Comprehensive Management of Talar Neck Fractures: An Operative Guide
Key Takeaway
Talar neck fractures are complex injuries historically termed "aviator's astragalus." Management requires meticulous assessment, precise surgical timing, and anatomical reduction to prevent devastating complications like osteonecrosis (AVN) and varus malunion. This guide details the Hawkins classification, optimal imaging including the Canale view, dual anteromedial and anterolateral surgical approaches, and modern fixation strategies using cannulated screws and mini-fragment plates to optimize patient outcomes.
Introduction and Historical Context
Many controversies surround the treatment of talar neck fractures, reflecting the inherent difficulties in clinical assessment, the selection of surgical approaches, the optimization of fixation methods, and the high frequency of postoperative complications. The historical context of these injuries provides insight into their high-energy nature. In 1919, Anderson, having observed 18 patients with talar injuries in the Royal Flying Corps, coined the term aviator’s astragalus. These injuries occurred when pilots crashed, driving the rudder bar forcefully up into the plantar aspect of the foot.
In 1952, Coltart reviewed 25,000 fractures sustained during World War II. He identified 228 talar fractures, 106 of which were classified specifically as talar neck fractures. His landmark review reported osteonecrosis (AVN) rates of 35% associated with subtalar dislocation and a staggering 95% with combined ankle and subtalar dislocation. Since Coltart’s report, the exact incidence of osteonecrosis after talar neck injuries has been widely debated. However, a universal consensus remains: increasing levels of displacement and dislocation progressively disrupt the tenuous extraosseous and intraosseous vasculature of the talus, directly increasing the incidence of osteonecrosis.
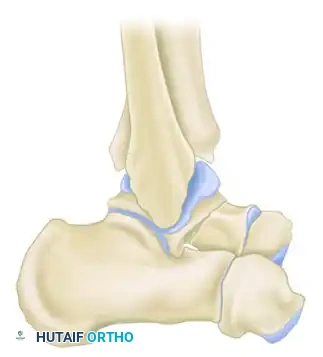
Surgical Anatomy and Biomechanics
Any fracture that involves a joint presents a difficult reconstructive problem, and this is especially true of a primary weight-bearing joint like the ankle and subtalar complex. Approximately 60% to 70% of the surface of the talus is covered by articular cartilage, leaving a limited footprint for vascular penetration. For this reason, almost any fracture of the talus involves a joint surface and threatens the blood supply.
More weight per unit of area is borne by the superior articular surface of the talar dome than by any other bone in the human body. Accurate reduction is therefore essential to reestablish the precise position of its articular surfaces. Any residual irregularity of the joint surfaces will inevitably produce rapid posttraumatic arthritic changes upon the resumption of motion and weight-bearing.
Clinical Pearl: The blood supply to the talus is retrograde. The artery of the tarsal canal (a branch of the posterior tibial artery) supplies the majority of the talar body. The deltoid branch provides a critical, often sole remaining blood supply in displaced fractures. Surgical approaches must meticulously preserve the deltoid ligament to avoid iatrogenic devascularization.
Classification: The Hawkins System
In 1970, Hawkins published a landmark paper detailing the results of 57 talar neck fractures in 55 patients. His classification of talar neck fractures remains the most widely used system today. It is simple, provides clear guidelines for treatment, and is highly prognostic for the development of osteonecrosis and the likelihood of a successful clinical outcome.
Canale and Kelly later reviewed 71 fractures of the neck of the talus with an average follow-up of 12.7 years, adding a Type IV to the original Hawkins classification to account for talonavicular dislocation.
Type I: Nondisplaced Fractures
Type I fractures are nondisplaced vertical fractures of the talar neck. Historically, osteonecrosis did not occur, and all fractures united. However, Canale and Kelly noted that in 2 of 13 nondisplaced fractures, osteonecrosis did develop, though both ultimately had excellent clinical results.
Type II: Subtalar Subluxation or Dislocation
Type II fractures are displaced talar neck fractures with subluxation or dislocation of the subtalar joint, while the ankle joint remains congruous. In Hawkins' original series, all Type II fractures united, although osteonecrosis subsequently developed in 42%. Canale and Kelly reported a 50% osteonecrosis rate, with 47% yielding an unsatisfactory clinical result.

Type III: Subtalar and Ankle Dislocation
Type III fractures involve dislocation of both the subtalar and the ankle joints. The talar body is often extruded posteromedially. In these severe injuries, nonunion occurred in 11% of Hawkins' patients, and osteonecrosis developed in 91%. An increasing percentage of fair and poor results (75%) was noted compared with Type II fractures.

