Tibial External Fixation: An Intraoperative Masterclass for Trauma Stabilization

Key Takeaway
This masterclass guides orthopaedic fellows through tibial external fixation, covering indications for open and closed fractures, detailed surgical anatomy, and meticulous preoperative planning. We'll execute the procedure step-by-step, emphasizing precise pin insertion, frame assembly, and critical intraoperative decision-making. Learn to manage common pitfalls and optimize postoperative care for successful patient outcomes in complex trauma.
Comprehensive Introduction and Patho-Epidemiology
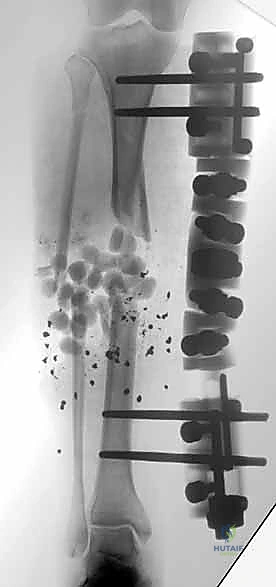
Tibial external fixation represents a cornerstone in the armamentarium of the modern orthopaedic trauma surgeon. The tibia, by virtue of its precarious subcutaneous anteromedial border and its role as the primary weight-bearing pillar of the lower extremity, is uniquely susceptible to high-energy trauma, severe soft tissue degloving, and open fractures. The evolution of external fixation—from the early rudimentary frames of Parkhill and Lambotte to the highly modular, biomechanically optimized carbon-fiber systems of today—reflects our deepening understanding of fracture mechanobiology. This procedure is not merely a method of skeletal stabilization; it is an active intervention in soft tissue resuscitation, allowing the traumatized limb to survive the acute phase of injury while mitigating the systemic inflammatory response.
The patho-epidemiology of tibial diaphyseal and periarticular fractures necessitates a nuanced approach to stabilization. High-energy mechanisms, such as motorcycle collisions or pedestrian-versus-auto accidents, impart massive kinetic energy to the limb. This energy transfer results in comminuted fracture patterns, profound periosteal stripping, and extensive microvascular thrombosis within the surrounding muscular envelope. In these scenarios, immediate definitive internal fixation (such as intramedullary nailing or plate osteosynthesis) introduces a "second hit" to the already compromised soft tissues, drastically increasing the risk of deep infection, wound breakdown, and osteomyelitis. External fixation circumvents this by providing rigid skeletal stability through percutaneous pin placement, entirely bypassing the zone of injury.
Furthermore, the concept of Damage Control Orthopaedics (DCO) relies heavily on the rapid application of external fixators. In the polytraumatized patient presenting with the "lethal triad" of coagulopathy, hypothermia, and acidosis, prolonged surgical times for definitive fixation are contraindicated. External fixation allows for rapid, life-saving stabilization of long bone fractures, stemming medullary blood loss, reducing pain, and facilitating nursing care and pulmonary toilet in the intensive care unit. Once the patient’s physiological parameters have normalized and the systemic inflammatory response syndrome (SIRS) has abated, the external fixator can be safely converted to definitive internal fixation.




Detailed Surgical Anatomy and Biomechanics
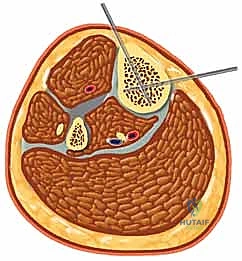
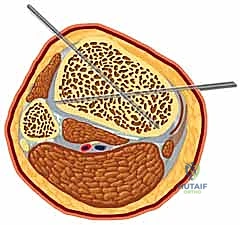
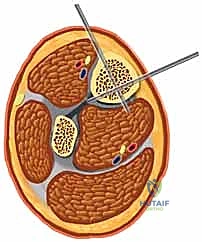
A profound mastery of the tibial cross-sectional anatomy is the absolute prerequisite for safe external fixation. The tibial diaphysis is essentially a triangular tubular structure, bordered by distinct muscular compartments that house critical neurovascular bundles. The primary safe zone for pin placement lies along the subcutaneous anteromedial face of the tibia. This surface is devoid of muscular coverage from the tibial tubercle down to the medial malleolus. However, the surgeon must remain acutely aware of the structures lying immediately adjacent to the bone, particularly when placing pins in a multiplanar or divergent configuration to increase construct stability.
The anterior compartment, containing the tibialis anterior, extensor hallucis longus, and extensor digitorum longus, also houses the deep peroneal nerve and the anterior tibial artery. These structures lie intimately against the interosseous membrane and the lateral cortex of the tibia. Pins placed too laterally or those that plunge excessively through the lateral cortex risk catastrophic injury to this neurovascular bundle, potentially resulting in an ischemic foot or an irreversible foot drop. Similarly, the lateral compartment contains the superficial peroneal nerve, which transitions from deep to superficial in the middle to distal third of the leg, making it highly vulnerable to percutaneous pin insertion if the safe zones are violated.
