Treating Tumors of the Foot: Optimizing Amputation & Resection

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Treating Tumors of the Foot: Optimizing Amputation & Resection. Malignant tumors of the foot present significant challenges for orthopedic oncologists due to the foot's complex anatomy and function. Complete resection can be difficult, often leading to amputation as a treatment. Tumors distal to the metatarsophalangeal joint may allow for amputation with minimal functional disruption, though preserving the first ray is crucial for optimal weight-bearing and function.
Introduction and Epidemiology
Malignant tumors of the foot present a formidable and highly specialized challenge to the orthopaedic oncologist. This complexity arises from the foot's unique bipedal weight-bearing function and its dense, interconnected anatomic peculiarities. Both osseous and soft tissue structures contribute to the dynamic stability of the foot, compartmentalized into tight, compact spaces traversed by intricate neurovascular bundles.
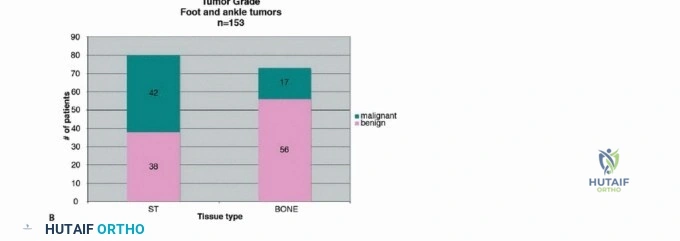
Complete resection, such as wide local excision of osseous structures, is inherently difficult due to the mandatory interruption of these complex anatomic relationships. Attempting limb-sparing wide resections often compromises the inherent stability of the foot, leading to profound functional deficits. Consequently, while malignant tumors of the bone are rare in the foot—and exceptionally rare distal to the metatarsophalangeal (MTP) joints—many of these aggressive lesions necessitate surgical amputation rather than limb salvage to achieve negative oncologic margins.
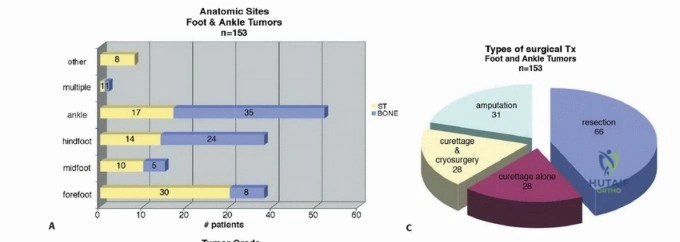
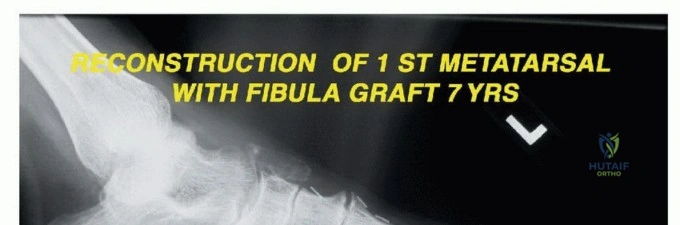
In high-volume orthopaedic oncology centers, amputations remain a cornerstone of definitive surgical management. For instance, in a large institutional series of 153 foot and ankle tumors, 31 required amputation to achieve local control. Fortunately, tumors localized distal to the MTP joint can often be managed with disarticulation through the MTP joint, yielding minimal functional disruption. The critical exception is the first ray, which bears approximately 50% of the body's weight during the toe-off phase of the gait cycle. Preservation of the proximal phalanx of the hallux, whenever oncologically feasible, is paramount to optimizing postoperative biomechanics.
Primary tumors affecting the foot, including osteosarcomas, have a remarkably low incidence. Metastatic lesions to the foot are similarly rare, with the most common primary sources being lung, renal, and colorectal carcinomas.