Type IV: Pan-Talar Dislocation
Added by Canale and Kelly, Type IV fractures describe an injury in which not only is the body of the talus extruded from the ankle mortise (as in Type III), but the head of the talus is also subluxed or dislocated from the navicular articulation. This represents a catastrophic disruption of the talar vascular supply.

Clinical Evaluation and Imaging
Care must be taken to search for local and remote associated fractures. A medial malleolar fracture is commonly associated with a displaced talar neck fracture. Furthermore, as with any axial loading injury (e.g., falls from a height, high-speed motor vehicle collisions), the lumbar spine, tibial plateau, and calcaneus should be evaluated thoroughly.
Radiographic Protocols
Standard radiographic evaluation of talar neck injuries must include:
* Anteroposterior (AP) view of the ankle
* Lateral view of the ankle
* Mortise (oblique) view of the ankle
* AP, lateral, and oblique views of the foot
The Canale View:
Intraoperatively and postoperatively, the view described by Canale is exceptionally helpful because it perfectly profiles the talar neck, allowing the surgeon to assess for subtle displacement and varus malalignment.
* Positioning: The foot is maximally plantarflexed and internally rotated 15 degrees.
* Beam Angle: The x-ray beam is angled 75 degrees cephalad from the horizontal plane.

Surgical Warning: A talar neck fracture must be thoroughly evaluated before labeling it as a Type I. Many fractures, if examined closely by CT scans, display subtle displacement. If any doubt exists about the presence of displacement, a fine-cut CT scan with sagittal and coronal reconstructions is mandatory.
Indications and Timing of Surgery
Nonoperative Management (Type I)
Impacted fractures of the head, usually associated with compression fractures of the navicular, or strictly nondisplaced Type I fractures, can be treated nonoperatively. If the subtalar joint is completely free of displacement and intra-articular fragments, the fracture should be immobilized in a below-knee cast for 8 to 12 weeks. Weight-bearing is strictly delayed until trabeculation across the fracture is radiographically confirmed.
Operative Management (Types II, III, and IV)
As a rule, displaced fractures of the neck of the talus should be treated with prompt Open Reduction and Internal Fixation (ORIF) because it is virtually impossible to obtain and maintain an anatomical reduction by closed means.
Timing of Intervention:
In early studies, emergent ORIF was advocated for all displaced fractures to preserve blood supply. More recent studies, such as those by Vallier et al., suggest that while prompt reduction of dislocated joints is critical to relieve tension on the soft tissues and neurovascular structures, definitive internal fixation can be safely delayed until soft tissue swelling has subsided.
However, Type III and Type IV fractures constitute an absolute orthopaedic emergency for two primary reasons:
1. Pressure from the dislocated talar body on the skin and neurovascular structures can lead to rapid skin sloughing and irreversible neurovascular insult.
2. The only remaining blood supply to the talus—the deltoid branch—may be rotated, stretched, and occluded. This ischemia is correctable only through emergency reduction of the talar body.
Surgical Approaches
