Surgical Management of Fixed Deformities and Charcot Arthropathy

Key Takeaway
Fixed deformities in the diabetic foot, combined with peripheral neuropathy, create high-pressure focal points that inevitably lead to ulceration. Surgical intervention, including Achilles tendon lengthening, metatarsal head resection, and corrective arthrodesis, is often required when conservative off-loading fails. In cases of Charcot neuropathic arthropathy, early recognition and total contact casting are paramount to prevent catastrophic midfoot collapse and preserve a plantigrade, ulcer-free foot.
FIXED DEFORMITIES IN THE DIABETIC FOOT
The management of the diabetic foot represents one of the most complex challenges in orthopedic surgery. An essential, yet frequently underestimated, element in the treatment of diabetic forefoot ulceration is the presence of a fixed bony deformity. It is exceedingly difficult to maintain soft-tissue healing—even when initially accomplished through off-loading or advanced wound care—if the underlying biomechanical fault remains uncorrected.
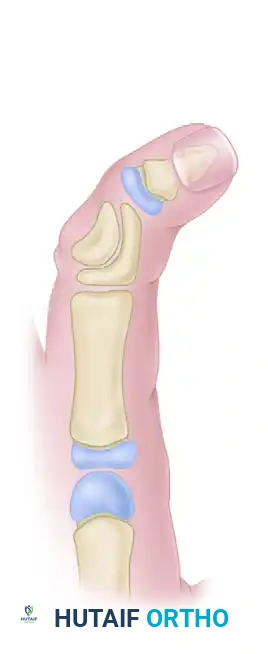
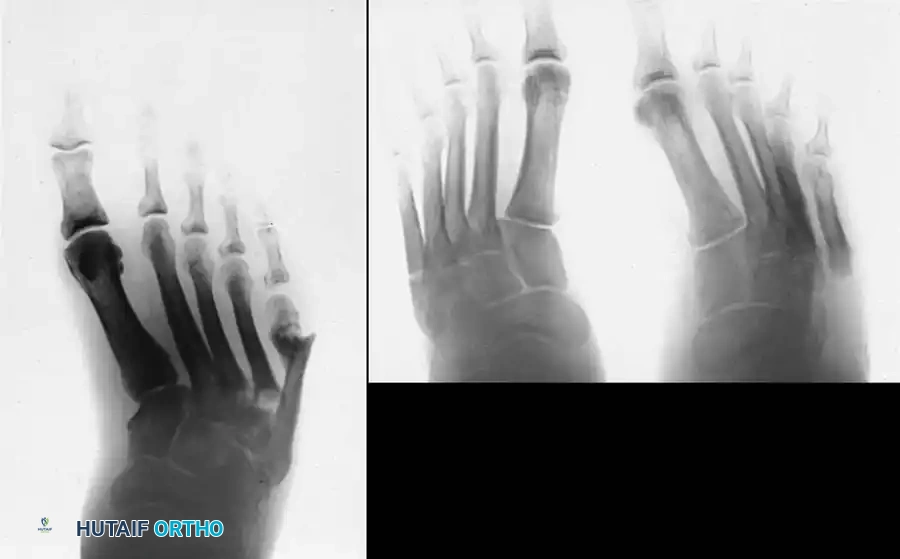
In the presence of motor neuropathy, the intrinsic musculature of the foot atrophies, leading to an intrinsic-minus foot posture. This results in the classic claw toe deformity: hyperextension at the metatarsophalangeal (MTP) joints and flexion at the proximal interphalangeal (PIP) joints. Consequently, the plantar fat pad is drawn distally, leaving the metatarsal heads prominent and unprotected against vertical and shear forces during the terminal stance phase of gait.
Surgical Correction of Forefoot Deformities
When conservative measures fail, surgical correction is mandated to prevent recurrent ulceration, deep space infection, osteomyelitis, and eventual amputation.
- Claw Toe Correction: Correction at the MTP and PIP joints is often necessary. This may involve extensor tendon lengthening, dorsal MTP capsulotomy, and PIP arthroplasty or arthrodesis.
