Fractional Lengthening of the Flexor Carpi Radialis and Finger Flexors
Key Takeaway
Fractional lengthening of the flexor carpi radialis and finger flexors is a cornerstone surgical intervention for managing spastic flexion contractures of the wrist and hand. By selectively dividing the aponeurosis while preserving the underlying muscle fibers, surgeons can achieve controlled elongation of the muscle-tendon unit. This guide details the biomechanical principles, step-by-step surgical approaches, and postoperative protocols necessary to optimize functional outcomes and prevent recurrence.
INTRODUCTION TO SPASTIC FLEXION CONTRACTURES OF THE WRIST AND HAND
Spastic flexion contractures of the wrist and fingers represent a profound source of functional impairment and hygienic difficulty in patients with upper motor neuron syndromes, such as cerebral palsy, traumatic brain injury, and post-stroke spastic hemiplegia. The flexor carpi radialis (FCR), flexor digitorum superficialis (FDS), and flexor digitorum profundus (FDP) are frequently implicated in these debilitating deformities.
When conservative measures—including aggressive orthotic management, physical therapy, and targeted botulinum toxin injections—fail to halt the progression of a dynamic deformity into a fixed myostatic contracture, surgical intervention becomes necessary. Fractional lengthening (also known as fractional recession) and the more extensive flexor slide are two highly effective, evidence-based techniques utilized to restore the biomechanical balance of the wrist and hand.
Unlike traditional Z-lengthening of the tendon, which can lead to unpredictable weakness and extensive adhesion formation, fractional lengthening relies on the controlled division of the aponeurotic sleeve overlying the muscle belly. This allows the intact muscle fibers to slide and elongate, providing a predictable increase in the resting length of the musculotendinous unit while preserving its continuity and functional strength.
BIOMECHANICAL PRINCIPLES OF FRACTIONAL LENGTHENING
The success of fractional lengthening is predicated on the unique microanatomy of the forearm flexors. The distal portion of the muscle belly in these units is enveloped by a dense aponeurosis that progressively thickens distally to form the true tendon.
By making a transverse incision exclusively through this aponeurotic fascia—proximal to the true musculotendinous junction—the surgeon releases the inelastic fibrous constraint. When passive tension (dorsiflexion of the wrist or extension of the digits) is subsequently applied, the underlying elastic muscle fibers stretch, causing the edges of the incised aponeurosis to separate. This creates a controlled "gap" that effectively lengthens the entire unit without completely severing the mechanical linkage.
Clinical Pearl: The primary biomechanical advantage of fractional lengthening over step-cut (Z-plasty) lengthening is the preservation of the muscle's inherent tension-generating capacity. Because the muscle fibers themselves are not transected, the risk of over-lengthening and subsequent devastating extension deformities is significantly mitigated.
PREOPERATIVE EVALUATION AND PATIENT SELECTION
Thorough preoperative assessment is critical to differentiate between dynamic spasticity and fixed myostatic contracture.
- Dynamic Spasticity: Characterized by increased tone that yields to slow, sustained passive stretching. Often responsive to chemodenervation (Botox) and splinting.
- Fixed Contracture: Characterized by structural shortening of the muscle-tendon unit and joint capsule, which does not yield to passive stretching. This is the primary indication for surgical lengthening.
Surgeons must carefully evaluate the contribution of each muscle group. The Volkmann angle (the angle of wrist flexion at which the fingers can be fully extended) should be measured to quantify the severity of the flexor tightness. Diagnostic nerve blocks (e.g., median or ulnar nerve blocks at the elbow) can temporarily abolish dynamic spasticity, unmasking the true extent of the fixed contracture.
SURGICAL TECHNIQUE: FRACTIONAL LENGTHENING OF THE FCR AND FINGER FLEXORS
The following technique details the fractional lengthening of the flexor carpi radialis, with concurrent lengthening of the finger flexors as dictated by the preoperative deformity.
Positioning and Setup
- The patient is placed supine on the operating table with the affected upper extremity extended on a radiolucent hand table.
- A well-padded pneumatic tourniquet is applied to the proximal arm.
- The limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to the appropriate pressure (typically 250 mm Hg or 100 mm Hg above systolic blood pressure).
- Loupe magnification (2.5x to 3.5x) is highly recommended to ensure precise identification of the aponeurosis and protection of adjacent neurovascular structures.
Incision and Exposure
- Begin by designing a curved volar incision over the distal forearm.
- The incision should start approximately 3 cm proximal to the volar wrist crease and extend proximally for about 6 cm. A slightly curved or lazy-S incision prevents the formation of a restrictive linear scar across the flexion crease of the forearm.
- Dissect through the subcutaneous tissue, taking meticulous care to identify and retract the palmar cutaneous branch of the median nerve, which typically lies between the FCR and the palmaris longus (PL).