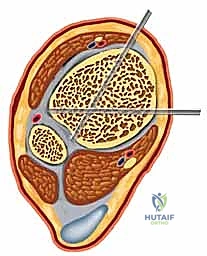
The posterior compartments present their own distinct hazards. The deep posterior compartment, containing the tibialis posterior, flexor digitorum longus, and flexor hallucis longus, protects the tibial nerve and the posterior tibial artery. These vital structures run directly posterior to the tibial diaphysis. Over-penetration of a Schanz pin through the posterior cortex by even a few millimeters can tether, lacerate, or compress these structures. Therefore, bicortical purchase must be achieved with meticulous precision, ensuring the pin tip just engages the far cortex without protruding dangerously into the posterior muscular envelope.
From a biomechanical standpoint, the stability of an external fixator construct is dictated by several modifiable variables. The stiffness of the frame is proportional to the fourth power of the pin radius; thus, increasing the pin diameter from 4.0 mm to 5.0 mm drastically increases the rigidity of the construct. However, pin diameter must not exceed one-third of the bone's diameter to prevent creating a stress riser and subsequent iatrogenic fracture. Construct stability is further enhanced by maximizing the spread of pins within each major bone fragment (near-near, far-far configuration), decreasing the bone-to-bar distance, and utilizing multiplanar pin configurations or double-stacked longitudinal bars when managing highly unstable or comminuted fractures.


Exhaustive Indications and Contraindications
The indications for tibial external fixation are broad, encompassing both acute trauma management and delayed reconstructive procedures. In the acute trauma setting, the most absolute indication is the presence of an open tibial fracture with severe soft tissue compromise, specifically Gustilo-Anderson Grade IIIB and IIIC injuries. In these scenarios, the risk of deep infection following immediate internal fixation is unacceptably high. The external fixator provides the necessary skeletal stability to protect microvascular repairs, facilitate serial debridements, and support eventual soft tissue coverage (such as free tissue transfer or rotational flaps) without introducing foreign material into the contaminated medullary canal.
Another critical indication is the temporization of high-energy periarticular fractures, such as complex tibial plateau (Schatzker V and VI) and distal tibial pilon fractures. These injuries are typically accompanied by massive soft tissue swelling, fracture blisters, and a high risk of compartment syndrome. Attempting open reduction and internal fixation (ORIF) through this compromised soft tissue envelope frequently leads to catastrophic wound dehiscence and deep infection. A joint-spanning external fixator (e.g., femur-to-tibia or tibia-to-foot) applied via the principles of ligamentotaxis restores length, alignment, and rotation while allowing the soft tissues to rest and recover over a period of 10 to 21 days before definitive ORIF is safely undertaken.
Contraindications to external fixation are relatively few but must be carefully considered. Absolute contraindications are rare in the setting of life-saving damage control orthopaedics. However, relative contraindications include patients with severe, uncorrectable coagulopathies where percutaneous pin placement might lead to uncontrollable compartment bleeding. Additionally, patients with profound osteopenia or metabolic bone disease may lack the cortical density necessary for adequate Schanz pin purchase, leading to premature pin loosening and loss of reduction. In such cases, alternative strategies like careful splinting, traction, or augmented fixation techniques must be employed.
Furthermore, external fixation is generally contraindicated as a definitive treatment modality in non-compliant patients who are unable or unwilling to adhere to strict pin site care protocols. The success of an external fixator relies heavily on meticulous postoperative care to prevent pin tract infections, which can rapidly progress to osteomyelitis or necessitate premature frame removal. In patients with severe psychiatric disorders or those lacking a reliable support system, the risks of long-term external fixation may outweigh the benefits, prompting the surgeon to seek alternative, fully internal methods of stabilization once the acute physiological crisis has resolved.