- Hallux Interphalangeal Arthrodesis: Fixed flexion deformities of the hallux interphalangeal joint create massive pressure at the distal tip of the toe. Arthrodesis of this joint, often combined with extensor hallucis longus (EHL) lengthening, is highly effective.
- Metatarsal Head Resection: Resection of one or more prominent metatarsal heads (or a complete pan-metatarsal head resection in severe cases) may be required to relieve plantar pressure and maintain ulcer closure.


The Role of Achilles Tendon Lengthening
For recurrent plantar forefoot ulcerations caused by neuropathy in a foot with adequate vascularity, a percutaneous Achilles tendon lengthening (TAL) is arguably the single most effective intervention.
Biomechanical Pearl: A tight gastrocnemius-soleus complex forces the patient to "vault" over the forefoot during the stance phase of gait, exponentially increasing peak plantar pressures beneath the metatarsal heads. TAL restores adequate ankle dorsiflexion, neutralizing this vaulting mechanism.
When combined with proper postoperative orthoses—such as custom-molded inserts, rocker-bottom soles, or an ankle-foot orthosis (AFO)—TAL drastically decreases the recurrence rate of forefoot ulcerations.
The Autosympathectomized Foot
Diabetic autonomic neuropathy leads to an "autosympathectomized" foot. The loss of sympathetic tone results in a lack of sweating (anhidrosis), leaving the foot dry, scaly, and prone to fissuring.
Clinical Warning: No callus in the diabetic patient is innocent. A dry, insensitive foot with an unyielding hyperkeratotic lesion over a bony prominence is the immediate precursor to an ulcer.
Whether it is a "kissing lesion" in the web space, a corn over a PIP joint, an end-corn associated with a mallet toe, or a dense callus beneath a metatarsal head or sesamoid, all must be treated as preulcerative lesions. Routine callus debridement, bony prominence padding, daily application of emollients, and meticulous hygiene are mandatory preventative measures.
NEUROPATHIC (CHARCOT) ARTHROPATHY
Neuropathic osteoarthropathy, commonly known as Charcot arthropathy, is a devastating, progressive, and destructive joint disease. While historically associated with neurosyphilis (tabes dorsalis) and Hansen's disease (leprosy), the vast majority of cases encountered by modern orthopedic surgeons are secondary to diabetes mellitus.
Pathophysiology
The exact etiology of Charcot arthropathy remains a subject of debate, but it is generally accepted to be a combination of two primary theories:
1. Neurovascular (French) Theory: Autonomic neuropathy leads to a loss of sympathetic vascular control. This results in profound arteriovenous shunting and a hyperemic state. Resting blood flow may be up to five times normal. This hyperemia causes localized osteopenia, weakening the structural integrity of the bone.
2. Neurotraumatic (German) Theory: Somatosensory neuropathy deprives the patient of protective pain sensation and proprioception. The osteopenic foot is subjected to repetitive, unrecognized microtrauma during weight-bearing, leading to microfractures, ligamentous laxity, and eventual catastrophic joint collapse.
Clinical Presentation and Diagnosis
The hallmark physical clue to an underlying acute Charcot event is a red, hot, swollen foot that is usually out of proportion to any remembered injury.




Diagnostic Pitfall: The acute inflammatory stage of Charcot arthropathy is frequently misdiagnosed as cellulitis, deep vein thrombosis (DVT), or gout. A high index of suspicion is required. If a diabetic patient presents with unilateral erythema and edema, Charcot must be ruled out.