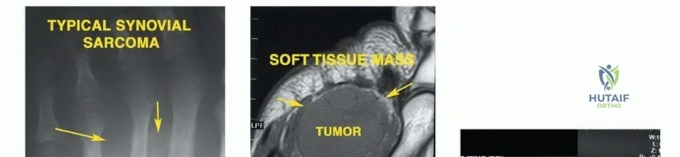
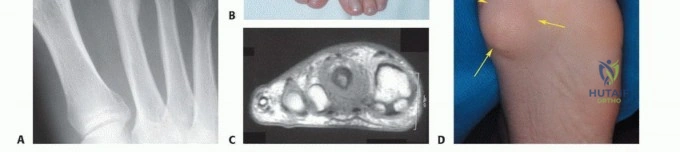
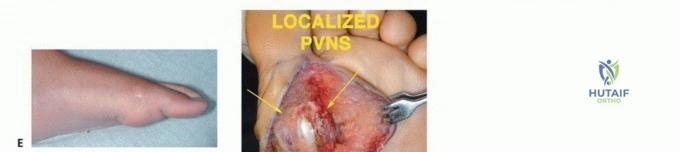
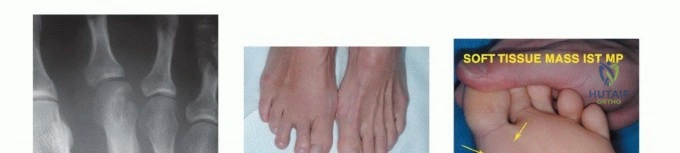
Soft tissue sarcomas (STS) of the foot, while also uncommon, present unique diagnostic and therapeutic dilemmas. Synovial sarcoma is disproportionately represented in the distal extremities, particularly the foot and ankle, often affecting young adults. These lesions are frequently misdiagnosed initially as benign entities such as ganglion cysts or plantar fasciitis due to their slow growth and occasionally indolent radiographic appearance. Clear cell sarcoma, historically termed melanoma of soft parts, also exhibits a predilection for the foot and ankle aponeuroses. For primary bone tumors, chondrosarcoma is the most frequently encountered malignancy in the adult foot, typically localizing to the calcaneus or midfoot, whereas Ewing sarcoma and osteosarcoma are more prevalent in the pediatric and adolescent populations.
Surgical Anatomy and Biomechanics
A profound understanding of foot biomechanics is required when planning oncologic resections. The foot is uniquely adapted for bipedal motion, functioning essentially as a dynamic tripod. This tripod is formed by the first ray medially, the fifth ray laterally, and the calcaneus posteriorly. These pillars are supported by the midfoot's osseous configuration, which forms a "Roman arch"—a structure that is inherently stable under axial loads. Ligamentous complexes and dynamic tendinous insertions further preserve this arch and facilitate propulsion.

Implications of Ray Resections
Resections involving the first and fifth rays predictably result in significant biomechanical alterations. Loss of the first ray eliminates the medial column's weight-bearing capacity and disrupts the windlass mechanism. The resulting forces are transferred to the lesser metatarsals, which are structurally ill-adapted to support the entire body weight, invariably leading to transfer metatarsalgia. These structural deficits can be partially mitigated through the judicious use of orthotics, such as medial heel wedges (to lateralize forces) or metatarsal bars (to distribute weight evenly across the lesser metatarsals).
Conversely, resection of the fifth ray is more easily compensated for with an orthosis that transfers forces medially, utilizing a lateral heel wedge. Resection of the middle rays (second, third, or fourth) generally results in insignificant functional loss and acceptable cosmesis, primarily causing a narrowing of the forefoot that is easily accommodated with standard shoe modifications.


