerve anteriorly, leading to traction neuritis. Management includes immediate release of tight splints and, if persistent, surgical exploration.
- Hematoma Formation: Due to the large dead space created by the muscle slide. Meticulous hemostasis and the use of a postoperative drain mitigate this risk.
- Under-correction: Often due to failure to release the lacertus fibrosus, incomplete elevation of the FDP from the ulna, or unrecognized joint capsular contractures.
- Over-lengthening: Rare, but can result in a severe loss of grip strength. This underscores the importance of proper patient selection; the procedure is primarily for salvage of severe deformity rather than fine-tuning functional grip.
CONCLUSION
The release of the flexor-pronator origin via the Inglis and Cooper technique remains a cornerstone in the operative management of the severely spastic, contracted hand. By understanding the biomechanical principles of the proximal muscle slide and adhering to meticulous surgical technique—particularly regarding neurovascular protection—the orthopaedic surgeon can reliably restore a functional resting posture, facilitate essential hygiene, and significantly improve the patient's quality of life.
You Might Also Like