Mastering Posterior Plateau Fractures via Direct Posterior Approaches
Key Takeaway
Here are the crucial details you must know about Mastering Posterior Plateau Fractures via Direct Posterior Approaches. A direct posterior approach treats tibial plateau fractures via a prone patient position, allowing stable fixation of posterior aspect fractures. This method is ideal for fractures hard to visualize conventionally, especially fracture-dislocations of the knee, posteromedial, or posterior dominant bicondylar patterns, ensuring precise reduction and stabilization.
Introduction and Epidemiology
Tibial plateau fractures represent a complex spectrum of intra-articular injuries that challenge the orthopedic surgeon regarding both reduction and stable fixation. Historically, the vast majority of these injuries were approached via conventional anterolateral or extensile medial incisions. However, with the advent of advanced cross-sectional imaging, specifically computed tomography with three-dimensional reconstructions, the high prevalence of posterior column involvement has been increasingly recognized. Posterior plateau fractures, particularly coronal shear fragments, are inherently unstable and difficult to visualize, reduce, and adequately fixate from an anterior trajectory.


The direct posterior approach to the proximal tibia offers unparalleled access to the posterior articular segments. This approach allows for direct visualization of the fracture, anatomical reduction, and the application of posterior buttress plating, which is biomechanically superior for neutralizing vertical shear forces during knee flexion. The approach to the posterior aspect of the proximal tibia was originally described in the French surgical literature by Cadenat in 1933. Later, the approach was further described in the English literature by Darrach in 1945 and Harmon in 1945. Kaplan in 1946 provided an excellent description of the anatomy of the approach, although none of these early authors explicitly described the use of the posterior approach to the proximal tibia for fracture fixation.

More recently, Lobenhoffer et al in 2004 described a limited posterior approach for tibial plateau fracture fixation that has been popularized by subsequent authors. This approach uses the medial aspect and dissection of the extensile approach for the treatment of posteromedial tibial plateau fractures. Carlson subsequently added the posterolateral incision and dissection for the treatment of posterior dominant bicondylar fractures. These techniques are most applicable to fracture-dislocations of the knee, typically resulting from high-energy mechanisms such as motor vehicle collisions or severe axial loading in a flexed knee position.
Epidemiologically, posterior plateau fractures are rarely isolated. They frequently occur as components of bicondylar fractures (Schatzker V and VI) or as specific fracture-dislocation variants (Moore types I-IV). Recognizing the posterior fragment is paramount, as failure to appropriately buttress a posterior shear fragment inevitably leads to posterior subluxation of the femoral condyle, early post-traumatic arthrosis, and poor functional outcomes.