Historically, a posterolateral approach was advocated, supported by biomechanical studies showing that the greatest strength of fixation was achieved with screws placed from a posterior-to-anterior direction. However, the current literature and modern surgical consensus strongly support the use of anterior approaches. Anterior approaches provide superior visualization of the fracture site, allowing for precise anatomical reduction of the articular surfaces.
The Dual Approach (Anteromedial and Anterolateral)
Because the talar neck is commonly comminuted medially, fracture alignment and reduction can be exceptionally difficult to assess from a single incision. Relying on a single approach frequently leads to an unrecognized varus malunion.
- Anteromedial Approach: The incision is made medial to the tibialis anterior tendon, extending from the anterior medial malleolus toward the navicular. This offers excellent exposure of the medial talar neck and is easily extended proximally if a medial malleolar osteotomy is required.
- Anterolateral Approach: We do not hesitate to add an anterolateral approach. The incision is made in line with the fourth ray, over the sinus tarsi. This allows direct visualization of the lateral talar neck and the subtalar joint, helping to assess reduction, correct varus, and offering a robust region for lateral screw or plate fixation.
Pitfall: Most authors agree that varus malunion, even of a few degrees, is almost uniformly associated with a poor outcome. Varus malalignment locks the transverse tarsal joint, severely restricting hindfoot eversion and leading to a rigid, painful foot. Dual incisions are the best defense against this complication.
Medial Malleolar Osteotomy
Open reduction of Type III and IV fractures, or complex talar body fractures, generally requires a medial malleolar osteotomy for adequate exposure. A chevron-type osteotomy is preferred. The osteotomy is pre-drilled and tapped for later repair. This approach provides unparalleled access to the medial talar dome and body, which is often inaccessible through standard incisions.
Operative Technique: Step-by-Step ORIF
1. Patient Positioning and Preparation
The patient is placed supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct natural external rotation, bringing the foot into a neutral position. A thigh tourniquet is applied. Fluoroscopy must be positioned to easily obtain AP, lateral, and Canale views.
2. Fracture Exposure and Debridement
Utilizing the dual anteromedial and anterolateral approaches, the fracture site is exposed. Hematoma and small, devitalized, non-articular cortical fragments are carefully debrided to allow visualization of the main fracture edges. Crucially, the deltoid ligament must not be elevated from the medial talar body.
3. Fracture Reduction
Reduction is often achieved by plantarflexing the foot to match the distal fragment to the plantarflexed proximal talar body. Dental picks, K-wires used as joysticks, and small point-to-point reduction clamps are utilized. The reduction must be visually confirmed both medially and laterally to ensure no varus or valgus malalignment exists.
4. Hardware Fixation: Cannulated Screws
Once provisionally held with K-wires, definitive fixation is typically achieved using titanium cannulated screws (usually 3.5 mm or 4.0 mm).
* Anteroposterior (AP) screw placement is standard. One screw is placed from the medial side of the talar head into the medial body, and a second is placed from the lateral process into the lateral body.
* Screws must be countersunk to prevent impingement on the navicular or anterior tibial plafond.
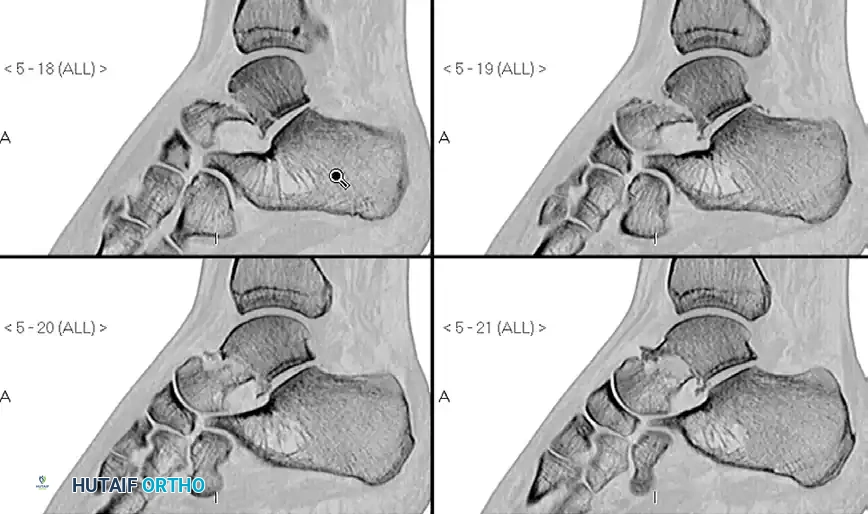
Pre-operative Imaging (Talar Neck Fracture):

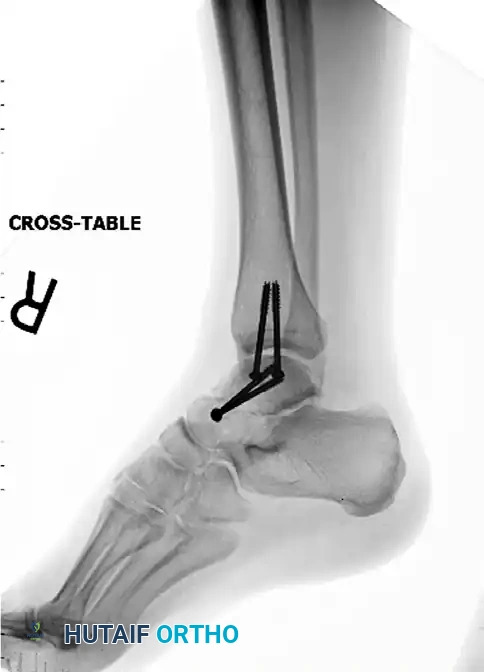
Post-operative Fixation with Cannulated Screws:

