Subtalar Dislocations: Comprehensive Surgical Management
Key Takeaway
Subtalar dislocations, or peritalar dislocations, involve the simultaneous dislocation of the distal articulations of the talus at the talocalcaneal and talonavicular joints. Medial dislocations are most common and often reducible closed. Lateral dislocations frequently require open reduction due to soft tissue interposition, typically the posterior tibial tendon. Post-reduction computed tomography is mandatory to identify occult osteochondral fractures or intra-articular debris that may necessitate surgical debridement or internal fixation to prevent post-traumatic arthrosis.
Introduction to Subtalar Dislocations
Subtalar dislocations, historically referred to as peritalar dislocations, represent a severe and complex disruption of the hindfoot architecture. In this injury pattern, the normal anatomic relationships of the talocalcaneal and talonavicular joints are simultaneously obliterated. Consequently, the calcaneus, cuboid, navicular, and the entire forefoot become displaced as a single unit from the inferior and distal aspects of the talus. The tibiotalar (ankle) joint and the calcaneocuboid joint typically remain intact.
These injuries are relatively rare, accounting for approximately 1% to 2% of all traumatic joint dislocations, and are most frequently the result of high-energy trauma such as motor vehicle collisions, falls from a height, or severe athletic injuries (often termed "basketball foot"). Because of the immense forces required to disrupt the robust ligamentous restraints of the peritalar complex—namely the talocalcaneal interosseous ligament, the cervical ligament, and the joint capsules—subtalar dislocations are frequently associated with severe soft tissue compromise, osteochondral shear fractures, and long-term morbidity.
Pathoanatomy and Classification
Subtalar dislocations are classified based on the direction of the displacement of the foot (calcaneus and navicular) relative to the talus.
Medial Subtalar Dislocations
Medial dislocations are by far the most common, accounting for approximately 65% to 80% of all subtalar dislocations, as corroborated by Bibbo et al. in one of the largest modern series.
* Mechanism of Injury: Typically results from forced inversion of a plantarflexed foot. The talus is forced laterally while the rest of the foot displaces medially.
* Clinical Appearance: The foot assumes an "acquired clubfoot" deformity. The head of the talus is prominent dorsolaterally, and the skin over the lateral aspect of the talus is often severely tented, placing it at high risk for ischemic necrosis.
* Reducibility: Medial subtalar dislocations, in the absence of marginal fractures of the calcaneus or talus, are almost always reducible by closed means.
Lateral Subtalar Dislocations
Lateral dislocations account for 15% to 35% of cases and are generally associated with higher-energy trauma.
* Mechanism of Injury: Results from forced eversion of a dorsiflexed foot. The talus is driven medially while the foot displaces laterally.
* Clinical Appearance: The foot assumes an "acquired flatfoot" deformity. The head of the talus is prominent medially.
* Reducibility: Lateral subtalar dislocations are frequently irreducible by closed manipulation. The most common offending structures blocking reduction are the posterior tibial tendon (which can become entrapped in the talonavicular joint) and osteochondral fractures of the talus.
Anterior and Posterior Dislocations
These are exceedingly rare (less than 5% combined) and usually result from extreme, direct high-energy forces. They are frequently open injuries with devastating soft tissue and neurovascular consequences.
Clinical Pearl: The "Irreducible" Dislocation
When a subtalar dislocation resists closed reduction under adequate sedation and muscle relaxation, repeated forceful attempts must be strictly avoided. Multiple closed reduction attempts exacerbate soft tissue trauma, increase the risk of iatrogenic osteochondral damage, and elevate the risk of compartment syndrome. Proceed directly to the operating room for open reduction.
Clinical and Radiographic Evaluation
Initial Assessment
Patients present with gross deformity, severe pain, and swelling. A meticulous neurovascular examination is paramount. The posterior tibial artery and nerve are particularly vulnerable in lateral dislocations, while the superficial peroneal nerve and dorsalis pedis artery are at risk in medial dislocations. Skin tenting over the prominent talar head requires emergent reduction to prevent full-thickness skin necrosis.