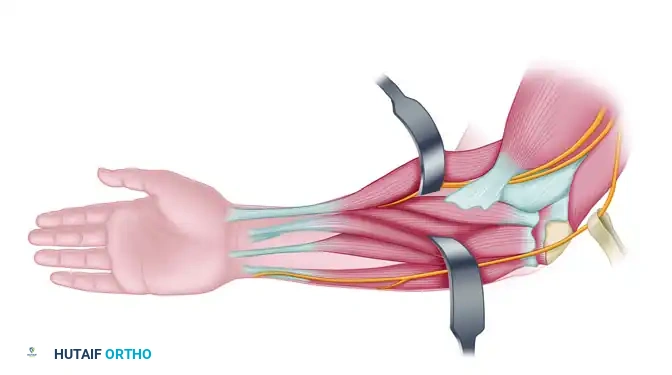
Identification of the Musculotendinous Junction
- Identify the flexor carpi radialis (FCR) muscle.
- Trace the FCR proximally from its tendinous portion at the wrist up to the musculotendinous junction, continuing further proximally until the distinct muscle belly is fully visualized.
- Observe the anatomy: The distal portion of the muscle belly is surrounded by a distinct aponeurosis that thickens distally, eventually coalescing to form the true tendon of the muscle.
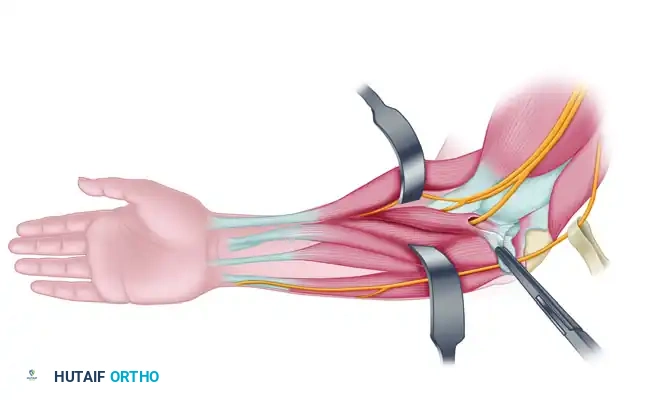
The Lengthening Procedure
- The objective is to lengthen the muscle-tendon unit while leaving it in absolute continuity.
- Completely identify the FCR muscle circumferentially. Use a blunt instrument (such as a Freer elevator or a right-angle forceps) to gently separate the muscle from the underlying structures, ensuring no neurovascular elements are tethered.
- Make a precise transverse cut through the aponeurosis proximal to the musculotendinous junction.
Surgical Warning: You must cut only through the aponeurosis and not through the underlying red muscle fibers. However, it is equally critical to divide the aponeurosis completely from medial to lateral. If even a small band of the tendinous aponeurosis is left intact, the muscle-tendon unit will fail to lengthen.
- After the transverse cut in the aponeurosis is completed, passively place the wrist into maximal dorsiflexion.
- As the wrist is extended, observe the transverse cut in the aponeurosis widen. The underlying muscle fibers will stretch, allowing the unit to lengthen while remaining structurally intact.
- If the desired length is not achieved with a single cut, a second transverse cut (recession) may be made approximately 1.5 to 2 cm proximal to the first cut.
Addressing Additional Contracted Units
In the spastic upper extremity, contractures are rarely isolated to a single muscle.
* Palmaris Longus (PL): Frequently spastic and contracted. It may require lengthening in the exact same fractional manner, or it may be simply tenotomized if it is severely contracted and non-functional.
* Finger Flexors: Through the same volar incision, the finger flexors can be accessed and lengthened.
* First, identify and lengthen the flexor digitorum superficialis (FDS) muscles.
* If contracture persists after FDS lengthening, proceed to lengthen the flexor digitorum profundus (FDP) muscles.
* Ensure that the median nerve, which runs deep to the FDS and superficial to the FDP, is identified and protected throughout this deeper dissection.
SURGICAL TECHNIQUE: THE FLEXOR SLIDE (INGLIS AND COOPER)
For patients with severe, global spastic flexion contractures of the wrist and fingers—often accompanied by severe pronation deformities—a simple fractional lengthening may be insufficient. In these advanced cases, a proximal flexor slide (the Inglis and Cooper technique) is indicated. This procedure releases the entire flexor-pronator origin from the medial epicondyle, allowing the entire muscle mass to slide distally.
Incision and Ulnar Nerve Management
- Incision: Begin the incision on the medial aspect of the volar side of the arm, starting approximately 5 cm proximal to the medial epicondyle. Continue the incision distally, crossing the elbow joint, to the midpoint of the forearm over the ulna (Figure 72-7 A).