Surgical Anatomy and Biomechanics
Mastery of the direct posterior approach requires an intimate understanding of the popliteal fossa and the posterior neurovascular structures. Dissection and approach to the posterior aspect of the proximal tibia are performed primarily through three tissue planes medial, middle, and lateral, all of which are part of the extensile posterior approach.
Medial Tissue Plane
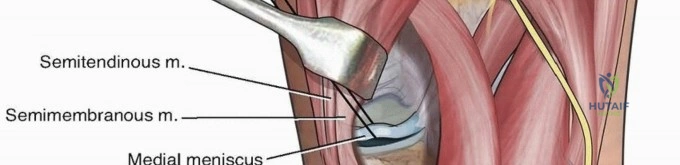
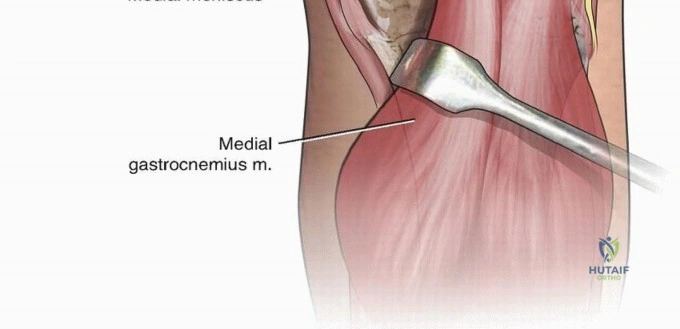
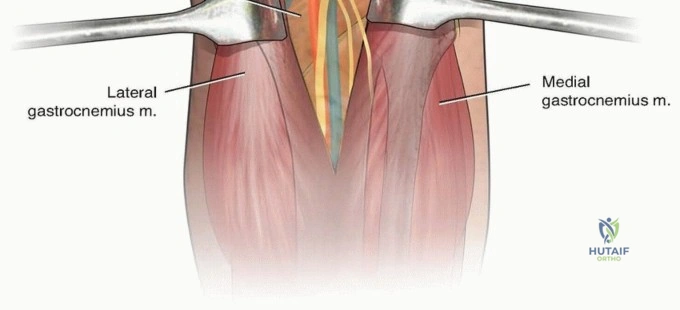
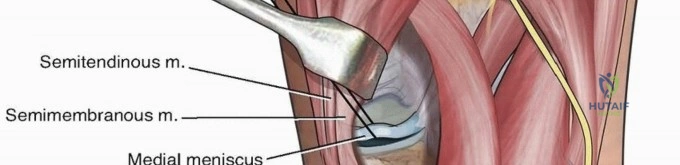
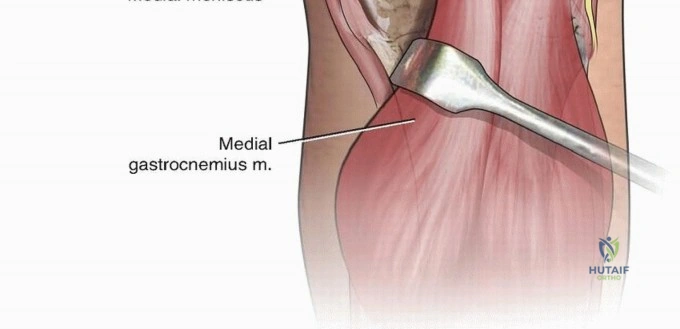
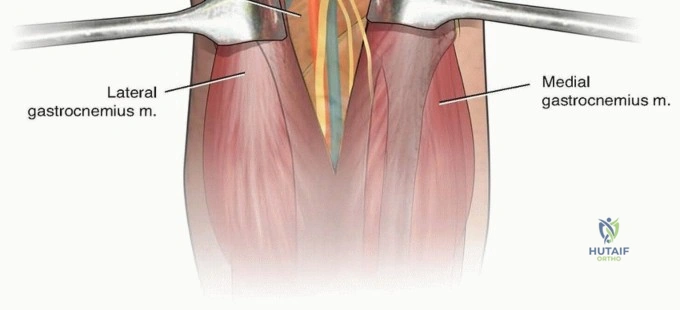
The medial tissue plane is utilized for the posteromedial approach. It is bounded superiorly by the semimembranosus muscle, laterally by the medial head of the gastrocnemius, and inferiorly by the soleus and popliteus muscles. Retraction of the medial head of the gastrocnemius laterally protects the midline neurovascular structures. During this dissection, the inferior medial geniculate neurovascular bundle is at significant risk. This bundle courses horizontally across the operative field and must be identified, protected, or selectively ligated if it impedes plate placement.

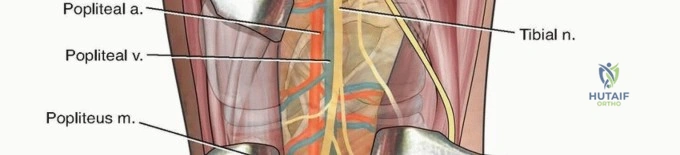
Middle Tissue Plane
The middle tissue plane involves direct mobilization of the neurovascular bundle. The popliteal artery is the deepest structure, tethered by its geniculate branches and the anterior tibial artery as it passes through the interosseous membrane. The popliteal vein lies superficial and slightly lateral to the artery, while the tibial nerve is the most superficial and lateral of the central structures. Accessing the central posterior plateau requires meticulous isolation and gentle retraction of these structures, typically utilizing vessel loops.