Midfoot and Hindfoot Articulations
The Lisfranc joint (tarsometatarsal joint) serves as the critical transition point between the midfoot and the forefoot. The base of the second metatarsal acts as the keystone of this Roman arch, securely recessed between the medial and lateral cuneiforms. Oncologic resections that violate the Lisfranc articulation or require removal of the second metatarsal base inherently destabilize the entire transverse arch, frequently necessitating complex arthrodesis or progressing to midfoot amputation to maintain a functional limb.
Proximal to the Lisfranc joint lies the Chopart joint (transverse tarsal joint), comprising the talonavicular and calcaneocuboid articulations. This joint complex is responsible for the transition between the flexible, shock-absorbing foot of early stance phase and the rigid lever arm required for the toe-off phase. Amputations at the Chopart level preserve the tibiotalar and subtalar joints but eliminate the insertions of the anterior compartment dorsiflexors, predictably resulting in a severe equinovarus deformity driven by the unopposed pull of the Achilles tendon and tibialis posterior, unless meticulous tendon transfers are performed concurrently.
Compartmental Anatomy and Oncologic Barriers
The foot is divided into nine distinct fascial compartments: the medial, superficial, lateral, adductor, four interosseous compartments, and the calcaneal compartment. Unlike the thigh or leg, where thick muscular septa provide robust barriers to tumor extension, the compartments of the foot are small, tightly packed, and separated by thin fascial layers that offer minimal resistance to aggressive sarcomas.
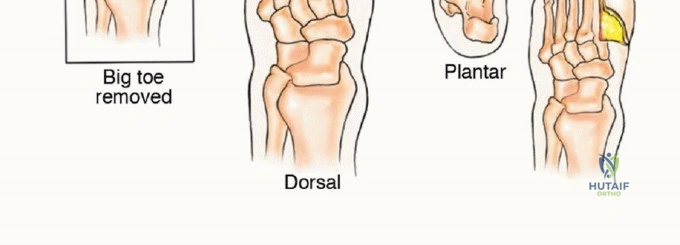
The plantar aponeurosis acts as a strong inferior barrier, but dorsal tumor extension easily tracks along the neurovascular bundles and tendon sheaths. The medial and lateral plantar nerves and vessels traverse these compartments, meaning that a tumor arising in the central compartment frequently contaminates the primary neurovascular supply to the plantar aspect of the foot. When a sarcoma encases these structures, limb-sparing resection typically requires en bloc excision of the neurovascular bundle, resulting in an insensate plantar flap—an absolute contraindication to limb salvage due to the high risk of subsequent neuropathic ulceration, infection, and secondary amputation.
Indications and Contraindications
The decision algorithm for treating foot tumors hinges on balancing oncologic control with functional outomes. The primary goal of any orthopaedic oncology procedure is the complete eradication of the tumor with negative margins. If limb salvage compromises this goal, amputation is mandatory.
When evaluating a patient for limb-sparing surgery versus amputation, the surgeon must consider the anatomic location, tumor histology, staging, and the expected functional morbidity of the reconstruction.
| Clinical Scenario | Operative Management | Rationale and Oncologic Principles |
|---|---|---|
| High-grade sarcoma encasing plantar neurovascular bundle | Below Knee Amputation (BKA) or Syme Amputation | Limb salvage would yield an insensate, non-functional foot prone to neuropathic ulceration. |
| Low-grade chondrosarcoma of the 3rd metatarsal | Central Ray Resection | Wide margins achievable without compromising the medial/lateral columns. Excellent functional prognosis. |
| Synovial sarcoma of the dorsal midfoot, small (<3cm) | Wide Local Excision + Adjuvant Radiation | Extensor tendons may be sacrificed and reconstructed. Plantar sensation remains intact. |
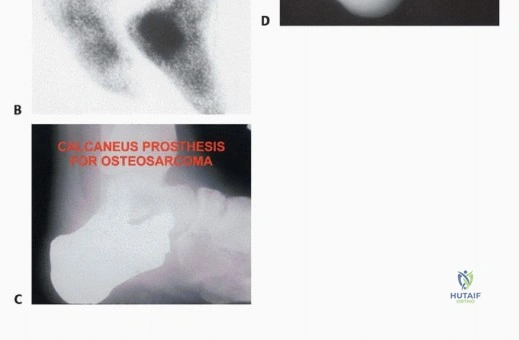
| Osteosarcoma of the calcaneus | BKA | Calcanectomy yields poor functional outcomes and high local recurrence rates for high-grade osseous malignancies. |
| Metastatic renal cell carcinoma to the talus with intractable pain | Palliative Talectomy or Radiotherapy | Focus is on immediate pain relief and early mobilization in the setting of systemic disease. |
| High-grade sarcoma of the first ray with clear proximal margins | First Ray Amputation / Transmetatarsal Amputation | Sacrifice of the first ray requires significant orthotic compensation but preserves a sensate heel and midfoot. |