| Category | Specific Indications | Relative / Absolute Contraindications |
|---|---|---|
| Trauma / Soft Tissue | Gustilo IIIB/IIIC Open Fractures, Evolving Compartment Syndrome, Severe Crush Injuries | Healthy soft tissue envelope amenable to immediate intramedullary nailing |
| Polytrauma | Damage Control Orthopaedics (ISS > 16), Hemodynamic instability, "Lethal Triad" | Stable patient with isolated injury (relative contraindication for temporary ex-fix) |
| Periarticular | High-energy Pilon/Plateau fractures with severe swelling (Temporization) | Simple articular fractures with minimal swelling |
| Patient Factors | Need for rapid mobilization/ICU care, Burns over the affected limb | Severe non-compliance, inability to perform pin care, profound osteopenia (relative) |




Pre-Operative Planning, Templating, and Patient Positioning
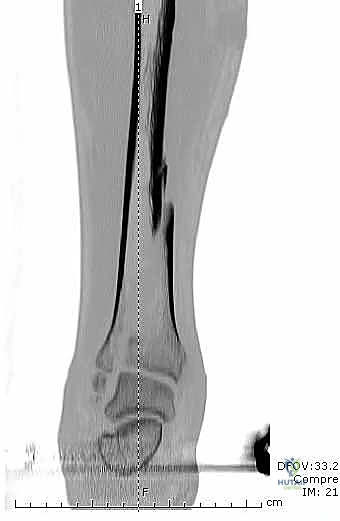
Thorough preoperative planning is the bedrock of a successful external fixation procedure. The process begins with exhaustive imaging. Standard orthogonal anteroposterior and lateral radiographs of the entire tibia, including the knee and ankle joints, are mandatory. These images must be scrutinized not only for the primary fracture pattern but also for occult non-contiguous fractures, coronal or sagittal plane deformities, and the extent of comminution. In the setting of periarticular injuries, a preoperative computed tomography (CT) scan is highly recommended, even if the initial plan is merely temporary spanning fixation. The CT scan provides invaluable three-dimensional data regarding articular impaction and fracture line propagation, which dictates safe zones for pin placement to ensure that Schanz pins do not inadvertently propagate intra-articular fracture lines.
Templating, while less formalized than in arthroplasty, is equally critical. The surgeon must mentally construct the frame architecture before making the first incision. This involves determining the optimal pin diameter (typically 5.0 mm or 6.0 mm for the adult tibia), the number of pins per segment (a minimum of two, ideally three in the diaphysis), and the required length of the carbon fiber or radiolucent connecting rods. The surgeon must also decide whether the frame will be joint-spanning or non-spanning. If spanning a joint, the position of immobilization must be carefully planned—for instance, the ankle should be fixed in neutral dorsiflexion to prevent debilitating equinus contractures, while the knee is typically fixed in slight flexion (10-15 degrees) to relax the posterior neurovascular structures and facilitate patient positioning in bed.
Patient positioning in the operating theater must facilitate unrestricted access to the limb and seamless fluoroscopic imaging. The patient is typically positioned supine on a fully radiolucent Jackson table or a standard operating table with the affected limb resting on a radiolucent cantilever board. A well-padded bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, bringing the patella and the tibial crest pointing directly towards the ceiling. This maneuver is crucial for achieving true anteroposterior fluoroscopic views without constantly rotating the C-arm or the patient's leg.
The C-arm fluoroscope should be positioned on the contralateral side of the injury, entering perpendicular to the operating table. The monitor must be placed in the surgeon's direct line of sight. Prior to prepping and draping, a "dry run" with the C-arm is highly recommended to ensure that perfect AP and lateral views of the entire tibia, from the knee to the ankle, can be obtained without obstruction from the table pedestal or other equipment. The limb is then subjected to a meticulous surgical scrub, often requiring extensive irrigation and debridement of open wounds prior to the formal application of the external fixator.





Step-by-Step Surgical Approach and Fixation Technique
The surgical technique for tibial external fixation demands meticulous attention to soft tissue handling and precise osseous targeting. The procedure begins with the identification of safe corridors for pin insertion. For a standard diaphyseal fracture, pins are typically placed along the anteromedial face of the tibia. A 1-centimeter longitudinal stab incision is made through the skin. It is imperative to avoid transverse incisions, as these create undue tension on the skin edges once the pins are in place, leading to necrosis and subsequent pin tract infections. Following the skin incision, a blunt hemostat is used to bluntly dissect down to the periosteum, spreading parallel to the longitudinal axis of the limb. This blunt dissection sweeps away small subcutaneous nerves and veins, minimizing iatrogenic injury.
Once the periosteum is reached, the use of a tissue protection sleeve is absolutely non-negotiable. The sleeve is inserted through the incision and seated firmly against the anterior cortex of the tibia. This sleeve serves a dual purpose: it prevents the surrounding soft tissues (muscles, nerves, vessels) from winding around the rapidly spinning drill bit, and it acts as a heat sink. Thermal necrosis of the bone during drilling is a primary cause of premature pin loosening and ring sequestrum formation. To further mitigate this, a sharp drill bit must be used, and the drilling should be performed in a pulsatile manner with copious cold saline irrigation directed down the drill sleeve. Both cortices must be penetrated, and the surgeon should feel a distinct "give" as the drill breaches the far cortex.