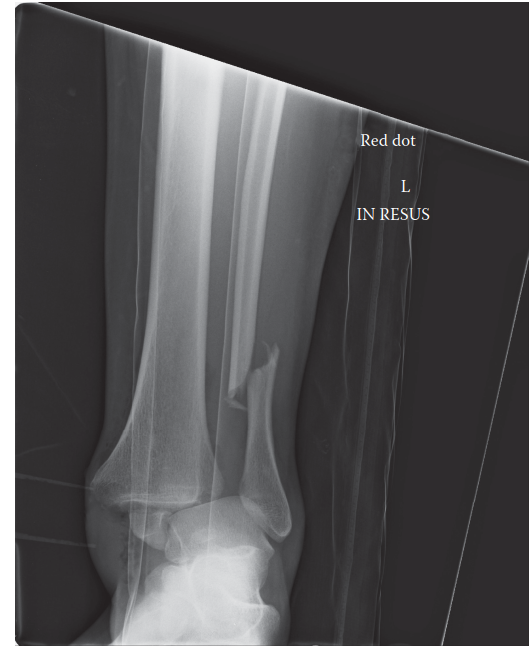
Radiographic Imaging
Standard trauma radiographs of the foot and ankle (Anteroposterior, Lateral, and Mortise views) are required.
* AP View: Demonstrates the talonavicular dislocation.
* Lateral View: Demonstrates the talocalcaneal dislocation and the loss of the normal talocalcaneal angle.
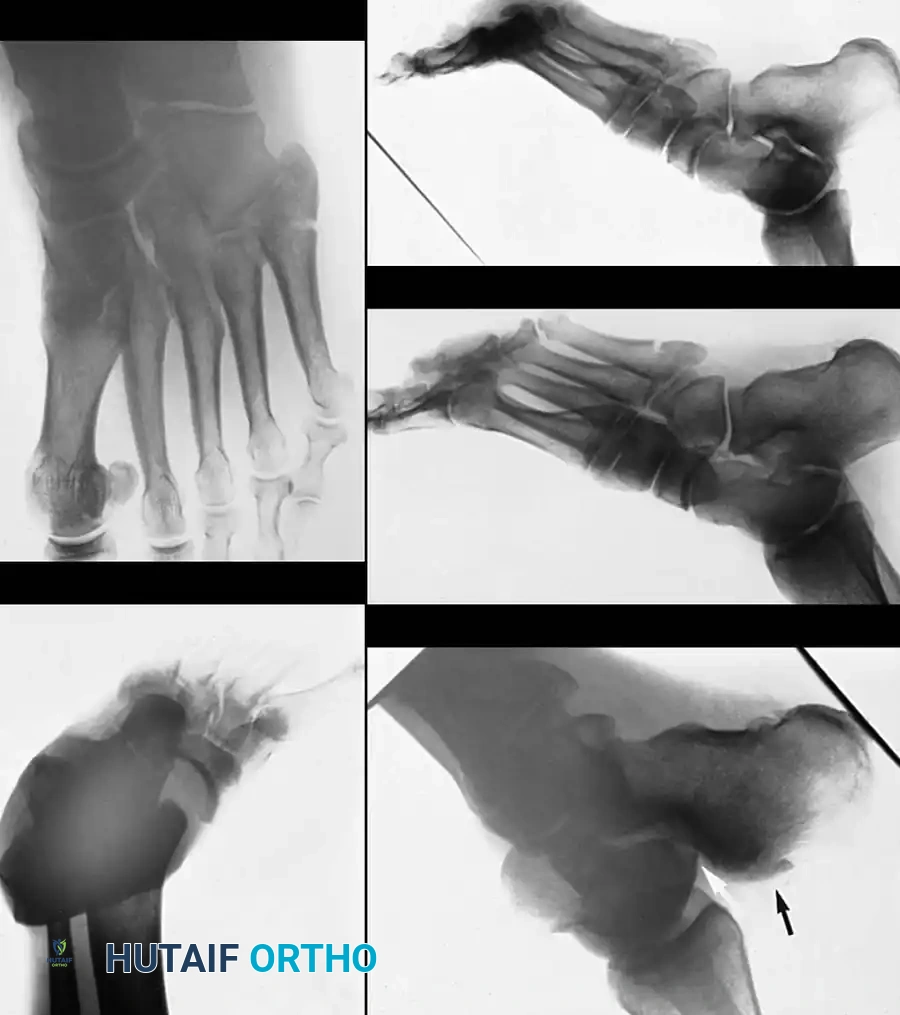
The Critical Role of Post-Reduction CT Scanning
Bibbo et al. emphasized the absolute necessity of obtaining a computed tomography (CT) scan after the reduction of a subtalar dislocation. In their series, patients who sustained a subtalar dislocation had a high incidence of additional abnormalities identified on CT that were initially missed on plain radiographs.