Contraindications to Limb Salvage
Absolute contraindications to limb salvage in the foot include:
1. Inability to achieve negative oncologic margins without sacrificing the primary neurovascular supply (resulting in an insensate plantar surface).
2. Major vascular encasement precluding reconstruction in a patient with baseline peripheral vascular disease.
3. Massive tumor size resulting in a lack of adequate soft tissue coverage, where free flap reconstruction is not viable or oncologically sound.
4. Intractable infection or fungating tumor mass.
Relative contraindications include poor baseline functional status, severe medical comorbidities precluding prolonged reconstructive surgeries, and tumors involving the hindfoot (calcaneus/talus) where functional outcomes of partial amputations or massive endoprosthetic reconstructions are historically inferior to a well-fitted below-knee prosthesis.


Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful oncologic surgery. Advanced imaging is mandatory. Magnetic Resonance Imaging (MRI) with and without intravenous contrast of the entire foot and ankle is the gold standard for defining intra- and extra-compartmental extension, neurovascular involvement, and joint contamination. Computed Tomography (CT) of the foot provides essential details regarding cortical destruction and occult osseous involvement not readily apparent on MRI.
Systemic staging must be completed prior to any surgical intervention. For soft tissue sarcomas, a high-resolution CT of the chest is required to rule out pulmonary metastases. For osseous malignancies like osteosarcoma or Ewing sarcoma, a whole-body PET/CT or technetium-99m bone scan is indicated.
Biopsy Principles
The biopsy is the most critical initial step and must be meticulously planned. A poorly executed biopsy can contaminate vital neurovascular structures or previously uninvolved compartments, converting a potential limb salvage candidate into an obligate amputee.
* Incision Orientation: Biopsy incisions in the foot must be strictly longitudinal. Transverse incisions contaminate wider swaths of soft tissue and complicate future flap designs.
* Placement: The biopsy tract must be placed within the planned definitive resection margin. If an amputation is a possibility, the biopsy tract must be located distal to the planned amputation flaps.
* Hemostasis: Meticulous hemostasis is required to prevent post-biopsy hematoma, which carries tumor cells and biologically contaminates adjacent tissues. Drains should generally be avoided, but if absolutely necessary, they must exit in line with the surgical incision.
Patient Positioning and Preparation
Patients are typically positioned supine on a radiolucent operating table to facilitate intraoperative fluoroscopy. A bump under the ipsilateral hip is utilized to internally rotate the leg, bringing the foot into a neutral position, particularly useful for lateral approaches.
Tourniquet use is standard to maintain a bloodless surgical field, which is critical for identifying precise anatomic planes and oncologic margins. However, exsanguination via Esmarch bandage is strictly contraindicated in the setting of malignancy, as the compressive forces can theoretically embolize tumor cells into the systemic circulation. Instead, the limb should be elevated for 3 to 5 minutes to allow for gravity exsanguination before tourniquet inflation.

Detailed Surgical Approach and Technique
The surgical technique dictates the functional outcome and oncologic success. The following sections detail the specific approaches for varying levels of resection and amputation in the foot.
Ray Resections
Ray resections are utilized for lesions strictly confined to a single metatarsal and its corresponding phalanges.
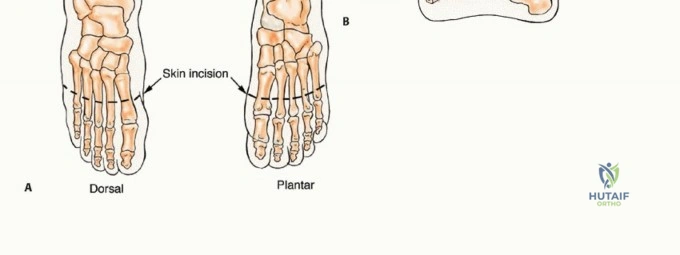
* First Ray Resection: A racquet-shaped incision is made encompassing the first MTP joint, extending proximally along the medial border of the first metatarsal. The internervous plane is generally not applicable as the dissection is subperiosteal (for benign lesions) or extra-periosteal (for malignancies). For sarcomas, a cuff of normal muscle (abductor hallucis, flexor hallucis brevis) must be taken en bloc with the bone. The osteotomy is performed at the metatarsal base or cuneiform articulation.
* Central Ray Resection: A dorsal longitudinal incision is preferred. The extensor tendons are retracted or resected depending on tumor proximity. The interosseous muscles adjacent to the affected ray are resected en bloc. Following removal of the ray, the adjacent metatarsals are approximated using heavy non-absorbable sutures through drill holes in the metatarsal necks to close the dead space and narrow the forefoot, improving postoperative shoe fit.