After pre-drilling, the Schanz pin is inserted. While self-drilling, self-tapping pins are available, pre-drilling the near cortex is highly recommended in the dense diaphyseal bone of the tibia to prevent excessive torque generation and micro-fracturing of the cortex. The pin is advanced under fluoroscopic guidance until the threads fully engage the far cortex. The tip of the pin should protrude no more than 1 to 2 millimeters beyond the posterior cortex. Excessive protrusion risks tethering the posterior musculature or, catastrophically, lacerating the posterior tibial artery or tibial nerve. This process is repeated until at least two, preferably three, pins are placed in both the proximal and distal main fracture fragments.
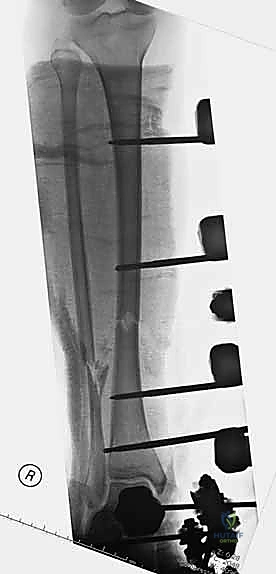
Once all pins are securely seated, the frame assembly begins. Pin-to-bar clamps are slid onto the Schanz pins, and a rigid connecting rod (carbon fiber or radiolucent aluminum) is passed through the clamps. At this stage, the clamps are left slightly loose to allow for fracture reduction. Reduction is achieved through a combination of manual longitudinal traction, manipulation of the pins as "joysticks," and the use of temporary reduction clamps if necessary. Fluoroscopy is utilized to confirm acceptable length, alignment, and rotation. Once the reduction is satisfactory, the clamps are systematically tightened. For highly unstable fractures, a second connecting rod can be added (double-stacking) to drastically increase the bending and torsional stiffness of the construct. The final step involves meticulously checking skin tension around all pin sites; any tethered skin must be released with a scalpel to prevent necrosis.










Complications, Incidence Rates, and Salvage Management
Despite its utility, tibial external fixation is fraught with potential complications, the most ubiquitous being the pin tract infection. The incidence of pin site infections varies widely in the literature but is generally reported between 10% and 30%. These infections are classified using systems such as the Checketts-Otterburn classification, ranging from minor soft tissue inflammation (Grade 1) to deep osteomyelitis necessitating pin removal and bone debridement (Grade 6). The majority of minor pin tract infections can be successfully managed with local wound care, chlorhexidine washes, and a short course of oral antibiotics covering common skin flora (e.g., first-generation cephalosporins). However, failure to aggressively manage early infections can lead to premature pin loosening, loss of construct stability, and the need for complex salvage procedures.
Loss of reduction and subsequent malunion or nonunion represent another significant complication profile. Because external fixators are inherently load-sharing devices, excessive rigidity can shield the fracture from the mechanical stress necessary for secondary bone healing (callus formation), leading to atrophic nonunion. Conversely, a construct that is too flexible may result in hypertrophic nonunion or progressive angular deformity. Regular radiographic surveillance is critical. If delayed union is suspected, the surgeon may employ "dynamization"—the deliberate loosening of the frame along the longitudinal axis to allow axial micromotion and stimulate osteogenesis. If nonunion persists, salvage management typically involves removal of the external fixator, a "pin holiday" (a period of splinting or casting to allow pin tracts to heal), followed by definitive intramedullary nailing or plate osteosynthesis with bone grafting.
Iatrogenic neurovascular injury is a devastating, albeit less common, complication, occurring in roughly 1% to 3% of cases. As detailed in the anatomy section, the deep peroneal nerve, anterior tibial artery, and posterior neurovascular structures are at highest risk. Injury usually results from a failure to utilize blunt dissection, neglecting the use of a tissue protection sleeve, or over-penetration of the far cortex. If a vascular injury is recognized intraoperatively, immediate consultation with a vascular surgeon for exploration and repair is mandatory. Neurological injuries, such as an iatrogenic foot drop, require careful documentation, removal or repositioning of the offending pin, and potentially nerve exploration if continuity is in question. Furthermore, the pins themselves can act as a nidus for secondary compartment syndrome, particularly if placed through tight fascial compartments without adequate release.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Pin Tract Infection | 10% - 30% | Meticulous insertion technique, avoiding thermal necrosis, strict post-op pin care | Oral antibiotics, local wound care; pin removal and debridement if loose or deep infection |
| Loss of Reduction / Malunion | 5% - 15% | Biomechanically sound frame construction, double-stacking bars for unstable patterns | Frame adjustment, dynamization, or conversion to internal fixation |
| Delayed Union / Nonunion | 5% - 10% | Avoiding excessive gap at fracture site, timely dynamization | Ex-fix removal, "pin holiday", conversion to Intramedullary Nail with bone grafting |
| Neurovascular Injury | 1% - 3% | Strict adherence to safe zones, mandatory use of tissue protection sleeves, bicortical control | Immediate pin removal/repositioning, vascular/nerve exploration and repair |