- Elevate thick fasciocutaneous flaps to expose the medial epicondyle, the cubital tunnel, and the proximal flexor-pronator mass.

- Ulnar Nerve Identification: The ulnar nerve must be identified early in the procedure. Locate it proximal to the cubital tunnel and trace it distally.
- Release the ulnar nerve completely from the cubital tunnel by dividing the Osborne ligament and the arcuate ligament of the flexor carpi ulnaris (FCU). The nerve must be meticulously protected with a vessel loop (Figure 72-7 B).
Release of the Flexor-Pronator Origin
- With the ulnar nerve protected, direct attention to the medial epicondyle.
- Tendinous Release: Sharply incise the tendinous origins of the flexor-pronator muscles directly off the medial epicondyle.
- The flexor carpi ulnaris (FCU) and the flexor digitorum profundus (FDP) muscles must be completely released from their origins on the medial epicondyle and the proximal ulna (Figure 72-7 C).
- Use a periosteal elevator to strip the muscle origins distally. The extent of the distal stripping dictates the amount of lengthening achieved.
Division of the Lacertus Fibrosus and Nerve Transposition
- To ensure a complete and unhindered slide of the muscle mass, the lacertus fibrosus (bicipital aponeurosis) must be divided.
- Release any remaining tethering portions of the flexor muscle origin.
- Once the flexor mass has been allowed to slide distally, the ulnar nerve will be under tension if left in its anatomical bed. Therefore, the ulnar nerve must be transposed anteriorly into a well-vascularized subcutaneous bed to prevent traction neuritis and postoperative neuropathy.
- Extend the wrist and fingers to confirm that the flexor mass slides distally by the required amount (often 3 to 4 cm) and that the contracture is fully resolved.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of both fractional lengthening and the flexor slide is heavily dependent on rigorous, well-managed postoperative care. The newly lengthened muscle-tendon units are vulnerable to rupture or recurrent contracture if not properly splinted and rehabilitated.
Phase I: Immobilization (Weeks 0 to 4)
- Immediately postoperatively, the limb is placed in a well-padded palmar (volar) short-arm splint (or a long-arm splint if a flexor slide was performed).
- The wrist is positioned in a neutral position or slightly extended (10 to 15 degrees of dorsiflexion). The fingers are placed in functional extension.
- Crucial Note: Avoid extreme hyperextension, as this can place excessive tension on the healing aponeurotic gaps, leading to muscle rupture or severe pain.
- This rigid immobilization is maintained continuously for 3 to 4 weeks to allow the aponeurotic gaps to fill with organized, resilient scar tissue.
Phase II: Mobilization and Protection (Weeks 4 to 8)
- At 3 to 4 weeks, the rigid surgical splint is removed.
- Active and active-assisted mobilization of the wrist and digits is initiated under the strict guidance of a specialized hand therapist.
- A custom-molded removable thermoplastic splint is fabricated. This splint is worn at all times for protection, except during designated therapy sessions and hygiene routines.
- Therapy focuses on tendon gliding exercises, maintaining the newly acquired extension, and re-educating the antagonist extensor muscles, which are often profoundly weak due to prolonged preoperative overstretching.
Phase III: Long-Term Maintenance (Months 2 to 6+)
- Daytime splinting is gradually weaned as active motor control and dynamic balance improve.
- A volar short-arm night splint must be utilized for an additional 4 to 6 months.
- Night splinting is absolutely critical. During sleep, the resting tone of the flexors can cause the immature scar tissue at the lengthening sites to contract, leading to a rapid recurrence of the deformity.
COMPLICATIONS AND PITFALLS
While highly effective, fractional lengthening and flexor slides carry specific surgical risks that the orthopaedic surgeon must actively mitigate:
- Inadequate Lengthening: Occurs if the aponeurosis is not completely divided from edge to edge during fractional lengthening. Even a 1 mm intact band will prevent the muscle from sliding.
- Over-Lengthening: Results from cutting too deeply into the muscle belly during fractional lengthening, or stripping the flexor origin too far distally during a flexor slide. This results in a devastating loss of grip strength and a potential iatrogenic extension deformity.
- Nerve Injury: The palmar cutaneous branch of the median nerve is at high risk during the volar forearm incision. During the flexor slide, failure to transpose the ulnar nerve anteriorly will almost certainly result in traction neuritis as the muscle mass shifts distally.
- Recurrence of Contracture: The most common long-term complication, almost exclusively due to non-compliance with the prolonged 4-to-6-month night splinting protocol.
By adhering to precise anatomical dissection, respecting the biomechanics of the aponeurotic sleeve, and enforcing strict postoperative splinting, surgeons can achieve excellent, durable outcomes in the management of spastic upper extremity contractures.
You Might Also Like