Transmetatarsal Amputation (TMA)
The TMA is a highly functional amputation level for extensive forefoot tumors. The goal is to preserve a robust plantar flap for weight-bearing.
1. Incision: A fish-mouth incision is utilized. The dorsal incision is made directly over the planned osteotomy sites. The plantar incision extends distally to the metatarsal necks to maximize the plantar fascial and myocutaneous flap.
2. Dissection: The dorsal structures are transected sharply. The metatarsals are exposed extra-periosteally.
3. Osteotomies: The metatarsals are transected using an oscillating saw. A critical technical pearl is to bevel the osteotomies from dorsal-proximal to plantar-distal. This prevents a sharp plantar bony prominence that would otherwise cause pressure ulcerations against the plantar flap. The metatarsals should also be cut in a gentle cascade, with the first metatarsal being the longest and the fifth the shortest, mimicking the natural transverse arch.
4. Nerve Management: The digital nerves must be identified, drawn distally under tension, and sharply transected to allow them to retract deep into the proximal soft tissues, minimizing the risk of symptomatic terminal neuromas. Targeted Muscle Reinnervation (TMR) can be considered by coapting these nerve stumps to motor branches of the intrinsic foot musculature.


Lisfranc and Chopart Amputations
Midfoot amputations are technically demanding due to the severe biomechanical imbalances they create.
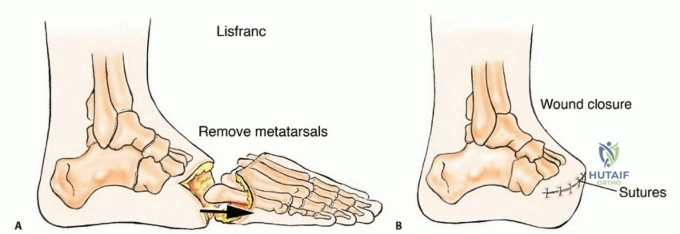
* Lisfranc Disarticulation: This involves disarticulation at the tarsometatarsal joints. The primary complication is an equinovarus deformity due to the loss of the anterior tibial (dorsiflexion) and peroneus brevis (eversion) insertions, while the Achilles tendon and tibialis posterior remain unopposed. To prevent this, the tibialis anterior tendon must be meticulously mobilized and transferred to the dorsal neck of the talus or the navicular. A concurrent percutaneous Achilles tendon lengthening (TAL) is often mandatory.
* Chopart Disarticulation: Disarticulation through the talonavicular and calcaneocuboid joints. The functional outcome is historically poor due to severe equinus contracture. If this level is chosen for oncologic reasons, aggressive tendon transfers (tibialis anterior to the talar neck) and rigid postoperative
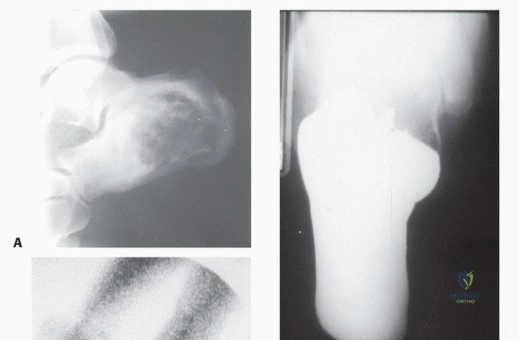
Clinical & Radiographic Imaging