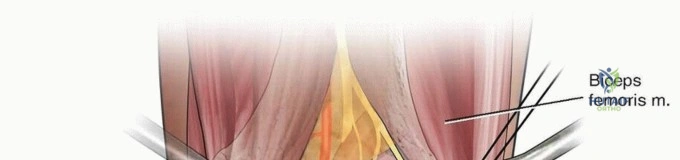
Lateral Tissue Plane
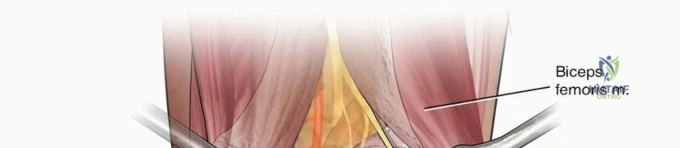
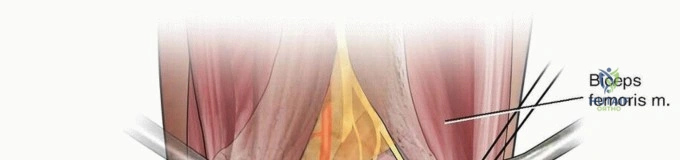
The lateral tissue plane provides access to the posterolateral plateau. This interval is developed between the lateral head of the gastrocnemius and the biceps femoris. The common peroneal nerve is the critical structure at risk here. It courses along the posterior border of the biceps femoris tendon before wrapping around the fibular neck. Identifying and neurolysing the common peroneal nerve is a mandatory early step in the posterolateral approach.

Biomechanical Considerations
Biomechanically, the posterior tibial plateau sustains significant compressive and shear forces during normal gait, particularly in early flexion. A posterior coronal fracture line creates a biomechanically unstable environment where the femoral condyle can slide posteriorly. Anterior-to-posterior lag screws placed via an anterior approach often fail to provide adequate resistance to these shear forces. A posterior buttress plate, applied directly to the apex of the fracture via a posterior approach, acts as an anti-glide construct, converting axial loads into compressive forces across the fracture site.


Indications and Contraindications
The decision to utilize a direct posterior approach hinges on fracture morphology, specifically the presence of a displaced posterior coronal fracture line that cannot be indirectly reduced or adequately stabilized with anteriorly based implants.


| Clinical Scenario | Operative Indication | Non-Operative Indication |
|---|---|---|
| Posteromedial Shear Fragment | Displacement > 3mm, articular step-off, or knee instability in flexion. Requires posteromedial buttress. | Non-displaced fractures with stable knee examination in full extension and flexion. |
| Posterolateral Shear Fragment | Displaced posterolateral fragment with lateral meniscal entrapment or subluxation. | Minimally displaced fragments without mechanical block or instability. |
| Bicondylar Fractures | Posterior dominant bicondylar fractures requiring dual posterior plating. | Severe medical comorbidities precluding prone positioning (relative). |
| Fracture-Dislocations | Moore type fracture-dislocations with posterior subluxation of the tibia. | N/A - Highly unstable, mandates surgical stabilization. |


Contraindications
Absolute contraindications include severe vascular injuries requiring immediate anterior arterial bypass, although posterior vascular injuries may actually be addressed through this same exposure. Relative contraindications encompass severe polytrauma where prone positioning compromises hemodynamic or respiratory stability. In such cases, a lateral decubitus or floating position may be considered as an alternative. Furthermore, compromised posterior soft tissue envelopes (e.g., severe Morel-Lavallée lesions or open posterior wounds) necessitate caution and potential delay of definitive internal fixation.