We routinely use CT for the definitive evaluation of these injuries. CT imaging frequently reveals:
* Osteochondral shear fractures of the talar dome or subtalar articular facets.
* Fractures of the lateral process of the talus (snowboarder's fracture).
* Impaction fractures of the navicular.
* Intra-articular debris blocking congruent reduction.
If a congruent reduction is obtained and proven on a post-reduction CT scan, and there are no intra-articular fragments or displaced bone fragments requiring repair, subtalar dislocations can be routinely treated nonoperatively.
Evidence-Based Outcomes and Prognosis
The long-term results after closed subtalar dislocations without associated fractures are generally good; however, patients must be counseled that subtalar motion may be moderately limited permanently, and walking on uneven surfaces often remains awkward.
Impact of Associated Fractures
After reviewing 17 subtalar dislocations observed for an average of 35 months, DeLee and Curtis concluded that if an osteochondral fracture is seen on post-reduction imaging, open reduction and internal fixation (ORIF) or excision of the fragment might significantly reduce the risk of degenerative arthritis.
Immobilization Protocols
Zimmer and Johnson investigated the duration of immobilization. They found a frequent incidence of subtalar instability when the period of immobilization was shortened and early exercises were instituted. Based on their findings, a strict 6 weeks of cast immobilization is recommended to allow the robust peritalar ligaments to heal adequately.
Severe and Open Injuries
In a long-term review of severe open subtalar dislocations, Goldner et al. found considerably worse results compared to closed injuries. Reviewing 15 adolescents and adults at an average of 18 years after a type III open subtalar dislocation, they noted devastating associated injuries:
* 10 tibial nerve injuries
* 5 posterior tibial tendon ruptures
* 5 posterior tibial nerve lacerations
* 12 articular fractures involving the subtalar joint
* 3 talar dome fractures
Crucially, the investigators found osteonecrosis (AVN) in the body of the talus in one-third of the patients. Approximately half of the patients in this severe cohort eventually required some form of arthrodesis procedure.
Bibbo et al. evaluated 25 patients and found that open reduction was required in 32%, with irreducibility statistically significantly associated with high-energy injury. Eighty-eight percent of patients sustained additional injuries to the affected foot and ankle. After a mean follow-up of 5 years, the American Orthopaedic Foot and Ankle Society (AOFAS) score of the dislocated extremity was significantly lower compared with the uninjured side (71 versus 93). Radiographically, 89% showed subtalar joint abnormalities, with 63% being symptomatic, and 16% eventually requiring subtalar arthrodesis.

Surgical Management: Open Reduction Technique
When closed reduction fails, or when post-reduction CT reveals intra-articular fragments blocking congruent reduction, open reduction is indicated.
Surgical Warning: Blocks to Reduction
In lateral dislocations, the posterior tibial tendon frequently blocks reduction and must be physically lifted out of the talonavicular joint. In medial dislocations, the extensor retinaculum, extensor digitorum brevis, or the capsule of the talonavicular joint may interpose.
Technique 86-12: Open Reduction of Subtalar Dislocation
1. Patient Positioning and Preparation
* Place the patient supine on a radiolucent operating table.
* Apply a well-padded thigh tourniquet.
* Ensure fluoroscopy (C-arm) is available and positioned to obtain true AP, lateral, and oblique views of the hindfoot and midfoot.
2. The Anterolateral Approach
* Make a longitudinal anterolateral incision approximately 7.5 cm long, starting from just proximal to the ankle joint and extending distally to the cuboid.
* Nerve Protection: Carefully identify and protect the medial and lateral dorsal cutaneous branches of the superficial peroneal nerve, which frequently cross the operative field.