5. Alternative Fixation: Mini-Fragment Plates
In cases of severe comminution, particularly medial comminution where screw fixation alone would lead to shortening and varus collapse, mini-fragment plates (2.0 mm or 2.4 mm) are highly effective. The plate acts as a buttress to maintain length and alignment.
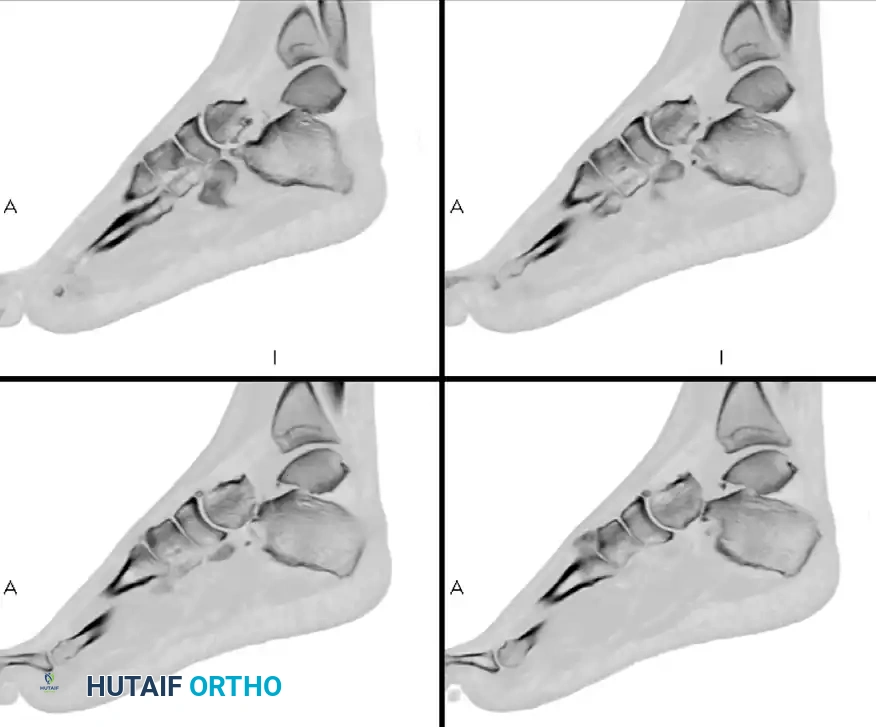
Pre-operative Imaging (Comminuted Talar Neck Fracture):

Post-operative Fixation with Mini-Fragment Plate and Screws:


Postoperative Protocol and Complications
Rehabilitation Protocol
Postoperatively, the patient is placed in a bulky Jones splint. Once incisions are healed (typically 2-3 weeks), the patient is transitioned to a short-leg cast or rigid CAM boot.
* Weight-Bearing: Strict non-weight-bearing is maintained for a minimum of 8 to 12 weeks.
* Motion: Early active range of motion of the ankle and subtalar joints may be initiated at 2 to 4 weeks if stable fixation was achieved and the soft tissue envelope is secure.
* Weight-bearing is only advanced when radiographic evidence of trabecular bridging across the fracture site is confirmed.
Complications
1. Osteonecrosis (AVN):
The rate of osteonecrosis ranges from 20% to 50% in modern series, with higher rates in patients with comminuted or open fractures. At 6 to 8 weeks post-injury, an AP radiograph of the ankle should be evaluated for the Hawkins Sign.
* Positive Hawkins Sign: A subchondral radiolucent band in the talar dome. This indicates that the bone is vascularized and undergoing disuse osteopenia. It is a highly reliable indicator that AVN will not occur.
* Negative Hawkins Sign: Sclerosis of the talar dome relative to the surrounding osteopenic bone, indicating avascularity.
2. Posttraumatic Arthritis:
The rate of posttraumatic arthritis varies from 54% to 100%, most commonly affecting the subtalar joint, followed by the tibiotalar joint. It is directly correlated with the severity of the initial cartilage impact and the accuracy of the surgical reduction. Approximately 50% of patients require secondary surgery—usually a subtalar or triple arthrodesis—at 10 years after injury for pain relief.
3. Varus Malunion:
As previously emphasized, varus malunion is a devastating complication. It forces the foot into a supinated position, overloading the lateral border of the foot and locking the transverse tarsal joints. Prevention through dual surgical approaches and meticulous intraoperative Canale views is paramount, as corrective osteotomies of the talar neck are technically demanding and yield unpredictable results.
You Might Also Like