Pre Operative Planning and Patient Positioning
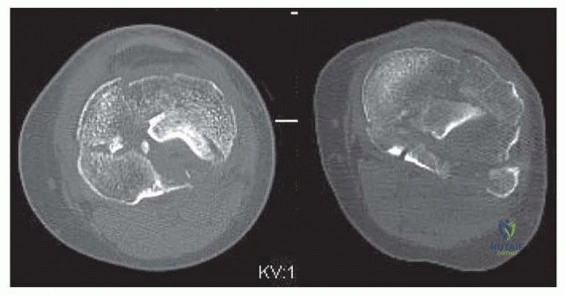
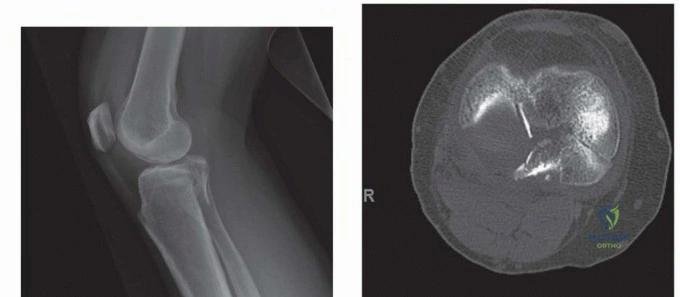
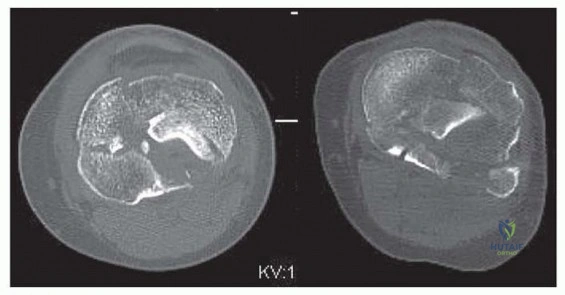
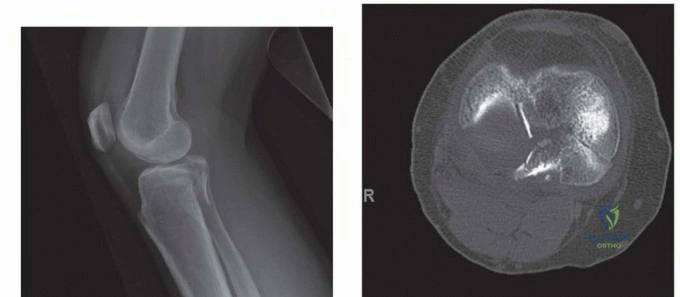
Thorough preoperative planning is the cornerstone of successful posterior plateau fixation. Standard anteroposterior and lateral radiographs are insufficient for complete characterization. A fine-cut computed tomography scan with sagittal, coronal, and 3D reconstructions is mandatory to delineate the size, location, and comminution of the posterior fragments. The surgeon must map the fracture lines to determine whether a posteromedial, posterolateral, or extensile midline approach is required.


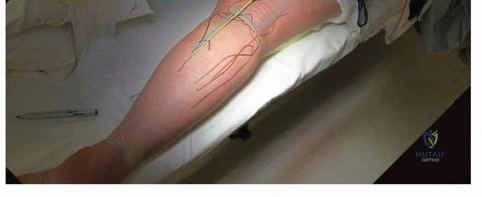
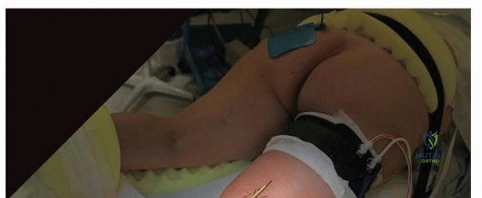
Patient Positioning
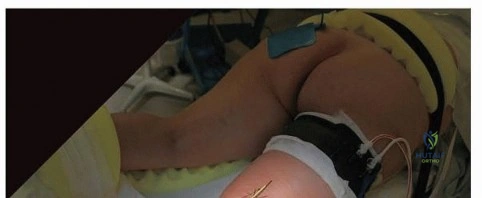
The patient is typically placed in the prone position on a radiolucent Jackson table or a standard operating table with chest and pelvic rolls to allow for abdominal excursion. The operative extremity should be prepped and draped free to allow for full knee flexion and extension. A sterile tourniquet is applied to the proximal thigh.

Fluoroscopy positioning is critical. The C-arm should be brought in from the contralateral side or from the head of the bed, depending on the table design. The surgeon must confirm that perfect AP and lateral fluoroscopic views can be obtained without obstruction before making the incision. Knee flexion is often utilized during the procedure to relax the posterior neurovascular structures and the gastrocnemius complex, facilitating deeper retraction.