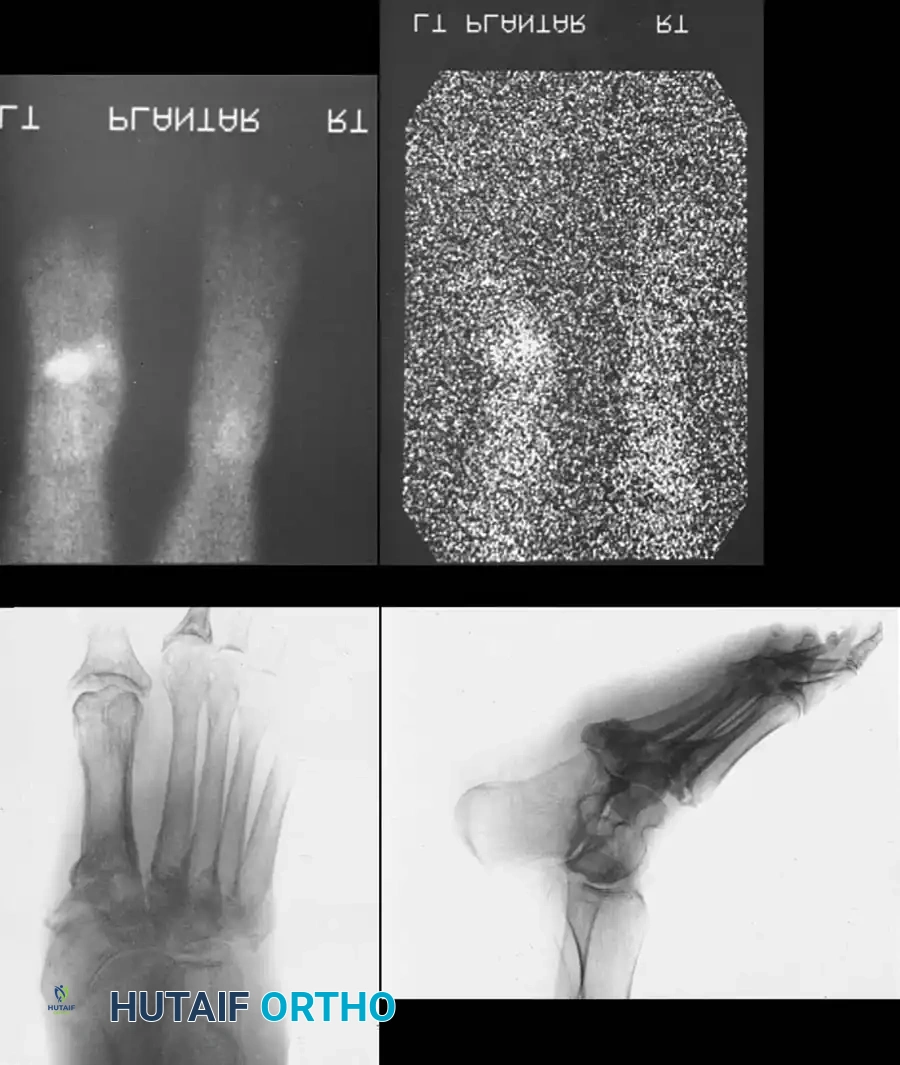
In the early stages, routine radiographs may appear entirely normal. A technetium-99m bone scan or MRI is highly sensitive and will be positive before radiographic destruction is visible. Indium-111 labeled white blood cell scans may be required to differentiate acute Charcot from osteomyelitis.
CLASSIFICATION OF CHARCOT ARTHROPATHY
The Eichenholz Staging System
Eichenholz provided a universally accepted classification system based on radiographic progression, which dictates the clinical management phase:
- Stage 0 (Prodromal): Unilateral edema, erythema, and warmth. Skin is intact. Radiographs are negative or show only localized osteopenia. MRI shows bone marrow edema.
- Stage I (Developmental/Fragmentation): Persistent clinical inflammation. Radiographs reveal osseous destruction, periarticular fragmentation, joint subluxation, or frank dislocation.
- Stage II (Coalescence): Clinical signs of inflammation begin to decrease. Radiographs demonstrate absorption of fine bone debris, early fusion of large fragments, and sclerosis.
- Stage III (Reconstruction/Consolidation): Resolution of edema and erythema. Radiographs show consolidation, remodeling of fracture fragments, and rounding of bone ends. The foot is stable but often severely deformed.
Anatomical Classification (Brodsky/Trepman)
Charcot arthropathy is also classified by the anatomical location of the involved joints:
* Type 1 (Midfoot): Involves the tarsometatarsal (Lisfranc) and naviculocuneiform joints. This is the most common pattern, affecting approximately 60% of patients. It frequently results in a rocker-bottom deformity.