* Deep Dissection: Retract the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) tendons medially. Retract the peroneus tertius tendon laterally. This interval provides excellent exposure of the lateral talus, the subtalar joint, and the midtarsal joints.
3. Capsulotomy and Joint Exposure
* Incise the capsule over the head and neck of the talus.
* Extend the capsular incision distally into the midtarsus to fully visualize the talonavicular and calcaneocuboid articulations.
* Irrigate the joint copiously to remove hematoma and small osteochondral debris.
4. Reduction Maneuvers
* Insert a bone skid or a robust periosteal elevator into the subtalar joint.
* Utilize leverage and longitudinal traction to disengage the locked articular surfaces and reduce the dislocation of the subtalar and talonavicular joints.
* For Medial Dislocations: Have an assistant simultaneously abduct and evert the foot while traction is applied.
* For Lateral Dislocations: Have the assistant adduct and invert the foot.
5. Addressing the Irreducible Lateral Dislocation (The Medial Approach)
* In a lateral dislocation, if the anterolateral approach does not yield reduction, the posterior tibial tendon is likely entrapped.
* Make a separate medial incision centered over the talonavicular joint.
* Carefully dissect and lift the dorsal neurovascular bundle and the offending posterior tibial tendon out of the talonavicular joint space.
* Incise the dorsal capsule of the talonavicular joint. With this structure loosened and the tendon retracted, the navicular may be levered around the head of the talus with a periosteal elevator to achieve anatomic reduction.
6. Assessment of Stability and Fixation
* Once reduced, assess the stability of the subtalar and talonavicular joints under fluoroscopy.
* If the reduction is highly unstable (often due to severe ligamentous disruption or associated fractures), hold the reduction with longitudinally placed stout Steinmann pins or Kirschner wires (K-wires).
* Pass the pins across the calcaneocuboid and talonavicular joints. Ensure the pins do not violate the tibiotalar joint.
* Leave the pins in place for 4 weeks to maintain alignment while early soft tissue healing occurs.
7. Closure
* Repair the joint capsules if tissue quality permits.
* Close the extensor retinaculum to prevent tendon bowstringing.
* Perform a meticulous layered closure of the subcutaneous tissue and skin.
Postoperative Protocol and Rehabilitation
The postoperative management of subtalar dislocations requires a delicate balance between protecting the healing peritalar ligaments and preventing profound hindfoot stiffness.
Phase I: Immediate Postoperative Period (0 to 6 Weeks)
- Immobilization: A well-padded short-leg cast is applied from the base of the toes to the tibial tuberosity over a bulky compression dressing.
- Swelling Management: The cast must be bivalved immediately in the recovery room to accommodate anticipated severe postoperative swelling and prevent compartment syndrome.
- Early Motion: Active exercises of the metatarsophalangeal (MTP) joints are encouraged immediately to prevent forefoot stiffness and aid in edema reduction.
- Weight Bearing: The patient is strictly non-weight bearing on the operative extremity.
- Pin Management: If Steinmann pins were utilized for stability, they are typically removed in the clinic at the 4-week mark.
Phase II: Transition and Early Mobilization (6 to 10 Weeks)
- At exactly 6 weeks, cast immobilization is discontinued (adhering to the recommendations of Zimmer and Johnson to prevent chronic instability).
- Orthosis: A custom lace-up foot and ankle leather corset or a rigid controlled ankle motion (CAM) boot is applied.
- Physical Therapy: Active inversion, eversion, dorsiflexion, and plantarflexion of the foot and ankle are initiated and strongly encouraged. Passive forceful stretching is avoided.
- Weight Bearing: Weight bearing to tolerance with crutches is allowed. The corset/boot is worn for at least 1 month to control dependent edema and provide mechanical support.
Phase III: Maturation and Strengthening (10+ Weeks)
- Full weight bearing should be comfortable by 6 to 8 weeks after the injury.
- Patients are transitioned to supportive athletic footwear.
- Patient Counseling: It is imperative to advise patients early in the treatment course that the foot and ankle may continue to swell for up to a year. Furthermore, the midfoot and hindfoot will likely feel stiff for several months, and a permanent loss of 20% to 50% of subtalar inversion/eversion is a common and expected outcome, even with a perfect anatomic reduction.
You Might Also Like