Detailed Surgical Approach and Technique
The surgical technique varies based on the targeted quadrant of the posterior plateau. The approaches can be divided into posteromedial, posterolateral, and extensile central posterior.
The Posteromedial Approach
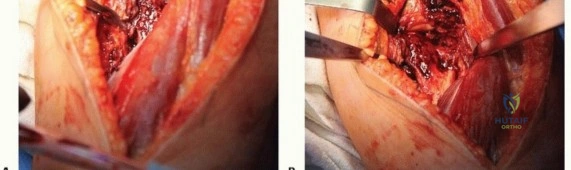
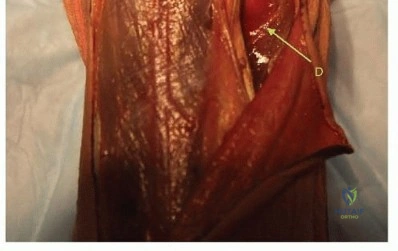
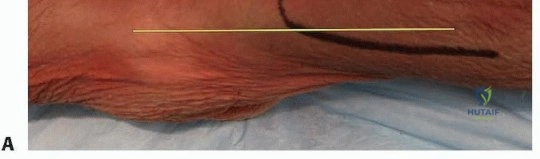
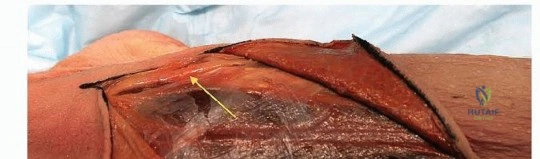
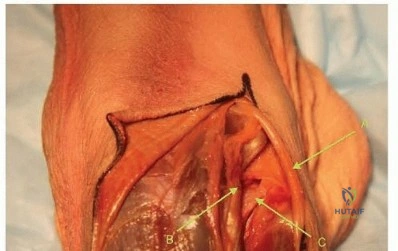
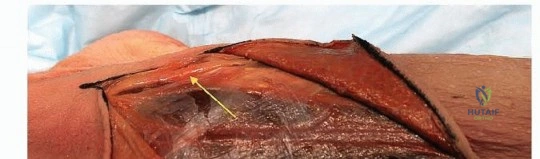
The posteromedial approach, as refined by Lobenhoffer, is the workhorse for posterior plateau fractures. An incision is made along the posteromedial border of the proximal tibia, starting at the level of the joint line and extending distally. The deep fascia is incised, and the pes anserinus tendons are identified and retracted anteriorly.


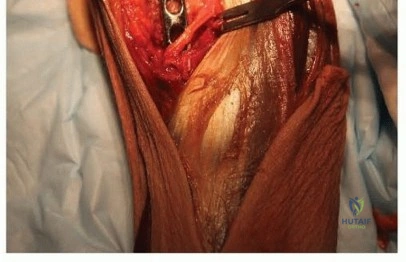
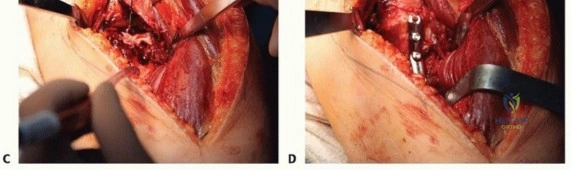
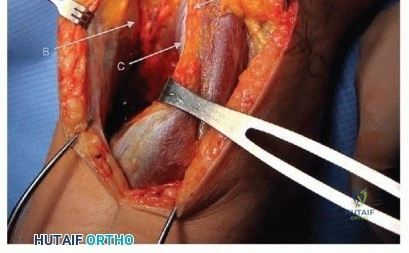
The medial head of the gastrocnemius is identified and mobilized laterally. This internervous plane protects the popliteal neurovascular bundle, which is swept laterally with the muscle belly. Deep to the gastrocnemius, the popliteus muscle is encountered. The popliteus is sharply elevated off the posterior tibia from medial to lateral. At this stage, the inferior medial geniculate artery is often encountered and may be ligated to permit full exposure of the posteromedial bony surface.

The Posterolateral Approach
Accessing the posterolateral corner is more challenging due to the presence of the common peroneal nerve and the fibular head. Carlson described a posterolateral approach utilizing an incision over the biceps femoris tendon. The common peroneal nerve is immediately identified posterior to the biceps tendon and carefully neurolysed.