* Type 2 (Hindfoot): Involves the subtalar, talonavicular, or calcaneocuboid (Chopart) joints. Requires prolonged immobilization and is highly unstable.
* Type 3A (Ankle): Involves the tibiotalar joint. Rapidly progressive and highly destructive.
* Type 3B (Calcaneus): Pathological fracture of the calcaneal tuberosity.



NON-OPERATIVE MANAGEMENT
The cornerstone of treatment for acute (Stage 0, I, and early II) Charcot arthropathy is strict off-loading and immobilization.
Total Contact Casting (TCC) is the gold standard. The goal is to maintain stability, arrest the inflammatory cascade, and prevent further architectural collapse.
* During the initial highly edematous phase, the cast must be changed frequently (every 1 to 2 weeks). As swelling rapidly subsides, a loose cast will cause pistoning, leading to iatrogenic shear ulcers.
* Immobilization must continue until the foot transitions to Eichenholz Stage III (clinical quiescence and radiographic consolidation). This process routinely takes 4 to 12 months, with proximal joint involvement requiring the longest durations.
Once stable, the patient is transitioned to a Charcot Restraint Orthotic Walker (CROW) or custom-molded extra-depth shoes with rigid rocker-bottom soles.
SURGICAL RECONSTRUCTION OF THE CHARCOT FOOT
Surgery in the Charcot foot is fraught with complications and should not be undertaken lightly. The host bone is often profoundly osteopenic, making rigid internal fixation difficult. Furthermore, these patients frequently have significant comorbidities, including peripheral arterial disease and poor glycemic control, which compromise wound healing.
Indications for Surgery
- Severe, unbraceable deformity (e.g., rigid rocker-bottom foot).
- Recurrent ulceration over a bony prominence despite optimal orthotic management.
- Gross instability that precludes ambulation.
- Early Stage I midfoot dislocation (controversial, but increasingly accepted to prevent inevitable collapse).
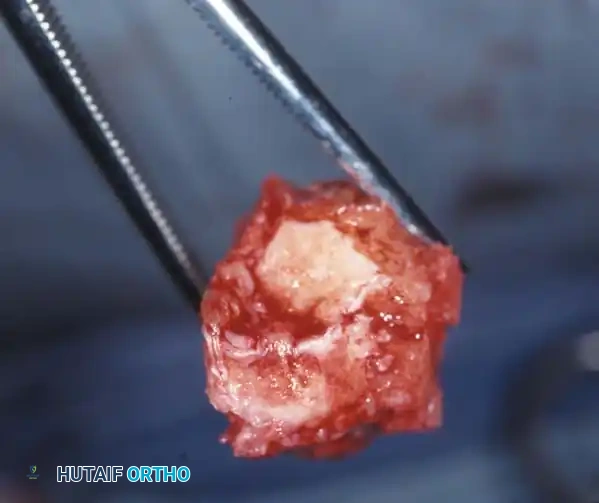
Exostectomy
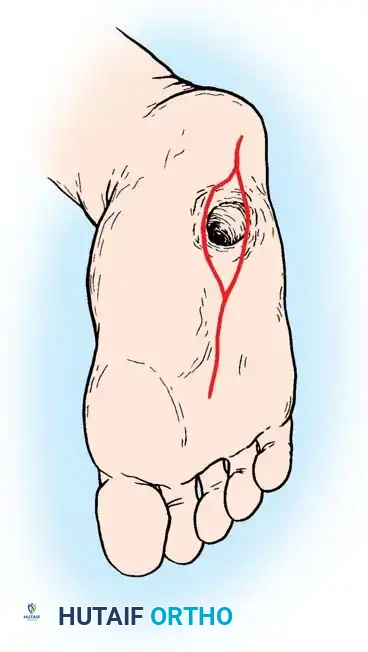
If an ulcer is driven purely by a localized bony prominence in an otherwise stable foot (Eichenholz Stage III), a simple exostectomy may suffice. The most common site is the plantar-medial aspect of the midfoot (prominent medial cuneiform or base of the first metatarsal). Care must be taken to resect enough bone to relieve pressure without violating the remaining stabilizing ligaments, which could trigger a secondary collapse.