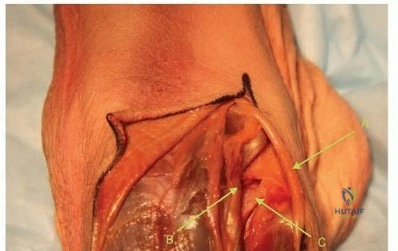
The interval between the lateral head of the gastrocnemius and the soleus is developed. Retracting the lateral gastrocnemius medially protects the central neurovascular bundle. The soleus is partially elevated from the posterior fibula and tibia.
Further modification of the posterolateral approach by adding an osteotomy of the proximal fibula has been described by Yu et al to improve exposure to the proximal posterolateral tibial plateau. The fibular osteotomy is performed horizontally or obliquely, allowing the fibular head and attached lateral collateral ligament to be retracted superiorly. In some circumstances, the fibular osteotomy comes as part of the fracture, and this can be exploited to improve fracture visualization without requiring an iatrogenic osteotomy.


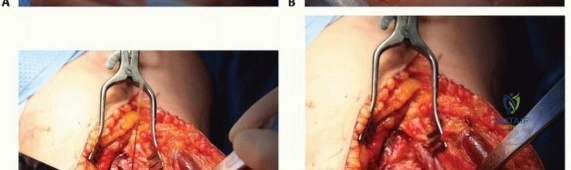
Fracture Reduction and Fixation Technique
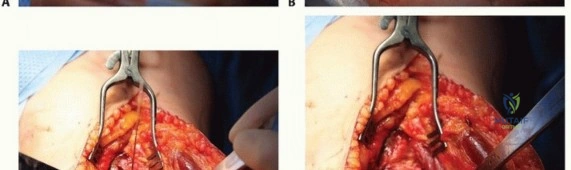
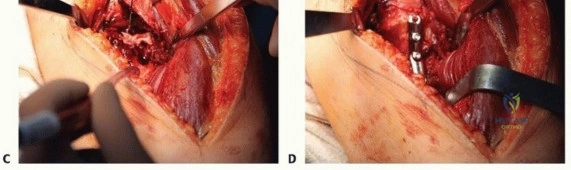
Once the fracture is exposed, a submeniscal arthrotomy is performed to visualize the articular surface. Hematoma and interposed soft tissues are debrided. Reduction is achieved through a combination of direct manipulation with dental picks, Schanz pins used as joysticks, and hyperextension of the knee to utilize the posterior capsule for ligamentotaxis.

Temporary fixation is achieved with smooth Kirschner wires. Articular congruity is confirmed visually and fluoroscopically. Definitive fixation relies on the application of a posterior buttress plate. The plate is slightly under-contoured to ensure that as the screws are tightened, the plate compresses the apex of the fracture, driving the articular segment superiorly and anteriorly into anatomical alignment. Small fragment (3.5 mm) T-plates, reconstruction plates, or anatomically pre-contoured posterior plateau plates are utilized.

For bicondylar fractures requiring staged management, the posterior approach can be combined with an anterolateral approach. However, it is hard to perform concurrently with an anterolateral tibial plateau approach in the prone position. Consequently, surgeons often fix the posterior column first, close the wound, and reposition the patient supine for the anterolateral fixation, or utilize a floating lateral decubitus position.