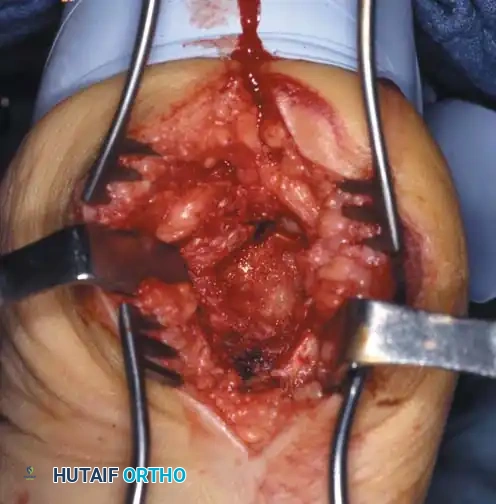
Arthrodesis and Realignment
When deformity correction is required, formal arthrodesis is performed. The goal is to create a plantigrade, stable, and braceable foot.
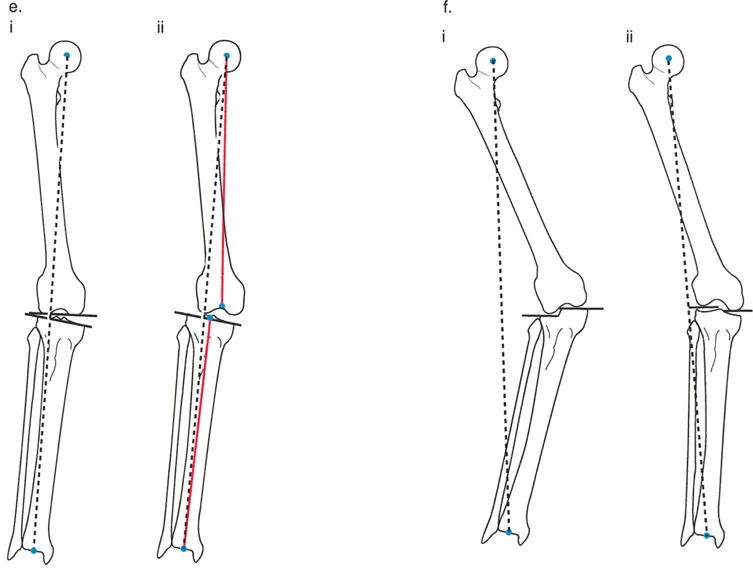
The Abducted Forefoot:
Lateral subluxation of the forefoot on the midfoot is the most common presentation of Type 1 Charcot. This produces an abducted forefoot, secondary hindfoot valgus, and a contracted Achilles tendon. Surgical correction involves a medial utility incision, resection of the destroyed TMT joints, realignment of the medial column, and rigid fixation using robust hardware (beaming screws, locking plates) or circular external fixation.


The Adducted Forefoot:
While less common, the adducted forefoot is notoriously difficult to treat. It is frequently precipitated by neuropathic fractures at the base of the fifth metatarsal. If the lateral column collapses and the forefoot adducts, massive pressure is transferred to the lateral border of the foot.
Surgical Warning: Simply excising the prominent fifth metatarsal base in an adducted Charcot foot is a critical error. It merely transfers the pressure apex proximally to the cuboid, leading to a new, more recalcitrant ulcer. Comprehensive realignment of the lateral column is required.



Early Intervention in Stage I Charcot
Historically, surgery was strictly contraindicated during the acute inflammatory phase (Stage I). However, modern paradigms suggest that if a frank dislocation at the tarsometatarsal joint is identified early—before extensive bony fragmentation and soft-tissue contracture occur—closed reduction and percutaneous pinning, or limited open reduction and primary arthrodesis, may be indicated. This proactive approach can prevent the devastating rocker-bottom collapse.




You Might Also Like