Complications and Management
The direct posterior approach carries distinct risks primarily related to the complex neurovascular anatomy of the popliteal fossa and the challenges of prone positioning. Meticulous surgical technique and a thorough understanding of the anatomical intervals are required to minimize these complications.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Neurovascular Injury | 1% - 3% | Avoid aggressive retraction of the central bundle. Flex the knee to reduce tension. If arterial injury occurs, obtain immediate vascular surgery consultation for repair or bypass. |
| Common Peroneal Nerve Palsy | 2% - 5% | Mandatory early identification and neurolysis in posterolateral approaches. Avoid rigid retractors on the lateral aspect of the fibular neck. Manage conservatively post-op with an AFO; most resolve within 6 months. |
| Wound Dehiscence / Infection | 3% - 7% | Avoid crossing the popliteal crease at a 90-degree angle; use S-shaped incisions. Ensure meticulous hemostasis and multilayer closure. Manage with targeted antibiotics and negative pressure wound therapy if required. |
| Loss of Fixation / Subsidence | 5% - 10% | Utilize rigid buttress plating. Avoid isolated lag screw fixation for shear fractures. If subsidence occurs, revision open reduction, structural bone grafting, and robust plating are indicated. |
| Joint Stiffness / Arthrofibrosis | 10% - 15% | Early range of motion is critical. Avoid prolonged immobilization. Consider manipulation under anesthesia or arthroscopic lysis of adhesions if flexion is < 90 degrees at 3 months. |
Careful handling of the soft tissues, particularly the muscular flaps used to protect the neurovascular bundle, is essential. At the conclusion of the procedure, a drain is often placed deep to the muscular fascia to prevent hematoma accumulation, which can lead to excessive tension on the posterior skin envelope or secondary nerve compression.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation must balance the need for early joint motion to prevent arthrofibrosis with the necessity of protecting the articular reduction and hardware construct.
Immediate postoperative protocols typically involve placing the patient in a hinged knee brace. Continuous passive motion (CPM) machines or early active-assisted range of motion exercises are initiated within the first 48 hours, provided the wound is stable. The patient is restricted to non-weight-bearing or toe-touch weight-bearing (maximum 20 lbs) for the first 8 to 12 weeks, depending on the severity of the comminution and the radiographic evidence of bone healing.
At the 6-week mark, progressive resistance exercises for the quadriceps and hamstrings are introduced. Full weight-bearing is generally permitted between 10 and 12 weeks postoperatively, correlated with clinical absence of pain and radiographic consolidation of the fracture lines. Advanced functional rehabilitation, focusing on proprioception and sport-specific movements, is initiated at 4 to 6 months.
Summary of Key Literature and Guidelines
The paradigm shift towards direct posterior approaches for specific tibial plateau fracture patterns is strongly supported by recent orthopedic trauma literature.
Lobenhoffer et al. (2004) revolutionized the modern approach by demonstrating that the posteromedial approach allows for direct visualization and mechanically superior buttress plating of posteromedial fragments without the morbidity of extensile midline posterior approaches. Their work established the posteromedial approach as the standard of care for medial shear injuries.
Carlson (2005) expanded on this by detailing the dual-incision posterior approach for bicondylar fractures with posterior comminution, proving that accessing both the posteromedial and posterolateral columns directly yields superior articular reduction compared to traditional anterior approaches.
Furthermore, biomechanical studies by Bhattacharyya et al. and others have definitively shown that anteriorly placed lag screws are insufficient for resisting the vertical shear forces exerted on a posterior coronal fracture during knee flexion. Posterior buttress plating provides optimal biomechanical stability, preventing fragment subsidence and posterior subluxation of the knee.
The integration of fibular osteotomies, as described by Yu et al., has further refined the posterolateral approach, providing surgeons with a reliable method to visualize the most challenging quadrant of the tibial plateau. Collectively, these advancements underscore the necessity for orthopedic surgeons to master the posterior approaches to effectively manage the full spectrum of tibial plateau trauma.
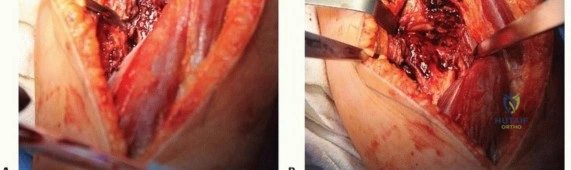
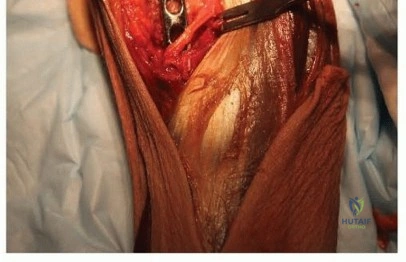
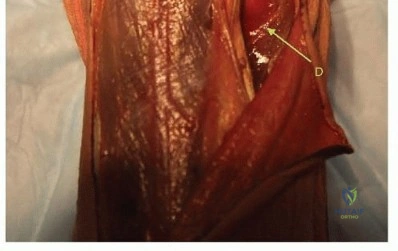
Clinical & Radiographic Imaging